“Urgency” is defined in the Oxford English Dictionary as “importance requiring swift action”. But there is also a motto: “less haste more speed”. Or even, “slowly, slowly, catch your monkey”.
The 47 million or so people living with dementia, I feel, deserve better.
It might seem attractive to summarise the whole motherhood and apple pie approach with: “care for today, and cure for tomorrow.” And, indeed, prevention of the dementias is big business also too. But this is at risk of neglecting the concerns and expectations of people currently living with dementia.
People with dementia don’t form a ‘homogeneous’ group – not least because they are so many of them. Like any group of individuals, ranging from athletes to taxi-drivers, they all have different backgrounds, communities and expectations about the future. Notwithstanding that, it’s essential to listen to them.
The way in which you do this is, arguably, not through single people on large panels with diverse agendas. People living with dementia who can organise their own social movement are able to advance their own agenda. This might conflict potentially with the agenda of ‘others’. These ‘others’ may indeed have been people who have traditionally been thought to speak on behalf of people with dementia: like doctors, academics, carers or even politicians.
The sense of urgency for people with dementia to take their stories onto the world stage has never, in fact, been greater. This is in, no sense, a “false urgency”. In other words, this crisis has not been fabricated out of nowhere. But one cannot be blasé about what this crisis is. It’s the issue that there are 47 million people in the world who have ultimately received a diagnosis of dementia. They are actual people, with friends and family, who have their own needs. Many of these needs remain ‘unmet’.
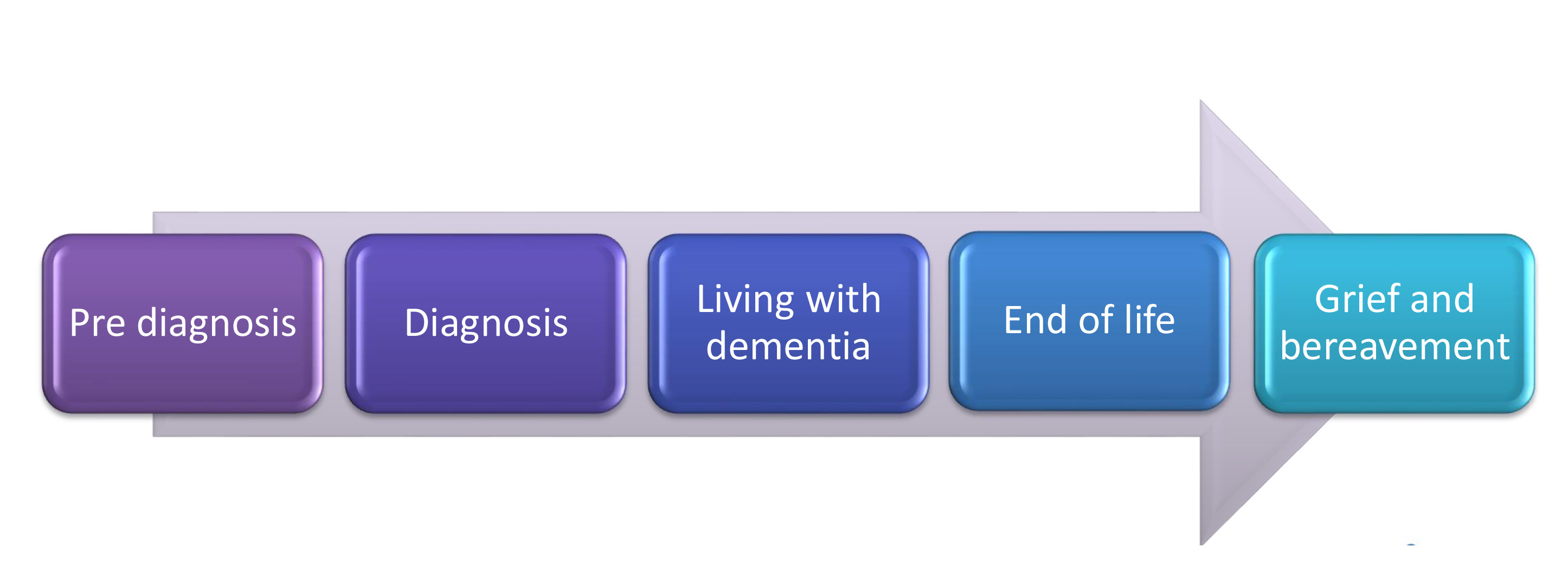
Sometimes the diagnosis is given brilliantly. Sometimes it’s not. Chris Roberts, living with a mixed vascular and Alzheimer’s dementia in Wales, describes how he was given his diagnosis in a loud office one afternoon, and there suddenly came a knock on the door with someone peering round and saying “Can you hurry up please?” A diagnosis of dementia is in effect given to the person with the dementia, but also his or her surrounding network. That person therefore needs to be ‘prepared’ for the diagnosis, and be supported after the diagnosis.
It has become traditional for the crisis to be couched in purely economic terms. And this added ‘cost’ becomes a ‘colossal burden’ and the such-like, and invariably accompanied by loaded terminology such as “tidal wave” and “tsunami”. This ‘shock doctrine’ is nothing new. Naomi Kline discusses the phenomenon brilliantly how ideology has been triumphantly forced upon people in the wake of ‘shocks’ such as Hurricane Tsunami or ‘the War on Terror’. Politically, everyone likes an ‘enemy’, and enemies come and go (such as the currently tirade against ‘benefit scroungers’ in the United Kingdom). But framing people with dementia as a ‘cost’ or ‘burden’ is to ignore totally their value.
To give you an example, I was once chatting to someone over lunch at the Healthy Living Club in Southwark, London. He was telling me how he’d come from South America several decades ago as a cleaner. He is now living with early Alzheimer’s disease. This is probably the most common cause of dementia in the world, and in the United Kingdom, and it’s often heralded with changes in learning and short term memory. And yet his memory for the 1950s was immaculate. He went onto tell me his experiences from the 1950s, and how he had felt welcomed to England as an immigrant.
It’s no mean feat to have had charities lobby national governments to get dementia onto the world stage. The G8 dementia event was a remarkable success; and so were the legacy events. But many of us were left wondering what the precise ‘shock’ was. The shock appeared to be that there is no ‘cure’ for dementia still.
Wait a second. Is this really a shock? Is there really a cure for ‘the common cold’? Probably some of these common colds are caused by rhinoviruses, but one could easily decide that it’s not worth a mass inoculation program against this common cold because of resource implications.
The most common neurological presentation is headache. And yet it is completely unfeasible that a general practitioner in primary care would order a brain scan immediately for every cause of headache. Of course, there are some urgent causes of headache which would require immediate action, but that is different.
Take another symptom – the wheeze. Would a respiratory physician embark upon a CT scan of the chest with every example of wheeze? A wheeze will commonly require symptomatic treatment in primary care, for example from a ‘blue puffer’ (the salbutamol inhaler).
A cure for dementia might be promised by a concordat of governments by 2025, but in all honesty is a tall order. A cure for dementia does, in my opinion, though serve a very useful function – in giving hope. Hope is not to be discouraged in public policy in dementia at all. One can compare, perhaps, dementia to cancer. There may be about 100 different causes of dementia, as there are many different causes of cancer. Certainly, dementia does attract similar stigma to how cancer used to (“the big C”).
Cures for cancer are different. A brain tumour might be surgically removed. A cancerous growth in the breast or lung might be subject to medical or surgical therapy. But the major issue here is that there has never been one big ‘cure for cancer’. I suspect likewise there will never be one ‘big cure’ for dementia. For example, a few weeks ago, there was great news about the possible application of immunotherapy to treat malignant melanoma. Malignant melanoma is one, important, type of cancer; in the same way that a rapidly progressive Creutzfeld Jacob disease is one type of dementia.
Raising funds for research must have this degree of transparency. People should know what exactly they’re raising funds for. We could do with much greater funds for dementia (at all), compared to other conditions, say cancer. Dementia doesn’t attract this level of funding. And the funding for dementia cannot morally, I believe, be simply for drug discovery, whether that be for symptomatic treatment or an outright cure. Some of these funds must be allocated into what better dementia care might be, or how best to promote living better with dementia.
Talk to anyone living with dementia, and he or she will tell you that they don’t want to wait til 2025 for something to happen. Richard Taylor Ph.D., living with probable Alzheimer’s disease, once joked what significance 2020 might bring. Are we to get suddenly excited that we are about to discover a cure for dementia? Let’s face it the “cure for dementia” Pharma invariably talks about is really a cure for Alzheimer’s disease. Possibly, however, what is discovered in finding a cure for Alzheimer’s disease will end up being useful for other dementias such as frontotemporal dementia, some of them have very different molecular biology footprints such as diffuse Lewy body disease.
So, the sense of urgency created in the world events, with prominent leaders of Big Charity and government, was a vicarious one on behalf of Big Pharma. It is well known that Big Pharma have found it difficult to keep up momentum for research and development of ‘drugs for dementia’, when the track record has been so poor. Currently, in the UK there are few licensed drugs for dementia, and they do not slow progression of disease. While some who have experienced these drugs (directly or not), have described substantial effects, it’s readily conceded by many that these drugs do not normally have an effect lasting more than a few months.
It’s widely pointed out by some that the recent NHS reforms in England around 2012 probably cost about £3bn, and generated much anxst for staff within the health service. There is a very important rewiring of health and care services yet to be done. The political appetite for making a big deal of this change is zilch, and yet all main parties in England know it has to come at some time. The current Conservative Government in the UK, due to run from 2015-20, have pledged to develop activities within the “Better Care Fund”. The official Labour opposition party had wished to implement “whole person care”. It is recognised that the last thing the NHS would apparently need at the moment is a massive ‘top down reorganisation’. This is why many people refer to the need for an organic ‘bottom up reorganisation’.
One can quickly see how the ‘crisis’ in dementia has many ‘faces’. For example, many acute admissions in England are of elderly adults living with dementia. As such, many are not admitted with ‘an acute exacerbation of dementia’, in the same way one might be admitted with ‘an acute exacerbation of asthma’ or ‘an acute exacerbation of multiple sclerosis’. The system is clearly not functioning well if, once people with dementia have had a medical crisis seen to (such as acute pneumonia), they are left languishing in hospital because they cannot be discharged in a timely manner.
Also there’s a crisis which is entirely of the medical profession’s making. That is, the “selling” of the model that ‘we, Doctors, can diagnose your dementia, give you a drug for your symptoms, and possibly even arrest the development of your dementia”. I am proud to be regulated by the medical profession, so I’ll be the first to support my colleagues who are doing great work everyday. Some of them are even good friends of mine. But the medical model is profoundly bust.
That is, the drugs aren’t great. Some of the drugs even make things worse (certain types of drugs go down really badly in people with certain types of dementia). I said earlier that hope is a good thing. False hope, though, I strongly feel, is a bad thing. Not content with the relative lack of success of drugs for dementia in the last few decades, you can palpably feel the attention switching by Big Pharma to ‘new markets’. It is good marketing that will see the notion of ‘pre dementia’ win. That is, ”pre-dementia” is an idea that people with dementia go through an asymptomatic phase first for ages; and it’s in this time window one might be able to have good impact. This of course is a terrific idea IF such a phase were easily identifiable. Currently, despite huge amounts of effort with ‘biomarkers’, this phase has not been easily identifiable.
“Pre-dementia” might be biologically plausible in vascular dementia. Here, somebody with a high cholesterol, if the evidence points that way, might enter a dialogue with his or her own doctor about possibly a statin to reduce the risk of developing dementia. And this for the doctor might be a ‘quick fix’ – being seen to do something, in that attending a ‘Dementia Friends’ session might convince you you’ve had some sort of “training” in dementia even though you have simply attended one 45 minute information session.
A real crisis is that this is diverting scarce resources towards drugs where a fraction of the money could make a massive quality of life to people with dementia though other means. The “Alive Inside” film was a real eye-opener for many, inspirational in showing that many people living with dementia could ‘come alive’ at the sounds of familiar music.
The accusation is that this type of ‘intervention’, with a mp3 player, is simply a ‘gimmick’ and waste of money. The accusation that there is not a huge evidence base for such interventions makes me angry, as there has been a concerted effort across a number of decades not to invest in such research. And yet against all the odds, Jörn-Henrik Jacobsen, Johannes Stelzer, Thomas Hans Fritz, Gael Chételat, Renaud La Joie, and Robert Turner published a paper in June 2015 explaining how parts of the brain which were relatively unaffected in advanced Alzheimer’s disease happened to be parts of the brain which could be involved in the perception of musical memories.
So the true crisis is unfolding. The resources may be being spent in the wrong place. And also resources which could be used to improve people’s quality of life are not being spent. It is worth pausing for a moment how this ridiculous situation has come about. There has been an assumption that politicians, members of the medical profession, Big Pharma and Big Charity are all acting in the “best interests” of people living with dementia. And there’s no doubt for me that people within the medical profession, Big Pharma and Big Charity are all capable to providing ‘small gains’ in helping people with dementia, if that’s a single leaflet explaining what Alzheimer’s disease is, if that’s a drug that can help for a bit, or if that’s identifying the type of dementia accurately so that appropriate medical care can be anticipated.
The social movement from people living with dementia is about to hit policy like a ‘tidal wave’ of its own. Be scared. Be very scared. Such a movement has organised itself, in the form of the Dementia Alliance International, and is growing in presence. It is effective as a peer group, offering much support to one another. It is also effective as a campaigning group, getting the concerns of people living with dementia onto the world stage. Reams and reams have been written on social movements, even including within the NHS. I believe that many people fixate onto the turning of ‘communication’ into action without first spending time to articulate the actual problem first.
And here’s the precise problem. The current global policy is for the benefit of Big Pharma, academia researching topics relevant to Big Pharma, and Big Charity who also get financial sustainability from supporting this agenda. It purports to be for the benefit of people living with dementia, but it is a sophisticated marketing ploy where people living with dementia are necessary for achieving the statutory purpose of maximising shareholder dividend. Most medical professionals would not wish to define their ‘success’ in terms of money. Living for longer is certainly one valid NHS outcome, but so is improving quality of life. The primary driver for Kotter’s “8 change model” is to turn around failure into growth, but growth here in the NHS is different to that of a corporate.
The financial case for turning the juggernaut around that is policy to living better with dementia is that it potentially saves a lot of money in the long run. This could be as shown by the University of Southampton in their analysis of clinical specialist nurses called “Admiral nurses”. These nurses are able to stop medical problems before they gain ‘lift off’, and can help to reduce the volume of ‘avoidable admissions’. The economic case for this is, in fact, monumental.
But it’s also very much a moral one. None of the major stakeholders can afford to be ‘complacent’ about the situation which has arisen problematically now in global dementia policy. And yet this is exactly what a ‘long term plan’ might actually unwittingly encourage – effectively ‘doing nothing’ until judgment day in 2025.
It is now, I believe, time that we listen to the stories and experiences of people living with dementia – and act on them. There is a sense of urgency, but this is not to deny that this problem has brewing for a very long time. It’s essential that leaders from the world community of people living with dementia are identified fast. And they are given real power to allow this movement to shine, as John Kotter would have intended.