On February 23rd 2015, I travelled down with Chris Roberts and Jayne Goodrick to see Tommy Whitelaw speak at Goodmayes Hospital. Tommy had been invited by the @BHRUT_Dementia team.
We only just made it in time.
Chris gave an introduction. Chris Roberts (@mason4233), living well with a mixed dementia (Alz and vascular), had travelled from North Wales to Goodmayes Hospital especially.
Barking, Havering and Redbridge University Hospitals NHS Trust operates across two main sites at Queen’s and King George hospitals serving a population of around 700,000 from a wide range of social and ethnic groups, making it one of the largest acute hospital trusts in England.
I was very impressed by another introductory talk by Matthew Hopkins, the Chief Executive. Matthew (@M_J_Hopkins) has gone via Addenbrooke’s Hospital where I indeed was a junior house officer in general medicine on Prof Tim Cox’s firm.
I truly found Tommy’s talk inspiring. I know Tommy will have given the talk many times, but it gave it his all. It must be emotionally exhilarating for Tommy to retrace these steps.
What I particularly found inspirational about Tommy’s talk was how it will remind individuals in the NHS and care workforce what is important; care for real people rather than anonymous patients. I strongly believe in the notion of personhood, that everyone is fashioned by his or her past and present, and environment including relationships and wider environment.
“Person centred care” is a over-rehearsed phrase, but Tommy’s approach is one of great power.
I explained in my comment that I did not wish to bombard the event with policy. When members of the public think about the wider economy, they tend to be less interested in the mechanics behind the GDP figures, but more concerned how the economy might relate to a zero-hours contract or standard of living.
Similarly, I don’t think it’s helpful to be bogged down in a morass of policy detail. People are people.
But it does happen that Tommy does raise wider issues in general. Everyone has a life story for example. As Tommy explains, his mother had unmet needs; and the subtext here is that Joan did not want to go into residential care, so it is important to have her needs addressed.
Tommy did in the end find support from a medical consultant and a district nurse. Quite often whom you meet can totally alter the nature of your personal experiences about a situation.
And yet Tommy does embrace the wider 6Cs, currently English nursing police: care, compassion, competence, communication, courage, commitment.
Tommy would be the first to explain that he felt relatively under-prepared for the caring rôle he would ultimately take in looking after Joan; this is not unusual with many caregivers not thinking of themselves as ‘caregivers’, and often wondering whether they’re doing things right.
But people like Tommy, I feel, are not only doing things right but doing the right things. This means that Tommy is not just managing the situation with Joan, but he is showing true leadership.
The law looks behind the substance behind the name. That many thousands have given personal pledges for Tommy, including the Chief Nursing Officer Jane Cummings, means that Tommy has created a highly formidable social movement.
This is not just called a ‘social movement’. It is a social movement.
“Dementia Friends” is an initiative from the Alzheimer’s Society and Public Health England. In this series of blogpost, I take an independent look at each of the five core messages of “Dementia Friends” and I try to explain why they are extremely important for raising public awareness of the dementias.
There’s more to a person than the dementia.
In 1992, the late Prof Tom Kitwood founded Bradford Dementia Group, initially a side-line. Its philosophy is based on a “person-centred” approach, quite simply to “treat others in a way you yourself would like to be treated”.
A giant in dementia care and academia, I feel he will never bettered.
His obituary in the Independent newspaper is here.
Personhood is the status of being a person. Its importance transcends medicine, nursing, policy, philosophy, ethics and law even.
Kitwood (1997) claimed that personhood was sacred and unique and that every person had an ethical status and should be treated with deep respect.
A really helpful exploration of this is found here on the @AlzheimerEurope website.
Personhood in dementia is of course at risk of ‘paralyis by analysis’, but the acknowledgement that personhood depends on the interaction of a person with his or her environment is a fundamental one.
Placing that person in the context of his past and present (e.g. education, social circumstances) is fundamental. Without that context, you cannot understand that person’s future.
And how that person interacts with services in the community, e.g. housing associations, is crucial to our understanding of that lived experience of that person.
All this has fundamental implications for health policy in England.
Andy Burnham MP at the NHS Confederation 2014 said that he was concerned that the ‘Better Care Fund’ gives integration of health services a ‘bad name’.
It is of course possible to become focused on the minutiae of service delivery, for example shared electronic patient records and personal health budgets, if one is more concerned about the providers of care.
Ironically, the chief proponents of the catchphrase, “I don’t care who is providing my care” are actually intensely deeply worried about the fact it might NOT be a private health care provider.
Person-centered care is an approach which has been embraced by multi-national corporates too, so it is perhaps not altogether a surprise that Simon Stevens, the current CEO of NHS England, might be sympathetic to the approach.
Whole-person care has seen all sorts of descriptions, including IPPR, the Fabians, and an analysis from Sir John Oldham’s Commission, and “Strategy&“, for example.
The focus of the National Health Service though, in meeting their ‘efficiency savings’, has somewhat drifted into a ‘Now serving number 43′ approach.
When I went to have a blood test in the NHS earlier this week, I thought I had wandered into a delicatessen by accident.
But ‘whole person care’ would represent a fundamental change in direction from a future Government.
Under this construct, social care would become subsumed under the NHS such that health and care could be unified at last. Possibly it paves the way for a National Care Service at some later date too.
But treating a person not a diagnosis is of course extremely important, lying somewhat uneasily with a public approach of treating numbers: for example, a need to increase dementia diagnosis rates, despite the NHS patient’s own consent for such a diagnosis.
I have seen this with my own eyes, as indeed anyone who has been an inpatient in the NHS has. Stripped of identity through the ritualistic wearing of NHS pyjamas, you become known to staff by your bed number rather than your name, or known by your diagnosis. This is clearly not right, despite years of professional training for current NHS staff. This is why the campaigning by Kate Granger (“#hellomynameis”) is so important.
It is still the case that many people’s experiences of when a family relative becomes an inpatient in the National Health Service is a miserable one. I have been – albeit a long time ago – as a medical student on ward rounds in Cambridge where a neurosurgeon will say openly, “He has dementia”, and move onto the next patient.
Together with the other four messages, that dementia is caused by a diseases of the brain, it’s possible to live well with dementia, dementia is not just about losing your memory, dementia is not part of normal ageing, the notion that there’s more to a person than the dementia is especially important.
And apart from anything else, many people living with dementia also have other medical conditions.
And apart from anything else, many people living with dementia also have amazing other skills, such as cooking (Kate Swaffer), fishing (Norman McNamara), and encouraging others (see for example Chris Roberts’ great contributions to the community.)
References
Kitwood, T. (1997).Dementia reconsidered: the person comes first. Open University Press.
Sue Stephen, one of the founding members of the Dementia Alliance International (DAI), spoke about how she came to be diagnosed with PCA.
This is one of the latest additions on their blog, which I strongly recommend. The DAI is an unique group of individuals with a strong sense of solidarity, who live with one of the various types of dementia.
“I had been noticing myself for the last few years that I was having visual issues… very bad glaring.. when I tried to read..”
She put it down to stress, but she still went ‘to get [my] eyes tested.’
And this went on for a few years. Interestingly, she reports this delay in diagnosisas rather typical for many people finding a diagnosis of PCA.
Tests for dementia of the Alzheimer type, typically initially shown up by problems in short term learning and memory, were negative.
When she was eventually given a diagnosis, she was told, “That’s it. There’s nothing I can do. Here’s a prescription for Aricept. See you in six months.”
But she described being shocked, and she had no idea what PCA is/was.
“I lost all certainty in my life. How do I make decisions in my life?”
She then sat on her month doing ‘research’, but reported ‘three wonderful things’ which came out of her research.
She found a list of symptoms which matched what she had been experiencing. “That was really good”. This enabled her to see her GP who then went referred her onto more suitable specific tests, confirming the diagnosis.
That’s one of the slight paradoxes about the way we approach a fellow citizen of ours living with a dementia. Nobody wants to be defined by any medical conditions they live with. They do not wish (rightly) to consider themselves as a collection of diagnoses.
But it is often reported by people living with conditions how it can be both a blessing to know what might happen but also a burden to know something might happen, with this information resulting from a clinical diagnosis.
She then reported discovering the work of Sir Terry Pratchett, who is living well with PCA, still writing books.
A third thing which she reports is finding a group of people on Facebook of people with posterior cortical atrophy. It’s a closed group where people can share in private “scenarios”.
“I could see in the future what symptoms might be. I look at symptoms, and I think if this happened to me, what could I do now to help?”
Stephen reports sharing these stories really helped.
Terry Pratchett went to see other people living with posterior cortical atrophy in 2010, a form of dementia.
Pratchett is an example of an individual who has shown that it is possible to live well with dementia.
Pratchett admitted he was apprehensive about the meeting, as he said it was like ‘seeing into the future’.
One person in the meeting, “Anything coming through the postbox, I can’t read. Susan has to do everything from cutting my nails to putting my shoes on. This disease.. or whatever you call it, changes your perspective.”
“It didn’t happen – it evolved.”
Pratchett though admitted despite his fears he enjoyed the meeting.
“I can see why people enjoy meeting up”
He had dinner with Graham Doggett, who is an 70 year-old author, and academic who has written books about quantum chemistry, and his wife.
“Susan is the gardener. If I help her, I can never find the wretched branches in the air to prune. They disappear.”
“I was doing computing since 1959. That’s gone.”
“I used to play piano up to grade 7. Gone.”
“Reading, writing, gone gone”.
When the term ‘living well with dementia’, one of the main disclaimers on that is that the person living with one of the dementias will have their life before to compare their experience to.
And this is bound to impact upon one’s own personal perception of living with dementia. Unless you bother to find out about the past of a person, in relation to his environment, you will not be able to understand his or her world.
The symptoms of PCA can vary from one person to the next and can change as the condition progresses.
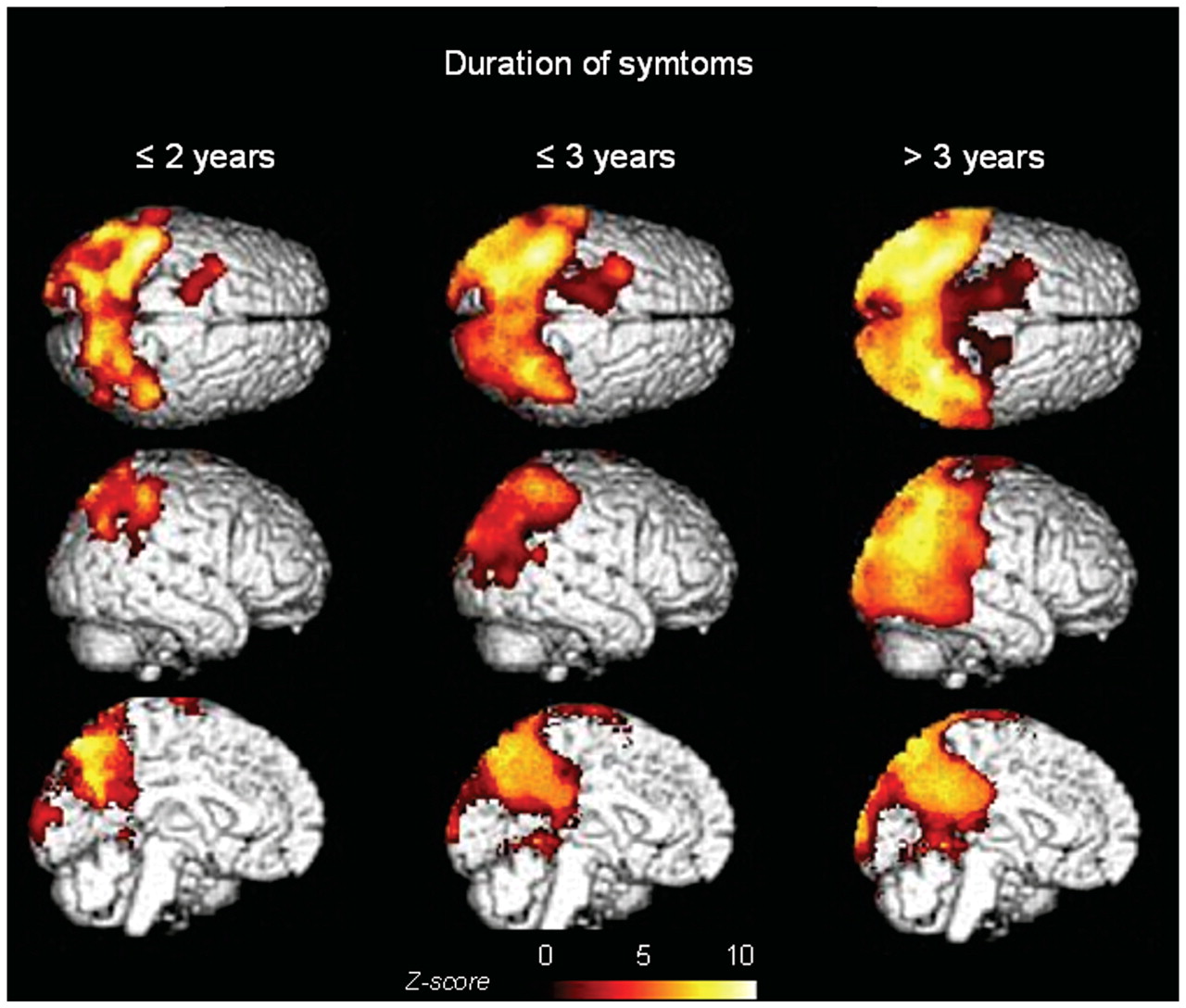
The most common symptoms are consistent with damage to the part of the brain at the back of the head, an area responsible for processing visual information.
Consistent with this process are slowly developing difficulties illustrating its slow and progressive nature due to a disease of the brain.
Now you’re even able to follow it using sophisticated ‘imaging’ of the brain.
These difficulties include visual tasks such as reading a line of text, judging distances, and distinguishing between moving objects and stationary objects.
Other symptoms include an inability to perceive more than one object at a time, disorientation, and difficulty maoneuvering, identifying, and using tools or common objects.
Some people can experience hallucinations.
Yet further symptoms can include difficulty performing mathematical calculations or spelling, and many people with PCA experience anxiety, possibly because they know something is wrong.
In the early stages of PCA, most people do not have markedly reduced memory, but memory can be affected in later stages.
This illustrates how this particular dementia is not just about memory.
Both Stephen and Pratchett demonstrate by a country mile while there are more to people than their dementias.
If you’d like to find more about dementia, you can do a short 45 minute session close to where you live in England (and now in other parts of the UK). The initiative is run by the Alzheimer’s Society, but is a Public Health England initiative. To find out more about this initiative called “Dementia Friends”, please go to their website.
There’s more to this initiative than the badge you’ll receive in the process, but this initiative is all about improving understanding in the general population about the dementias. I hope you will wish to learn more.
People with PCA are are at risk of being let down by ‘traditional dementia support groups’.
That is partly because they are younger and face different challenges, and partly because the activities offered in day centres puzzles, large-font books—are visual and thus actively unhelpful for people with PCA.
PCA is not new to the research community.
Already in 1902, the Czech psychiatrist Arnold Pick mentioned a woman’s inability to see and grab a lit candle held in front of her face in his essay “Ueber eine eigenthuemliche sehstoerung senile dementer,” Jahrbuecher f. Psychiatrie u. Neurol., see excerpt.
Several attempts at defining criteria for diagnosis exist.
The neurologist Frank Benson at the University of California, Los Angeles, coined the term while describing the pattern of symptoms in five patients (Benson et al., 1988).
Later, Mario Mendez, also of University of California and San Francisco proposed clinical diagnostic criteria arguing that PCA is its own syndrome, not simply Alzheimer’s disease with visual symptoms (Mendez et al., 2002).
The English dementia strategy is mindful of the needs to develop communities supportive of the needs of people living with PCA, of the need for high quality research research into PCA, and to think how people living with PCA can be best supported professionally and personally.
It’s not only people with posterior cortical atrophy who experience problems with vision, however. This is very important to be aware of.
We are continually being reminded that ‘money does not grown on trees’. Funds are said to be ‘unsustainable’. You’ve heard it all before.
And yet there is potentially a scanty evidence base for certain initiatives in the NHS, where every penny does count. For every contract awarded, there’s an equal and opposite contract which has not been awarded. Recent problems in health policy to do with the English NHS shows a genuine problem with trust, whether it’s implementation of the Health and Social Care Act (2012) or “Care Data”.
As entities get bigger, their presentation tends to get slicker. With economies of scale, things can be done more ‘efficiently’. The overwhelming danger is that everything becomes alarmingly centralised, actually deprofessionalising and lowering standards of what is being delivered. It can become all too easy to run courses, get the facilitator to run the DVD and read a pre-prepared script, and, even if the end-user doesn’t pay for it, the taxpayer does.
But the culture in the NHS is not right. People are scared to ‘speak out safely’ against practices which they do not agree with, even if the reasons are perfectly sound. The pattern of behaviour at people who have criticised, with good intentions, in healthcare has tended to follow a similar pattern: ignore – discredit – attack – ignore – ostracise. But increasingly as the same grant winners tend to get more grants, as they built up a dominant presence and brand loyalty, they are in a position to flex litiginous muscles.
It all has an “Emperor’s New Clothes” feel about it. “The Emperor’s New Clothes” is a famous short story by Hans Christian Andersen about two weavers who promise an Emperor a new suit of clothes that is invisible to those unfit for their positions, stupid, or incompetent. When the Emperor parades before his subjects in his new clothes, a child cries out, “But he isn’t wearing anything at all!” And that’s the position we’ve reached with various prestigious brand leaders.
And yet it is fundamentally an anethema to the whole basis of personhood as conceptualised by Tom Kitwood. There is an increasing army of people who are quite horrified, like me, how personhood has become transformed into marketing shills and glossies in a standardised package corporate-feeling sort-of-way.
There’s certainly concern about how dementia training and person-centred approaches have become commercialised, in a way that would have made the late great Tom Kitwood shudder.
Kitwood’s approach was more conceptually and theoretically developed, and highlights the importance of the person with dementia rather than the disease process itself. Kitwood argues that people with dementia do not lose their personhood, but rather can be maintained through relationships with other people.
Thus, Kitwood defines personhood as ‘a standing or a status that is bestowed on one human being, by another in the context of relationship and social being’. Within person-centred care therefore, the personal and social identity of a person with dementia arises out of what is said and done with them.
In other words, it IS highly personal and individual.
Anyone who has worked in the NHS knows likewise that one junior doctor covering all the medical wards in a hospital and acute admissions is bound to be rushed off his or her feet. Any emergency room nurse facing the common situation of being ten patients behind will know exactly how stressful the job is, propelled by ‘efficiency savings’ the NHS “MUST” make to resolve the “funding gap”.
A concerning strand has emerged therefore of marketising and selling compassion. This is a very strange concept as it implies that compassion in some way can be “imposed”.
In October 2013, it was mooted that unregistered care support workers wouldsoon have to obtain a “care certificate” to show they have completed basic training before they are allowed to work unsupervised, the government has announced.
Health minister Earl Howe has revealed that Health Education England would lead work on developing a certificate of fundamental care, as recommended by Camilla Cavendish in her review of regulation and training in the sector earlier this year.
He said it was too early to know what the care certificate would look like, but said it would build on the national minimum training standards published by Skills for Care and Skills for Health in March, as Cavendish recommended.
This policy plank is incredibly difficult, for fear that the implication is that certain care staff are deliberately ‘withholding’ compassion. But it is patently more of a problem that junior care and nursing staff are in certain cultures finding it very difficult to speak out against unsafe levels of staffing cuts (a common strand in the dangerous ‘Keogh trusts’.)
The way some commissioners are tending to behave is fair-and-square a ‘tick box’ culture. What are we doing today?
“C” for compassion
And “D” for dementia friendly communities.
A Dementia Friends Champion is a volunteer who encourages others to make a positive difference to people living with dementia in their community. They do this by giving them information about the personal impact of dementia, and what they can do to help.
It is not supposed to be specialist in training for dementia.
But it can be argued that the whole set-up of Dementia Friends and Dementia Champions gives their organisers an advantage. It must have a business model somewhere, and presumably the Alzheimer’s Society is working with the current Government to deliver this initiative? Virtually every newspaper article about dementia these days mentions ‘Dementia Friends’. Parliamentarians mention it. And yet there is no mention of other dementia societies, such as Alzheimer’s BRACE or Dementia UK. For every penny in one direction, a penny is lost in another direction.
A strange phenomenon is that you don’t need to have any particular experience or skillset to be a Dementia Friends Champion.
This level of standardised packaging of ‘a training’ therefore has two inherent problems. Firstly, it denies the whole ethos of Kitwood’s bestowment of personhood. Secondly, it lends itself too easily to a ‘tick box’ culture from commissioners who can say ‘they’ve done dementia’ in a race to the bottom. And people who’ve done the Dementia Friends often report a dubious relationship about whether it is or it is not the Alzheimer’s Society, parking aside the statement that “Dementia Friends is an Alzheimer’s Society” initiative at the bottom of the ‘Dementia Friends’ website.
If a charity is being supported by Government in delivering the Dementia Challenge, this should be made much much clearer. This is because the charity ‘market’ is itself being distorted. And furthermore with access to the media commercial endorsements can deprive others of media attention, while ‘picking winners’.
“Our high streets are set to become more dementia friendly following a commitment from major British businesses today (Friday 28 February).
Our high streets are set to become more dementia friendly following a commitment from major British businesses today (Friday 28 February). Argos, Homebase, Marks and Spencer, Lloyds Pharmacy and Lloyds Banking Group, backed by Health Secretary Jeremy Hunt, have committed to create over 190,000 Dementia Friends in shops and banks across the UK.”
Certainly the staff at the Alzheimer’s Society are brilliant, and totally devoted to the cause.
This was Ian McCreath today.
@legalaware some AS staff are DF champions (myself included) but all do so entirely on a voluntary basis and on our own time.
Dementia is clearly a ‘good market’, and so is ‘compassion’ despite inability of some people in being to define it properly.
Nobody is denying the rôle for both to be prominent planks in English dementia policy, but the public needs to have trust that these are all effective use of taxpayers’ money. People who’ve done thousands of home visits, albeit as unregistered dementia care workers, including carers and other careworkers, or even people living with dementia, will have qualms about people without any specialist training themselves of dementia raising dementia awareness.
We do need an honest debate about how effective these initiatives are, especially in relation to the ‘getting most of your buck’ idea. The system is open to abuse, with powerful people getting more powerful, as a result of who you can get to deliver your package fast and at the most competitive price.
I have always understood “living with dementia” to mean that that person carries on with life, knowing that there is an underlying medical phenomenon somewhere. To me, it’s exactly the same as living in recovery from alcohol dependence. If I were to have another alcoholic drink, I wouldn’t be able to stop drinking. It’s a pathological reaction. I view it in the same way that some people have an allergy to peanuts. I don’t actively think about not drinking all day – it’s just something that’s part of my life.
It did genuinely come as a surprise to me, however, that some individuals view ‘living with dementia’, as living with somebody close to them with a dementia. I respect this viewpoint, and it is clear that no offence is intended there as well.
I don’t know what a person living with dementia (in my sense of the phrase) “feels like”, in the same way philosophically I cannot know what he or she perceives as the colour red. But an attempt to understand what one of the dementias might be like for that person I believe is pivotal for care, consistent with Tom Kitwood’s seminal work on personhood. In this framework, your prime concern is the person (rather than patient) with one of many types of dementia. A person will be a ‘product’ of experiences unique to him or her, and his or her own physical health, and not just a sum of his or her chemical receptors in the brain.
For medical professionals, a diagnosis can operate at a number of levels. One is individual, pertaining to someone’s identity or concept of being ‘sick’. One can be institutional (in relation of that individual to clinicians, politicians or social movements). We have seen this year how some politicians have been clamouring for a slice of the dementia diagnosis action. One can be societal, which depends entirely on how diagnosis frames that particular entity. For example, society might view that a delayed diagnosis for a dementia, where there is no obvious reason for this delay, is simply unacceptable.
There are in theory four possible options. With a diagnosis, a person may find himself or herself with a ‘disease’ or ‘illness’that potentially could be cured or treated, ‘healthy’ or no illness (but subject to future monitoring), ‘at risk’ of developing a future disease, or an illness with no disease (something wrong but not fitting conventional protocols of medicine.)
But as Blaxter warned back in 1978, “The activity known as ‘diagnosis’s is central to the practice of medicine but is studied less than its importance warrants.”
A diagnosis is by no means a trivial issue. It has become powerful because of the close proximity in academic and practitioner circles between legal, insurance and medical jurisdictions.
A diagnosis can have important consequences. Those consequences might be “administrative”, allowing somebody to access resources in health care; it can “legitimise” sickness (or the rather perjorative notion of “deviance”); or can encourage research into the existing evidence base.
A person as a result of a diagnosis may adopt “a sick role”, after Talcott Parsons’ seminal work in 1951. This construct of ‘sanctioned deviance’ is not without its critics, who argue that this encourages a culture of blaming ‘the sick’.
For the purposes of the medical profession, a diagnosis can be seen as a diagnosis of a cure or treatment. Indeed, for many, the identification of a cure or treatment would contribute to diminishing the stigma associated with, or discrimination to the detriment of, a person with a diagnosis. These days, particularly for dementia perhaps, given arguably the lack of a robust cure or disease-modifying treatments for the most common form of dementia known as Alzheimer’s disease, having a diagnosis might be seen as enabling rather than labelling (after Marian Naidoo.)
Kate Swaffer, who has herself written candidly about her personal experiences of dementia, concludes her recent poem, “If they are not diagnosed with dementia…They cannot be living with it.”
“Some people have agreed vehemently with my opinion about the use (or mis-use) of the term ‘Living with dementia’ and others have disagreed just as strongly, while others have sought to question further, to look at themselves differently, or to question me. I too have sought to look at this topic through others’ eyes, to see it differently and from as many sides of the same coin as humanly possible.”
There is indeed more to this than immediately meets the eye. Take autism, for example.
Contrary to popular assumption, people diagnosed with so-called “mild forms of autism” often don’t fare any better in life than those with severe forms of the disorder. That’s the conclusion of a recent study that suggests that even individuals with normal intelligence and language abilities struggle to fit into society because of their social and communication problems.
In fact, people diagnosed with pervasive developmental disorder-not otherwise specified (PDD-NOS) are no more likely to marry or have a job than those with more disabling forms of autism, according that study.
There’s been a growing realisation that diagnostic criteria are not “gospel“, and a number of medical phenomena have seen a number of patient groups query this; these include myalgic encephalitis, B12 deficiency and Lyme Disease.
In the case of autism, such difficulties might be mitigated against by merging of pervasive developmental disorder into the autism spectrum. And a similar phenomenon is taking place for the reclassification of the dementias as “neurocognitive disorders” (of major and minor types.)
It can’t easily be denied though that some individuals find a diagnosis helpful in that such a diagnosis might help to make sense of the past, present, and future (see for example “midlifeguy”‘s experience here).
“”Time to change Wales” are doing amazing things and I am proud to say that I wear their end stigma badge everyday and am frequently asked about it. I am so passionate about stamping out stigma and discrimination against mental health that some days it’s literally all I can think about. I guess that’s why I set up my campaign Kim’s Voice, in memory of my late sister who committed suicide in 2009.”
Persons who have been given medical diagnoses have tended to find support from others who share similar experiences and there are instances of specific-issue health movements shaping medical practice and government policy. And it’s inevitably going to be the case that some diagnoses are contested, challenged and/or politicised. Indeed, diagnostic categories can, and often are, resisted or disputed.
Whether you happen to agree with Kate Swaffer, ironically, is personal to you, but it’s hard to deny that that poem throws up some important questions about identity and the way others perceive you.