I remember once being told that an “alcoholic” is uomebody who drinks as much alcohol as you, but somebody you don’t particularly like.
Culture has an odd way of inflicting labels on people it doesn’t particularly respect. This can be done for entirely political reasons – a need to place a ‘them against us’ division, like the term ‘benefit scroungers’ for people who cannot find gainful employment.
I remember when I went to the Alzheimer’s Show last year, and a senior consultant in psychiatry gave a talk on ‘challenging behaviours and BPSD’. I challenged him at the end for whom did he deem the behaviour challenging – for the person with dementia distressed, or for the professional who wanted a quiet shift?
I then shortly afterwards went to an evening of a drug company sponsored CPD session on frailty. The GP presenting the case study kicked off with the line ’83 y.o. demented F’. I asked the presenter to justify the use of the word ‘demented’ in his case study. He informed me it was about as pejorative, and equally inoffensive, as saying ‘wheelchair user’.
I don’t want to enter into a discussion about normative morality. That is way beyond the scope of this blogpost. But there comes a time when you simply can’t cope with the deluge of cultural impropriety.
Two events happened back to back only yesterday. For example, a friend of mine, in an otherwise good article in a tabloid, was called ‘Dementia sufferer’ in the title. A press release about a forthcoming BBC programme on cures and dementia was littered with the word ‘sufferer’.
But I have recently been doing a lot of work in education of dementia, and it shocks me how entrenched the BPSD dogma is. I simply don’t want teaching I am involved in with to perpetuate knowingly this misfeasance.
‘Person-centred care’ is a much used and abused term. But dealing with failures in communication with a person who lives with dementia but who is distressed is a more ethical (and cheaper) way of behaving, other than pimping money out at Big Pharma.
An individual who’s received a diagnosis of dementia has a right to be angry, agitated, anxious or depressed at conscionable behaviour from a carer or professional, for example. An individual who’s received a diagnosis of dementia is therefore entitled to feel emotions if provoked.
What this situation does not give professionals a right to do is to drug innocent people with dementia always to prescribe antipsychotics inappropriately as a ‘chemical cosh‘.
In parallel to the human right to live with dignity, found in the European Convention of Human Rights which we can all petition over in England and Wales if we are a signatory, irrespective of the Human Rights Act (1999), there’s an expectation that patients of the NHS are not subject to assault and battery from inappropriate medications.
Whilst many of us are saddened by the lack of clarity in the current Government assaulting the legislation over human rights, we also take some comfort in devolution. Scotland is a clear example of an administrative style in one country. Manchester has been another. Maybe with the election of Sadiq Khan in London today we may have another example of a devolved infrastructure, which can distance itself from Westminster, and act as a nestbed for the integration of health and social care?
Be in no doubt – it takes a long time to alter the directions of supertankers. Dementia Alliance International has been campaigning hard on this for a few years now, and as the only influential international stakeholder group run by people with dementia, many of us wish them well.
When I was doing my junior medical rotations, in preparation for the clinical examinations for the Royal Colleges of Physicians, there would always be the scary assessment of ‘communication skills’.
This is long before the time of the current #mynameis campaign in the NHS.
Having introduced yourself to the patient, one of the first things you’d be examined on is your exploration of the patient’s “beliefs, concerns and expectations.” The aim of the medical consultation was to prepare a management plan, given the time constraints, given these aspirations from the patient.
In reality, we all know the nonsense of being able to deal with all of a patient’s issues within a ten minute timeframe. People living with conditions, such as dementia, have had long time to reflect on the nature of their conditions and how impact on their lives.
The power imbalance in the doctor-patient relationship, I do not wish to deny, can potentially be a problem. For an example a medical patient’s wish to ‘live better with dementia’ can easily become a GP’s wish to solve a problem (s)he thinks (s)he can solve – like a modest improvement of memory through a drug.
For example, I violently object to Doctors seeing people as nameless entities, with no background, simply as a list of medical problems.
In life, I believe strongly we should actively seek out what people can do too.
Ultimately, I feel we are all persons, and that we become patients when we become ill. I think personhood is all about embracing a person’s past and present, and his or her relationships with everyone else; this should have been an aim of healthcare professionals all along.
I happen to be proud of being a ‘Dr’ only because I endured (so I perceived) quite a lot of stigma from being banned from the Medical Register during my problems consequent upon alcohol abuse. In fact, I deliberately avoided calling myself ‘Dr’ even though I knew I was perfectly entitled to, on the grounds of having completed a doctor of philosophy (“a real Doctorate”).
In hospitals, it can be useful also to be a ‘Dr’ to save a lot of time. I am only saying this as I have seen circular discussions on ‘abolishing hierarchies’ in the “new model NHS”, and I can say for a fact that I never had an ‘attitude’ from being any sort of Doctor. In hospitals, it can be useful for patients to differentiate yourself from other health professionals.
With being a Doctor comes a lot of baggage too, like always being on best behaviour 24/7 outside of your job, or not giving any advice to complete strangers despite people asking for advice. That is, rather, an honour of professional regulation.
But I feel that the term ‘person centred care’ requires explanation. If it is not patient centred, what else is the healthcare system revolved around?
It could be “relationships” centred, and this takes away the rather individualistic approach. Or it could be “family centred”, in that you can make decisions jointly and severally with whole families. But no terms are ideal – some people can have few relationships, and/or no family.
However you define ‘person centred care’, it is not only liable to being a bandwagon, but liable to be a performance reductionist metric imposed by non-professionals on professions to ‘improve quality’, when the whole world knows that many healthcare professionals desire time, space and resources do the job.
When I chat with a friend of mine living with dementia I do not see as ‘person centred care’, merely just being a good support hopefully. Likewise, if we have ‘dementia friendly communities’, I genuinely wonder who else we are being friendly or unfriendly to.
It’s become dreadfully easy for ‘person centred care’ to trip off the tongue.
But a few basic ‘messages’ somehow appear to have become drowned out – such as health and wellbeing not merely the absence of illness.
Kate Swaffer once joked about ‘purse centred care’ in a now seminal article “There is Big Money in dementia” (click here).
And after all you can set your criteria for your brand of purse centred care is like, trademark it, flog it; but this would defeat the whole ethos of the intentions of the work of Tom Kitwood.
Often ‘person centred care’ can be synonymous with profit generation in the private sector, hence a focus more on purses than persons as once quipped by Kate Swaffer, but it is a methodology whose roots warrant scrutiny. It gets away from the idea of patients as fodder for biochemical and neuroimaging investigations, with not much to be added by professionals. The meme that ‘there is no treatment for treatment’ plays very nicely into the medical model of dementia. However, taking a more social or psychological approach, you get a totally different perspective.
The complexity of dementia demands comprehensive individualised care that addresses physical, psychological, social, and legal issues of the persons with dementia as well as their caregivers Recently, person-centred care (PCC) has become valued in the field of dementia care. Nonetheless, PCC has been considered to be rather abstract or vague, partly as many publications are based on personal opinion, anecdotal evidence and/or theoretical constructs only.
Person-centred care is increasingly considered essential, whereas purpose-built facilities and environmental design are reported to enhance safety and to have a positive effect on behaviour. Within the UK National Health Service (NHS), the provision of person-centred services for individuals with acquired neurological conditions has been widely promoted. Services provided for people with dementia have been criticised in reports such as the UK Audit Commission’s ‘Forget-Me-Not’ which found them inflexible rather than person-centred, with poor integration of health and social services (Audit Commission, 2000).
To inform and direct service development for this clinical population, the National Service Framework for Long Term Neurological Conditions (Department of Health, 2005) originally set out quality requirements for improving PCC. PCC in rehabilitation has been defined as an approach that facilitates participation in decision making and goal-setting, client-centred education, client evaluation of outcomes, family involvement, emotional support, physical comfort, co-ordination and continuity.
Progressive deterioration in cognition, function, and behaviour make people with dementia increasingly dependent on others for normal activities of daily living. A person-centred approach is uniquely enmeshed with the pivotal importance of dignity. Dignity of identity represents a person’s subjective experiences of dignity and is related to integrity, autonomy, self-respect and social relations. This kind of dignity may be taken away or threatened by external events or by the acts of other people, for example, if an individual is humiliated or treated as an object.
Ideas about person-centred caregiving have been discussed by several authors within the gerontology literature. In the United Kingdom and elsewhere, Kitwood’s work with residents with dementia has been influential (Kitwood, 1997). This approach reconceptualises the dementias as involving processes not focused on pathology but on the social psychology of the person affected. An individual’s characteristics, including such things as the past, roles, personality, values, self-worth, spirituality, and so on, combined and defined through years of living, are often used to identify personhood at a higher level. Kitwood’s research places an emphasis on the belief that older adults should be treated as social beings worthy of relationship. Within each human being, regardless of cognitive impairments, is the desire to be respected and connected with others.
Dementia-care mapping (DCM) is a person-centred, multi-component intervention developed by the Dementia Research Group at Bradford University in the UK and is based on Kitwood’s social-psychological theory of personhood in dementia. DCM is a systematic approach for the assessment of PCC that can help to identify factors influencing behavior and to create individual person-centred care plans. DCM can also be used as an assessment for residents’ well-being.
As recent research investigations in nursing homes have emphasised, the personal relationships direct care workers forge with individual residents appear central to quality of care or quality of life outcomes on the part of residents. Evidence for improved outcomes for people with dementia through provision of person-centred care and dementia-care mapping thus far has been largely observational. However, taking a more robust scientific approach (it is mooted), person-centred care and dementia-care mapping both seem to reduce agitation in people with dementia in residential care.
Nursing staff’s person-centredness does play a modest role in relation to job characteristics and job-related well-being. Flexibility, possibly, is an essential ingredient of personcentered care. This person-centred care philosophy attempts to adapt care to the needs, preserved abilities, personality, habits, preferences, and cognitive, sensory, and physical limitations of the person with dementia. In order to do so, caregivers often have to adapt schedules, decision-making processes, and environments to the needs of the person with dementia, thus requiring a great degree of flexibility. It is currently felt that DCM is a “cost-neutral” intervention. It effectively reduces outpatient hospital appointments compared to usual care. Other considerations than costs, such as nursing homes’ preferences, may determine whether they adopt the DCM method.
The concept of person-centred care has recently been expanded to include “family-centred care” which acknowledges the important role of the family or other loved ones in the patient’s final days. Whereas experiences of having a relative with dementia in long-term care have been explored, the experience of spouses specifically is relatively sparse. As a contrast, staff on standard care wards often do not routinely complete personal profile documentation with family carers.
There has been – on the whole – a welcome recognition of the importance of a well-trained workforce to support people with dementia living in care homes. However, there is an emerging between the interventions that are routinely available and being commissioned, and the evidence base indicating benefit, arguably. In a way, person-centred care and family centred-care are not especially different what excellent caregivers, including professionals, should have been doing. Whilst nobody ‘owns’ the agenda, it would be a real shame if the marketing and corporatism o this ideology overplayed their hands at the expense of their clinical underpinnings. References
Audit Commission. Forget Me Not: Mental Health Services for Older People. London: Audit Commission, 2000.
Department of Health (2012b). Compassion in practice: Nursing, midwifery and care staff. Our vision and strategy. London: Department of Health.
Kitwood, T. (1997). The experience of dementia. Aging & Mental Health, 1, 13–22.
Sue Stephen, one of the founding members of the Dementia Alliance International (DAI), spoke about how she came to be diagnosed with PCA.
This is one of the latest additions on their blog, which I strongly recommend. The DAI is an unique group of individuals with a strong sense of solidarity, who live with one of the various types of dementia.
“I had been noticing myself for the last few years that I was having visual issues… very bad glaring.. when I tried to read..”
She put it down to stress, but she still went ‘to get [my] eyes tested.’
And this went on for a few years. Interestingly, she reports this delay in diagnosisas rather typical for many people finding a diagnosis of PCA.
Tests for dementia of the Alzheimer type, typically initially shown up by problems in short term learning and memory, were negative.
When she was eventually given a diagnosis, she was told, “That’s it. There’s nothing I can do. Here’s a prescription for Aricept. See you in six months.”
But she described being shocked, and she had no idea what PCA is/was.
“I lost all certainty in my life. How do I make decisions in my life?”
She then sat on her month doing ‘research’, but reported ‘three wonderful things’ which came out of her research.
She found a list of symptoms which matched what she had been experiencing. “That was really good”. This enabled her to see her GP who then went referred her onto more suitable specific tests, confirming the diagnosis.
That’s one of the slight paradoxes about the way we approach a fellow citizen of ours living with a dementia. Nobody wants to be defined by any medical conditions they live with. They do not wish (rightly) to consider themselves as a collection of diagnoses.
But it is often reported by people living with conditions how it can be both a blessing to know what might happen but also a burden to know something might happen, with this information resulting from a clinical diagnosis.
She then reported discovering the work of Sir Terry Pratchett, who is living well with PCA, still writing books.
A third thing which she reports is finding a group of people on Facebook of people with posterior cortical atrophy. It’s a closed group where people can share in private “scenarios”.
“I could see in the future what symptoms might be. I look at symptoms, and I think if this happened to me, what could I do now to help?”
Stephen reports sharing these stories really helped.
Terry Pratchett went to see other people living with posterior cortical atrophy in 2010, a form of dementia.
Pratchett is an example of an individual who has shown that it is possible to live well with dementia.
Pratchett admitted he was apprehensive about the meeting, as he said it was like ‘seeing into the future’.
One person in the meeting, “Anything coming through the postbox, I can’t read. Susan has to do everything from cutting my nails to putting my shoes on. This disease.. or whatever you call it, changes your perspective.”
“It didn’t happen – it evolved.”
Pratchett though admitted despite his fears he enjoyed the meeting.
“I can see why people enjoy meeting up”
He had dinner with Graham Doggett, who is an 70 year-old author, and academic who has written books about quantum chemistry, and his wife.
“Susan is the gardener. If I help her, I can never find the wretched branches in the air to prune. They disappear.”
“I was doing computing since 1959. That’s gone.”
“I used to play piano up to grade 7. Gone.”
“Reading, writing, gone gone”.
When the term ‘living well with dementia’, one of the main disclaimers on that is that the person living with one of the dementias will have their life before to compare their experience to.
And this is bound to impact upon one’s own personal perception of living with dementia. Unless you bother to find out about the past of a person, in relation to his environment, you will not be able to understand his or her world.
The symptoms of PCA can vary from one person to the next and can change as the condition progresses.
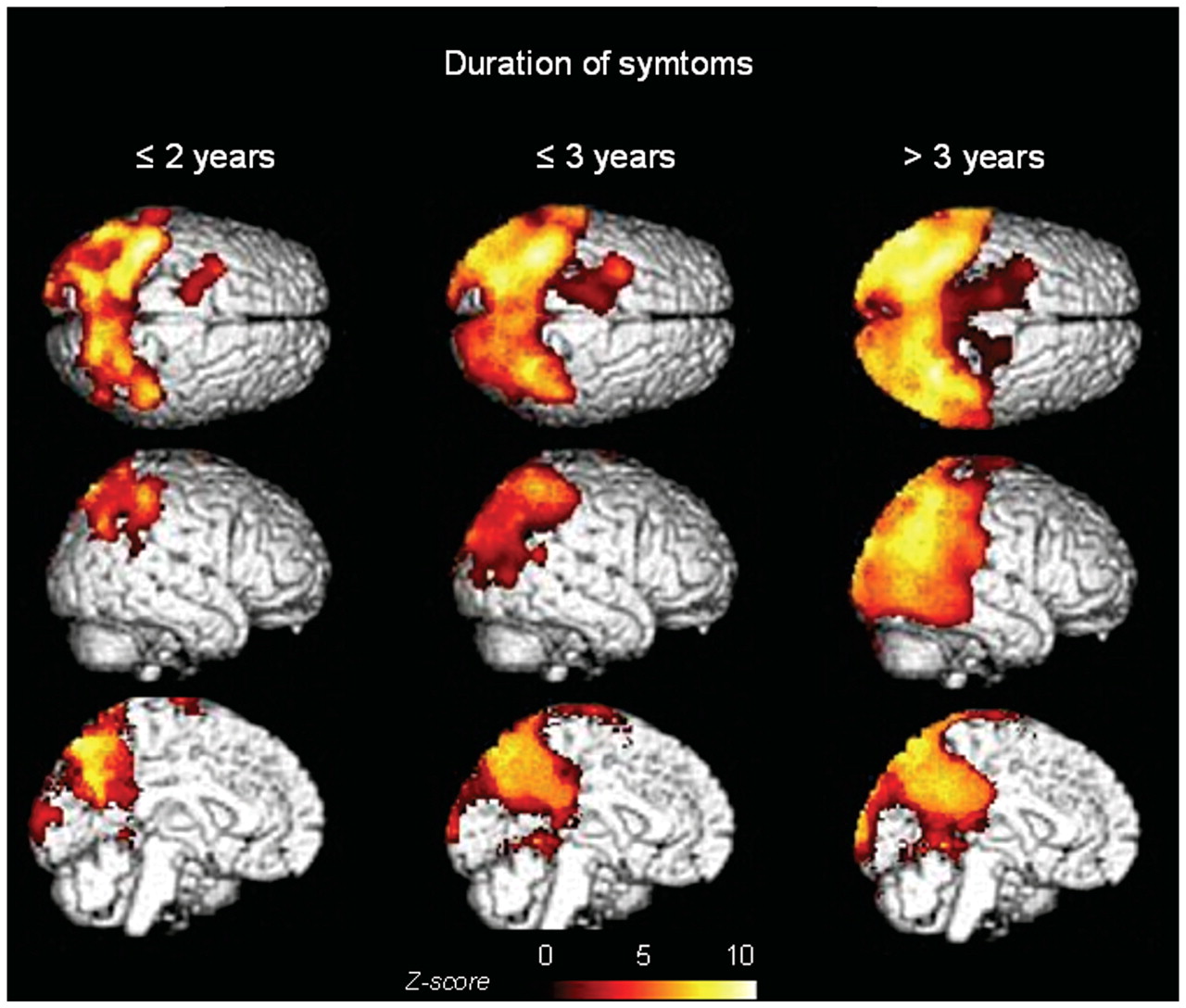
The most common symptoms are consistent with damage to the part of the brain at the back of the head, an area responsible for processing visual information.
Consistent with this process are slowly developing difficulties illustrating its slow and progressive nature due to a disease of the brain.
Now you’re even able to follow it using sophisticated ‘imaging’ of the brain.
These difficulties include visual tasks such as reading a line of text, judging distances, and distinguishing between moving objects and stationary objects.
Other symptoms include an inability to perceive more than one object at a time, disorientation, and difficulty maoneuvering, identifying, and using tools or common objects.
Some people can experience hallucinations.
Yet further symptoms can include difficulty performing mathematical calculations or spelling, and many people with PCA experience anxiety, possibly because they know something is wrong.
In the early stages of PCA, most people do not have markedly reduced memory, but memory can be affected in later stages.
This illustrates how this particular dementia is not just about memory.
Both Stephen and Pratchett demonstrate by a country mile while there are more to people than their dementias.
If you’d like to find more about dementia, you can do a short 45 minute session close to where you live in England (and now in other parts of the UK). The initiative is run by the Alzheimer’s Society, but is a Public Health England initiative. To find out more about this initiative called “Dementia Friends”, please go to their website.
There’s more to this initiative than the badge you’ll receive in the process, but this initiative is all about improving understanding in the general population about the dementias. I hope you will wish to learn more.
People with PCA are are at risk of being let down by ‘traditional dementia support groups’.
That is partly because they are younger and face different challenges, and partly because the activities offered in day centres puzzles, large-font books—are visual and thus actively unhelpful for people with PCA.
PCA is not new to the research community.
Already in 1902, the Czech psychiatrist Arnold Pick mentioned a woman’s inability to see and grab a lit candle held in front of her face in his essay “Ueber eine eigenthuemliche sehstoerung senile dementer,” Jahrbuecher f. Psychiatrie u. Neurol., see excerpt.
Several attempts at defining criteria for diagnosis exist.
The neurologist Frank Benson at the University of California, Los Angeles, coined the term while describing the pattern of symptoms in five patients (Benson et al., 1988).
Later, Mario Mendez, also of University of California and San Francisco proposed clinical diagnostic criteria arguing that PCA is its own syndrome, not simply Alzheimer’s disease with visual symptoms (Mendez et al., 2002).
The English dementia strategy is mindful of the needs to develop communities supportive of the needs of people living with PCA, of the need for high quality research research into PCA, and to think how people living with PCA can be best supported professionally and personally.
It’s not only people with posterior cortical atrophy who experience problems with vision, however. This is very important to be aware of.
Language is very important. Only this week, the media was stuffed full of talk of dementia being a ‘horrible disease’, and people ‘suffering’.
A recent Telegraph article cited, “Health Secretary Jeremy Hunt says it is “utterly shocking” that only half of people suffering from dementia are being formally diagnosed.”
Society has a certain image of dementia. It really is no use denying that this image is horribly negative, and feeding on this fear can be low-hanging fruit for raising funds through charity.
In this scheme of thinking, those with the dementia are only viewed through the prism of their illness, and this is often reduced to the image of its last and most tragic phases.
It is as if as soon as a diagnosis of a progressive dementia is made, the person in question, it is perceived by the rest of society, automatically becomes incapable of taking any autonomous decisions, loses his/her personality and identity and immediately needs to be cared for.
In reality, however, this illness can develop quite slowly: between the moment when it is diagnosed and the terminal phase, there may be years of development. Moreover, people living with the illness can rarely have the opportunity to express their thoughts and feelings about it: there is communication about them, but only rarely with them. The individual sadly disappears behind the blanket label of an illness.
The term “suffering”, however, sounds negative, and does not support the concept of “personhood”, and certainly does not fit with a philosophy of “hope” and “wellness”.
The way the NHS has latterly been structured as a market also reinforces this customer-supplier master-servile relationship. Dementia care is a ‘service’ you can pay for, with or without a personal health budget.
The dominant notion itself that the need of people with dementia to socialise should be met by “services” is disempowering, for the concept of service incorporates the notions of “providers” and “recipients”; of the “helpers” and “the helped”, of “us” and them”.
These notions further perpetuate the stigmatising assumption that people with dementia are only able to participate in relationships as “receivers”, and that relating to them is a problem for those who do not have the disease: they further advance the widespread perception that people with dementia are, essentially, a “burden” on their families and society.
This term “burden” can perhaps help validate the ‘burden’ some caregivers experience, but should not be assumed and should be avoided when speaking in generalities such as public presentations.
This language and terminology are in desperate need of change, and the prevailing perception of people past the first stages of dementia as just receivers of care, and users of services, needs drastic reframing.
The truth is that, as the symptoms of the disease progress, people with dementia can still play an active role in society, if provided with support, and this support can very often be provided by fellow citizens, rather than by professionals paid to deliver a service.
The purpose of person-centred language is to recognise the impact of language on thoughts and actions, to ensure language does not diminish the uniqueness and intrinsic value of each person.
Personhood is pivotal. This is the standing or status that is bestowed upon one human being by others in the context of relationship and social being. It implies recognition, respect and trust.
The aim is to create the positive conditions where the person can live without stigma; where people are treated with warmth and authenticity, listened to without judgment and are given opportunity for self-expression.
There are, however, ways to ‘reframe’ this debate.
Framing is a fast developing concept, as much in communication sciences as in other disciplines. This is partly due to the fact that it is a rather flexible approach that lends itself to many applications.
When there is a question relating to knowing how a particular subject is presented, in the media for instance, framing immediately springs to mind.
Instead of painting the illness as a homogenous and unchanging totality, it would be preferable to place the accent on its progressive and developmental nature.
One can put the accent on continuing to be a real person despite the decline due to the illness: acknowledge the personality, the identity and the life journey of those with a progressive dementia.
One can also develop empowerment and social inclusion with people with a progressive dementia. Such individuals are more than passive and dependent consumers of help and care services. They have resources that should be mobilized. The principle of inclusion implies that society is composed of all its citizens. However, this needs competent leadership.
Let those who living with dementia speak. It will provide others with one of the most powerful counter-examples in relation to the current dominant image, which often makes the individual disappear behind his/her illness.
Let your respect for those living with the dementia be obvious in what you have to say.
It is useful also never to forget that people with Alzheimer’s disease also have their own life story, their own personality and character. This is because their long-term memories are relatively preserved, due to a phenomenon first characterised by the French neurologist Ribot in the 1880s. Enable these aspects to be expressed too.
Those who disseminate messages, especially via texts designed to influence people, may deliberately choose a frame that the reader is supposed to pick up and appropriate so as to henceforth view reality in this way.
Given that frames form part of any culture, many of them are common to both the sender and the recipient of a given message.
The question of whether framing is a conscious process remains open to discussion: how far will the writer of a given text deliberately choose a frame that serves his own interests?
As we approach the G8 leading on the subject of what is important in dementia diagnosis, research and care, it is all the more important that we frame the discussion properly.
There are so many stakeholders in English dementia policy, it can be quite uncertain know where the current dementia policy has come from.
David Cameron has often argued that ‘it is not where you’ve come from, it’s where you’re going to’. If one of the goals is destigmatising dementia in society, how we articulate the present debate today is vital to our progress tomorrow.
This means not talking about ‘horrible’ and ‘suffering’ in a way as to encourage ‘moral panic’.
This means treating people with dementia, living at all stages with any particular condition, with the dignity they deserve; this will enormously help carers too.