It was a huge achievement for Prof Peter Mittler, human rights advisor to Dementia Alliance International, to get human rights firmly on the map last week. Dementia Alliance International is the main peak body for people with dementia, working closely, but autonomously, with the hugely influential Alzheimer’s Disease International.
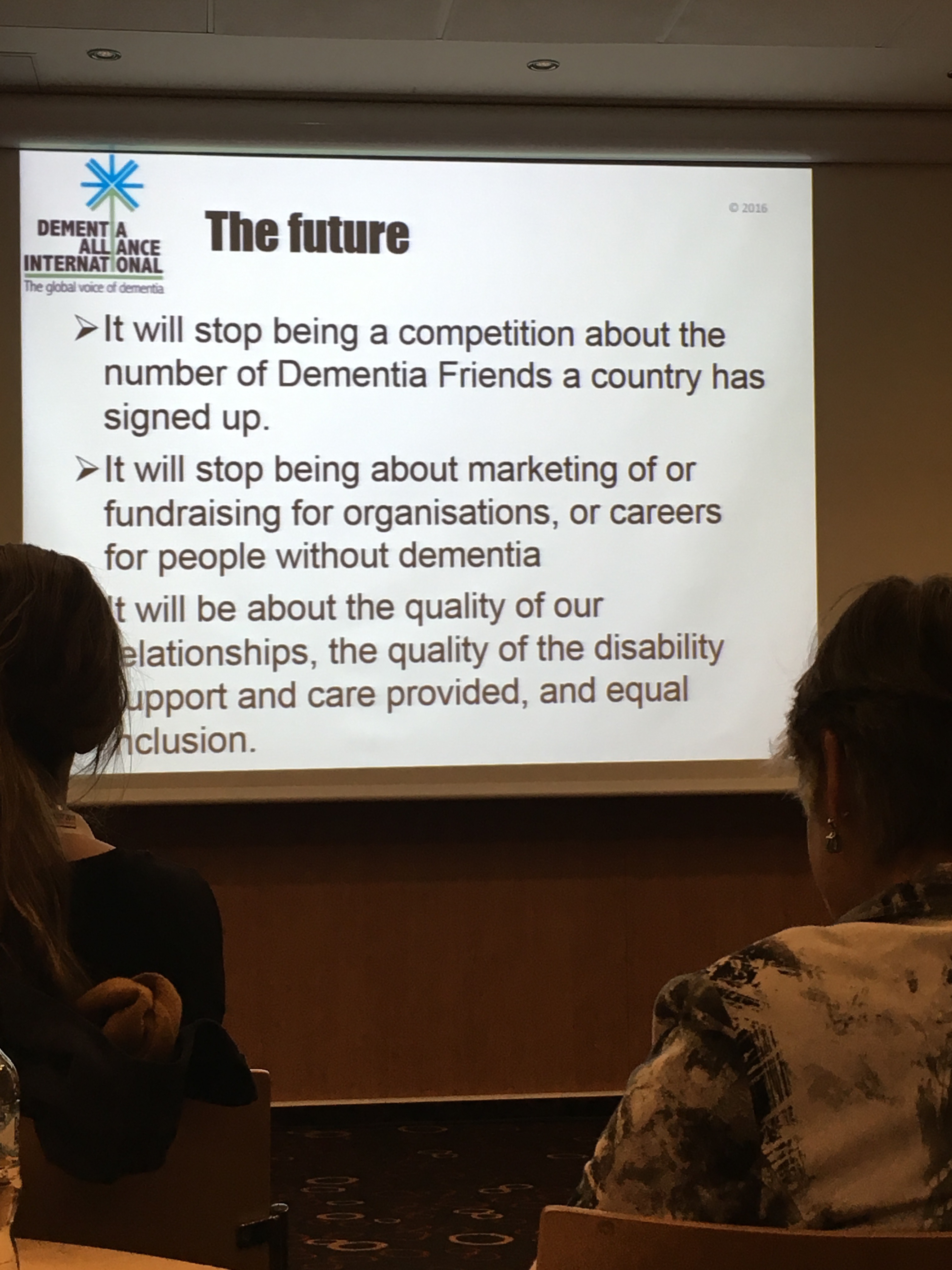
We have to talk about the Dementia Alliance International. This is a group entirely of people who are ‘living beyond dementia’, in the phraseology of their leader Kate Swaffer, campaigning for the needs of people living with dementia.
This can mean that they are often highly sought after for their independent, yet massively influential, views. Prof Mittler CBE has a long and distinguished career in the intellectual disabilities, and now currently lives with dementia. Mittler was indeed one of the leaders who helped to establish the UN Convention on Rights for People with Disabilities.
Mittler’s voice is therefore an authentic and learned one. He has much experience in navigating through the maze that is the policy territory of international NGOs. It was therefore pretty predictable therefore that the resolution he worked on for Dementia Alliance International, with Neil Crowther, would be unanimously assumed by the Alzheimer’s Disease International. This means that rights-based advocacy has now been delegated to all the national dementia societies to implement at a local level.
I believe the way forward in ‘activism’ for human rights needs above all to have authenticity. People with dementia need to be leading from the front, taking charge of the campaign. This is a cardinal example of authentic leadership from the front being much more convincing than ’empowerment or engagement’.
This means that an approach based on slick presentations and booklets with relevant case studies, for the benefit for commissioners, will not be effective in embedding a rights-based consciousness for rights, akin to the racial civil rights movement of Martin Luther King or the democratic movement of Mahatma Gandi.
This means that glossy pitches, grants and Powerpoints in town halls will not be the defining factor for embedding a rights-based culture.
Where I think the town halls will be useful will be in building up a ‘guiding coalition’ of people with similar values, such as other groups which are at the forefront of equality and campaigning against discrimination – e.g. groups campaigning for race-related rights, or rights of people with intellectual disabilities.
But again, such a manner of campaigning solely through this formulaic approach would be highly naïve, bordering on disingenuous, here. Human rights are universal and inalienable – this means they can’t be easily siloed off according to which ‘protected characteristic’, e.g. sexual orientation, age, has been breached on any one particular occasion.
Take for example a right to health, or a right to independent living, under the current framework of global policy on sustainable communities. People with dementia often are not only living with dementia: ergo, policy and campaigning should not treat them as if they are only living with dementia, even if this is a useful corporate third sector construct.
We need to get away from the idea, running through English policy like letters in a stick of rock, that dementia is a condition to be gamed for the purposes of writing grants, for example in human rights.
Above all, people with dementia, not anyone else, must be leading the campaign on rights based advocacy.
Martin Luther King wasn’t white.
Mahatma Gandhi wasn’t from Slovenia.
A rights based advocacy approach for dementia in England can be achieved to a limited extent even if fronted by big charity and associated enterprises belatedly jumping on the bandwagon. But I don’t deny they also serve an important function in ‘playing the system’ – but this is not really what campaigning for rights is about. And they also have the big £££££.
Authentic organisations like Dementia Alliance International, going local, are the key.
The conundrum is quite literally this: Only people with dementia can do it, but they can’t do it alone?
The World Health Innovation Summit (WHIS) now moves to the Royal College of Obstetricians and Gynaecologists on the 24th & 25th June 2016. This follows the success of the inaugural WHIS summit that took place in Carlisle, Cumbria in March of this year (23.7 million twitter impressions achieved).
WHIS is an unique and innovative forum in that it supports our health services by bringing communities together to innovate and share knowledge to improve health care for all.
The World Health Innovation Summit aims to bring all members of our communities together to support and help our health services by providing a platform for us to come together as a community to innovate and share knowledge so we all benefit.
As with the first Cumbrian summit, the London event has a range of expert patient innovators, clinical leaders, health commentators, academics and members of the business community speaking and working with members of the community to inspire innovation in healthcare.
I sadly was unable to make it up to Cumbria in the end, due to unforeseen circumstances, but my ‘here’s one I made earlier’ specially prepared talk on innovation and dementia was shown (and received good feedback).
I enjoyed the opening ceremony – though some delegates remarked to me how ‘fit’ the dancers were, maybe indicative of long plane flights to get to the conference venue.
Yesterday, I remarked to the CEO of Alzheimer’s Disease International (ADI), Marc Wortman, as Marc was leaving the hotel, that the Alzheimer’s Disease International conference had ‘interesting dynamics’.
What I actually mean is this.
Speakers from Dementia Alliance International were outstanding. I think Prof Peter Mittler’s talk on how people with dementia must demand access to their rights under the UN Convention for People with Disabilities was a game changer for many. For me, it was the best lecture I’ve ever attended in my lifetime.
I mentioned to some separately that for me Prof Peter Mittler was the equivalent of a premiership footballer, in terms of lecturing ability, when many lesser mortals in comparison look in lower divisions.
I reckon I would’ve actually made it to Dennis Frost’s talk on time especially, not wandered through accidentally half-way through by accident, had Dennis not been advertised as ‘A person with dementia’. This billing on the programme was complete nonsense – as ridiculous as having ‘A person without dementia’ to describe the billing of someone like a policy wonk from WHO.
This was a worthy project which caught my eye.
It was lovely to be recognised by so many at the conference – people whom I had never met before, as well as longstanding close friends of mine. The conference expectedly did have the atmosphere of a family wedding – with people I like and respect there.
I think Jeremy Hughes and George McNamara, senior people at the Alzheimer’s Society, gave excellent presentations. George’s one is particularly relevant to my next book, and contained many many useful avenues for future directions. I think Dementia Friends on principle has good aims, but a real concerted effort must be put now into making meaningful sense of this high cost campaign.
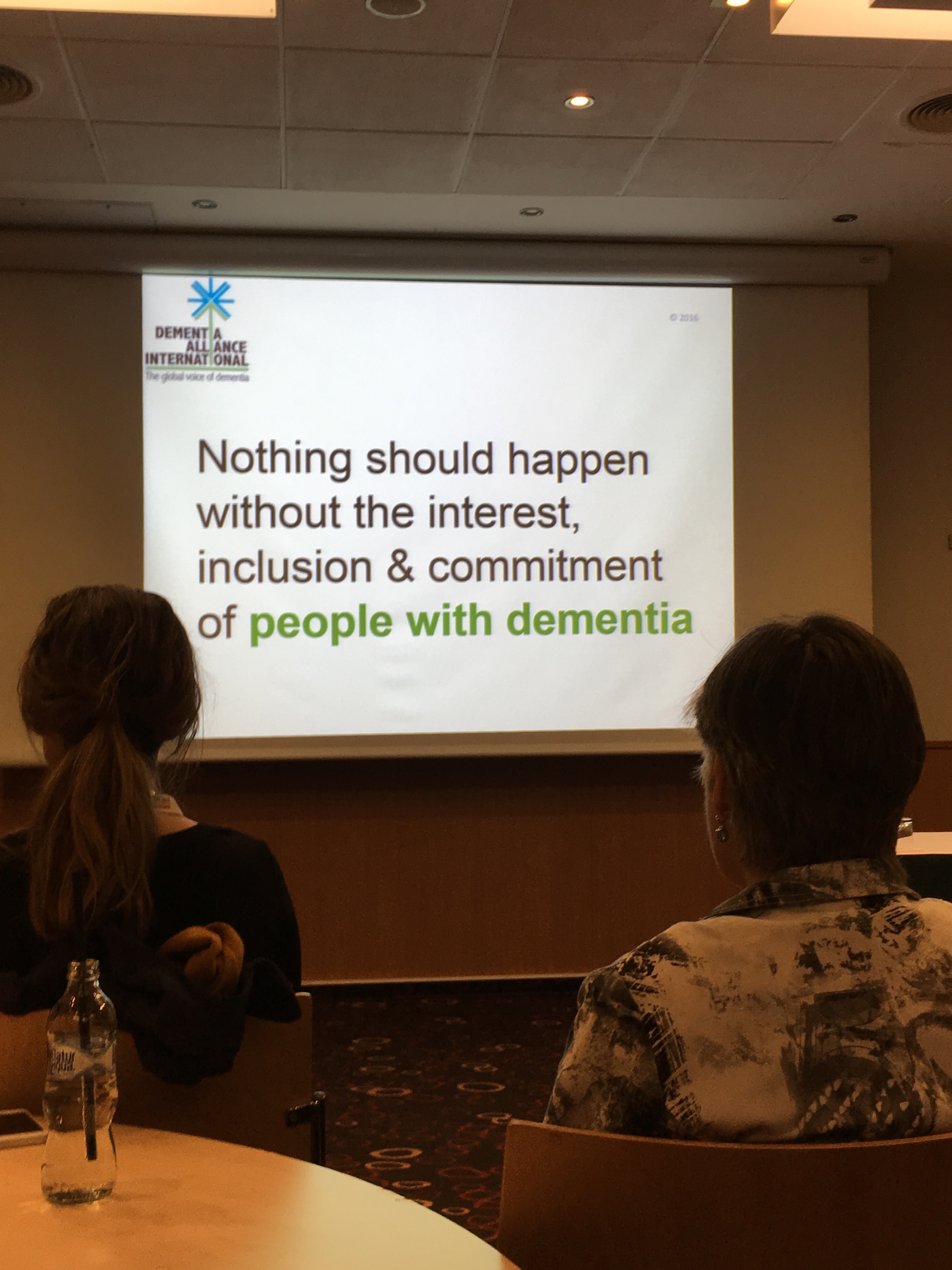
Dementia Alliance International (DAI) is a group essentially run by people with dementia to advocate for people with dementia. But the sheer individual brilliance of the presenters shone through – including Prof Peter Mittler and Prof Mary Radofsky whose contributions were incredibly interesting. There’s no doubt ADI hugely benefited from their presence in the conference, including in the programme list. But I do also feel this is a beginning.
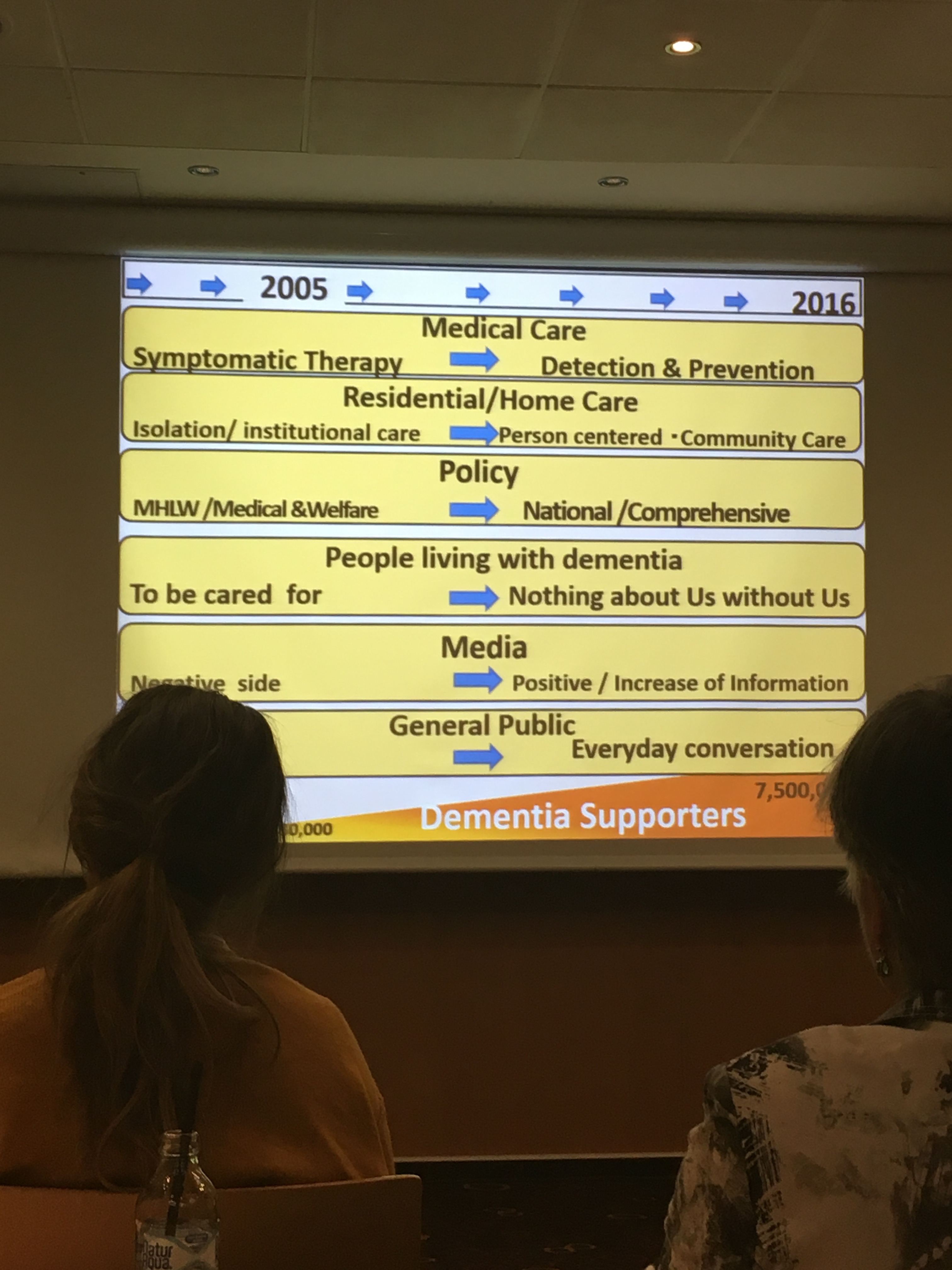
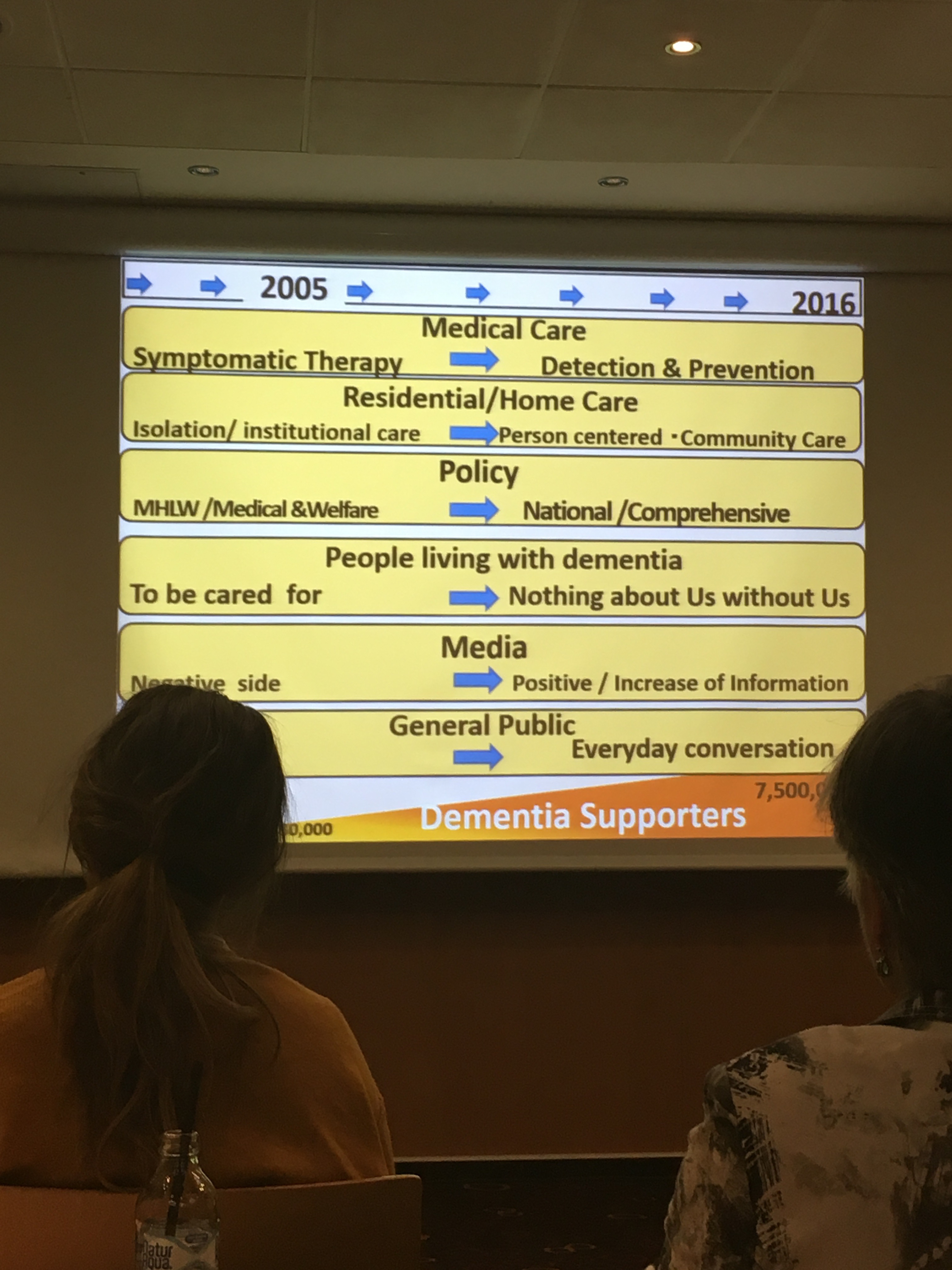
The mood music has changed. DAI has a scarce resource other people want – individual expertise by people with dementia – which many people do not have. It’s clear that the future direction of dementia policy now can be ‘no decision about us without all of us’, and can move from dinosaur lobbying techniques and hospital-dominance to representing the sincere views of people living with dementia.
A day before the first full day, Glenn Rees AM, Chair of ADI, let us know that his Board had approved DAI’s proposal to promote Convention rights, and this would now become their official policy, such that it would be left up to individual national organisations as to how best implement rights-based advocacy. Rights-based approaches, including rights to independent living and right to health, have huge implications for dementia care and support worldwide.
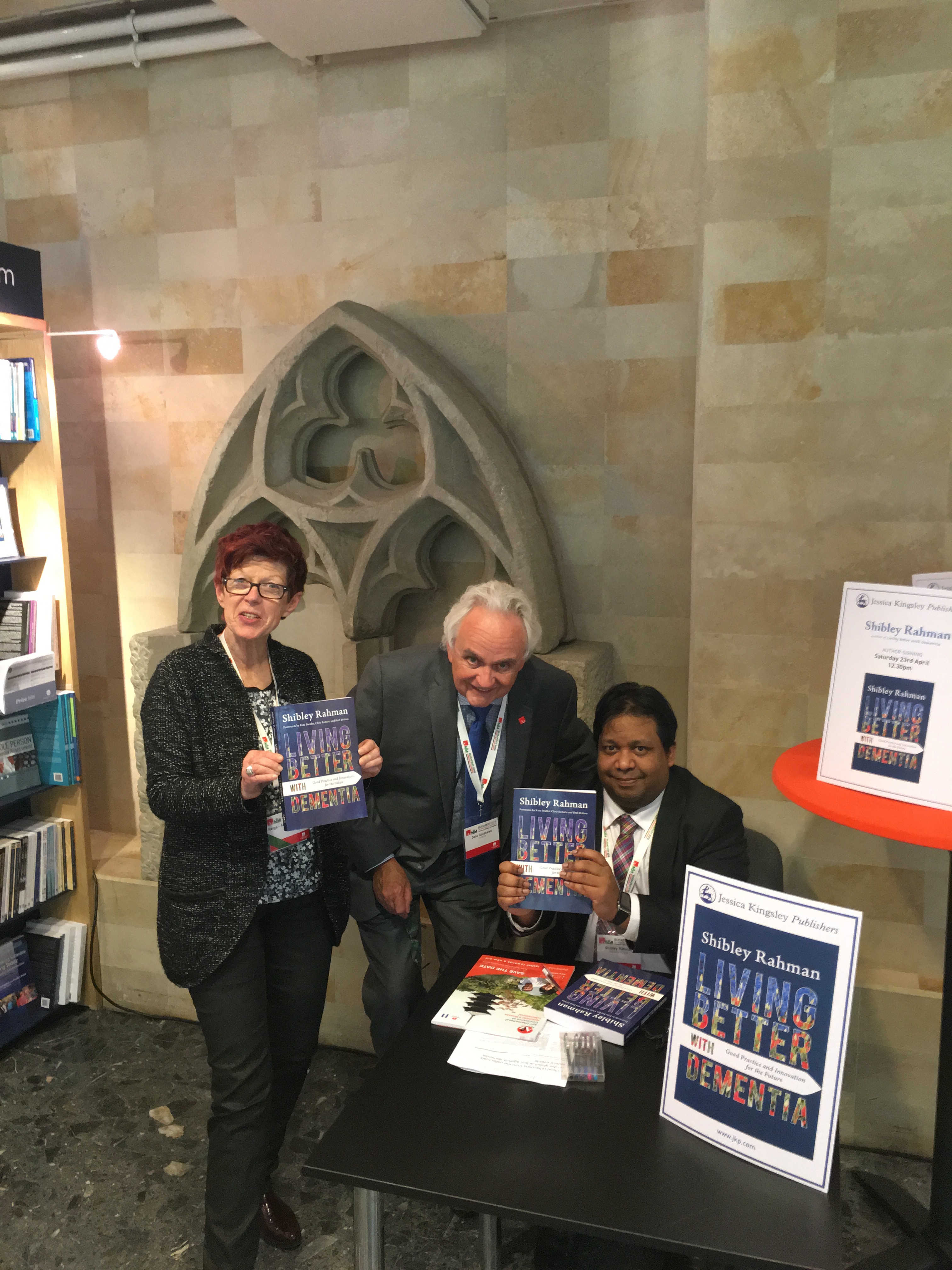
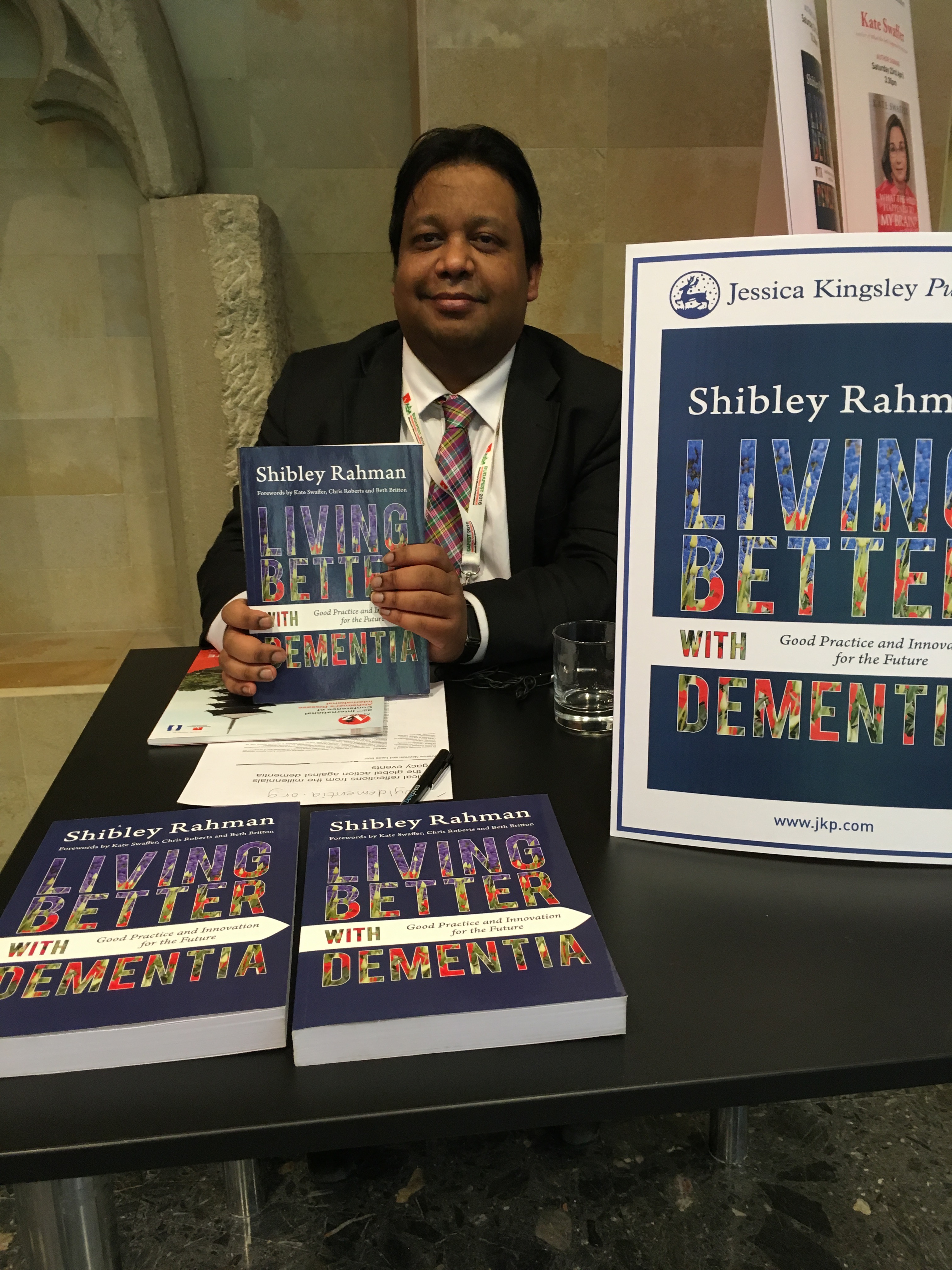
Helga bust a gut to help me with my book signing session.
Thanks very much to Peter Macfarlane from Wisepress for his help for this. Dale Goldhawk, Vice Chair of ADI, even bought a copy!
I had great feedback from my presentation on the awareness of international human rights. Thanks very much to John O’Keefe for chairing this.
Some photos I took are here.
I suppose my favourite ‘times’ of conference was when Agnes Houston made a ‘selfie’ photo of herself for the first time.
And also I think Agnes and Nancy McAdam talking about how they felt really included in Scottish dementia research (#whywedoresearch) on a boat on the Danube was much fun too. A sort of “Alas Houston and McAdam” moment.
Whether or not interventions and initiatives are worthwhile demands long term scrutiny. This is to make sure that initiatives such as ‘Dementia Friends‘, the provision of mass information sessions for the public on some basics about dementia, or accreditation schemes for dementia friendly communities aren’t done, ‘signed off’, and silently disposed of when it’s unclear what the outcomes have been.
It’s always been said that “Dementia Friends”, not ‘training’ but provision of information about dementia, unsuitable for anything higher than tier 1 (in comparison specialist healthcare staff might be trained to tier 3), is a ‘social movement’ “turning communication to action”. In other words, armed with your new knowledge of dementia, you might do something constructive in response.
I have never convinced of a reason for this programme, say, is in improved detection by you of someone slow with their change ahead of you in a shopping queue because of dementia. In fact, getting frustrated at an old person in front of you due to slowness in counting change might be a phenotype of outright ageism, irrespective of the presence of dementia, or simply bad manners. There has been an issue of how the programme might encourage you to behave a certain way towards ‘a person with dementia’. But that is to assume you can identify a person with dementia as if they were wearing a sticker on their forehead with the word “DEMENTIA” in big letters. Many disabilities, including dementia, are indeed invisible. This is akin to not judging a person as ‘normal’ who happens to have an indwelling catheter due to continence issues in multiple sclerosis.
The late Conservative health minister, J. Enoch Powell, famous for various other things too, always warned against the ‘numbers game’. In a break-out session for the Alzheimers Disease International conference yesterday, four speakers from four jurisdictions, including England, Japan, India and Australia, described their perception of what a ‘dementia friendly community’ might be. Kate Swaffer, Chair of Dementia Alliance International, emphasised how such a community should be seen as enabling and inclusive, citing Kiama as an example of good practice.
But other jurisdictions clearly lapsed into “the numbers game” – Japan cited a growing number of ‘dementia caravan volunteers’. the state of Kerala in India offered 100,000 “dementia volunteers”, and Jeremy Hughes, CEO of the Alzheimer’s Society, cited how the Dementia Friends “With a little help from your friends”, slickly produced by professionals, had garnered over a half of million ‘hits’ on YouTube.
Particularly having met Gina at the Alzheimer’s Society conference in London last year, I can say I love the Dementia Friends video as a creative pitch.
But there is a moral imperative to see what these dementia programmes are doing, not least because the substantial cost of a public backed initiative might be at an opportunity cost to other equally meritorious approaches, such as improving rehabilitation services for dementia. Also, there is a fundamental wish, surely, to know whether the initiative has met any of its original ambitions.
The original English dementia strategy, “Living well with dementia”, was supposed to last five years, and indeed did so from 2009. There was never a renewal of this strategy. There was instead an overwhelmingly underwhelming‘implementation plan’ for ‘Dementia 2020′ from the Department of Health, which did not address the Baroness Greengross’ stated wish to log the ‘lessons learnt’ from the successes and failures of the original strategy.
In this strategy, it was clearly stated that English dementia policy had to prioritise mitigation against stigma and prejudice towards dementia. Of course, there can be ‘unintended consequences’ of so-called ‘dementia awareness’ – a substantial number believe that queuing in a shopping queue called ‘dementia friendly checkout’ or parking in a ‘dementia friendly car parking space’ in fact markedly exacerbates stigma, and is potentially quite offensive.
Even a badge, rather than encouraging inclusion, can impose an unintended ‘them and us’ distinction.
So the idea of “Dementia Friends”, or any other jurisdictional attempts to emulate this, being a ‘social movement’ is deserving of scrutiny, and should not glibly assumed.
Consider this. Say there are 2 million people who go out each to buy a Mars Bar, a homogeneous product, following an intense publicly funding marketing campaign set up by top quality marketing agencies. Could be said that 2 million purchases of Mars Bars was a social movement of Mars Bar friends – or simply an anticipated benefit of a mass marketing ‘top down’ broad sweep campaign?
The talks from the other jurisdictions indeed touched upon what might have been reasonable outcomes.
Say, for example, in Japan.
And indeed there are a number of possible ways in which you could consider ‘Dementia Friends’ has been of benefit.
These might conceivably include:
reduction of stigma and prejudice in public perceptions
better knowledge of dementia and how dementia impacts on personal lives
uptake of ‘dementia friendly initiatives’ in quality of care, such as ‘dementia friendly hospital wards’
better ‘customer experience’ from high street businesses or corporates
better perceived ‘quality of life’ of people living with dementia and those closest to them
better awareness of possible symptoms of dementia thus promoting more timely diagnosis of dementia
increased confidence of people with dementia living independently (not in isolation) in the community.
It is not fair and appropriate to reduce this into two or three questions, say “how much more confident do you feel about dementia?”. People invariably don’t know the sample size, or any other thing about basic demographics of the sample.
I have noticed a huge drive in Dementia Friends, and in fairness other jurisdictions too, to play ‘the numbers game’. So, at first, you are seeking one million friends – and then you can make the website deliver more friends more easily – so the number increases for little further effort. But this is being accompanied by a marked shift in societal attitudes in dementia? It’s like my mass marketing of Mars Bars analogies.
A social movement for me also implies that the people delivering the information session have some intellectual investment in the process. This is not true of Dementia Friends, which specifically wants Dementia Friends Champions to deliver the same product as advertised – as indeed a Big Mac is the same whether you buy it in Doncaster or Dubai. The organisers of Dementia Friends clearly do not want Mars Bars accidentally turning into Snickers, by the addition of a few peanuts, by a few ‘rogue champions’.
One or two companies delivering a ‘better customer experience’ will be an expected outcome from those companies which have invested money in such a programme. The issue is whether this is replicable through means such as ‘secret shoppers’.
So, all in all, it is of vital importance how you actually measure the efficacy of the social movement. I indeed asked this as a general discussion point in the session chaired by Glenn Rees, the Chair of Alzheimer’s Disease International.
And of course there are a number of ways to tackle this question.
Jeremy Hughes mooted the idea of high quality survey data. I think this would be far superior to relying on a quantitative analysis of pledges from the pledge card. For a start, there is a problem with potentially low response rates for pledge cards. Secondly, whilst easy to codify, the information from the pledge cards are only as good as the quality of the pledges you can pick from in a multiple-choice fashion. For example, in my experience as a Dementia Friends Champion, I have learnt that many people want to ‘join dementia research’, as it gives them some agency and hope about dementia. And yet this is not a stated pledge. It does concern me how slow Dementia Friends has seen to be in working with NIHR in fostering links between the ‘Dementia Friends’ and ‘Join Dementia Research‘ initiatives?
Formal assessments do of course exist of the ‘success’ of social movements. But for the reasons I describe above actually identifying the outcome measures is itself tricky.
Take for example the ‘social value return on investment’ (SROI).
The key assumption of SROI analysis is that there is more to value creation than purely economic value, indeed the value creation process can be thought of as a continuum with purely economic value at one end, through to socio-economic somewhere in the middle, and social value at the other end. Economic value creation is the raison d’etre of most for-profit corporations (i.e. taking a product to service to market that has greater value than the original inputs and processes that were required to generate it), whereas social value is created when ‘resources, inputs, processes or policies are combined to generate improvements in the lives of individuals or society as a whole’.
Social value creation is a huge goal for the third sector in facilitating social inclusion and access for those that may be marginalised). However, unlike economic value, social value is difficult to quantify, varies according to the type of organisation involved in its creation and does not have a common unit of analysis (such as money) that enables it to be easily standardised and compared.
Social Movement Impact Theory (otherwise known as Outcome Theory) is a subcategory of social movement theory, and focuses on assessing the impacts that social movements have on society, as well as what factors might have led to those effects. It is relatively new, and was only introduced in 1975 with William Gamson’s book “The Strategy of Social Protest,” followed by Piven and Cloward’s book “Poor People’s Movements”.
Finding appropriate methods to use for studying the impacts of social movements is problematic in many ways, and is generally a large deterrent to scholars to study in the field. The first problem scholars ran into was defining “success” for social movements; the significance of this is that key stakeholders often have disagreements of what a movement’s goals are, and thus come to different conclusions about whether a movement has “succeeded.” Argos might have different outcomes in mind to Addenbrookes Hospital in Cambridge?
Other issues arise when one attempts to locate a movement’s impact in all arenas. Impacts are most often studied at the political level,and yet it has been proven that they have individual, cultural, institutional, and international effects as well. Is exporting an operational homogenous product the same as propagating a wider social movement?
The psychology of the individuals who participate in movements are normally profoundly affected. But do the 1.5 million ‘Dementia Friends’ feel any sense of connectedness to one another? One suspects not, especially if some have achieved ‘Dementia Friends’ status through a few minutes on a computer terminal in isolation.
Has Dementia Friends shifted quality of care or attitudes in care homes, for example? Has it shifted political attitudes to dementia which have historically been shaped by much political lobbying? One parsimoniously thinks not if the current Government wishes to shift emphasis now to diabetes, and has not even renewed post 2014 the English dementia strategy.
Inevitably within government there continues to be an interest in and application of techniques for program or project evaluation such as cost benefit analysis. And this from an utilitarian perspective makes complete sense – in terms of society’s assessment of ‘getting most bang for your buck’.
Lessons for Dementia Friends can also be usefully learnt from other arenas.
For example, an interesting example of an impact evaluation is provided in a report from a few years ago. This report was entitled “An evaluative framework for social, environmental and economic outcomes from community-based energy efficiency and renewable energy projects for Ashton Hayes, Cheshire March 2012″ , and was published from the nef (the new economics foundation).
Ashton Hayes is a rural village located just outside Chester. Their aim is to become the first carbon neutral village in England, through energy efficiency measures and carbon offsetting; by: ‘…encouraging everyone in their community to think about how their way of life affects their impact on climate change and to help people to understand how simple actions can make a big impact on carbon dioxide emissions to the atmosphere.”
The report helpfully discusses choice of indicators.
It was proposed that all stakeholders are often the best people to identify indicators, but a common mistake is to misinterpret what is meant by ‘measurable’. One should avoid the trap of using inappropriate indicators just because they are readily available; so, if the outcome is important, you will need to find a way to measure it.
Outcomes work also concedes that effect of some outcomes will last longer than others. Some outcomes depend on the activity continuing and some do not. For example, in helping someone to start a business, it is reasonable to expect the business to last for some time after your intervention. The difference between ‘benefits’ and ‘outcomes’ is therefore imperative in this context. The outcomes of a campaign such as ‘Dementia Friends’ will be valid as a snapshot in one particular time.
I feel things will change say when people with dementia are genuinely considered as ‘equal and reciprocal partners’ in any relationship. For example, it should be an automatic given that dementia friendly communities include people living with dementia as paid consultants, not tokenistically ‘involved’.
Kate Swaffer successfully conveyed the sentiments behind this for Australia yesterday, for example.
And I think that is the way things are heading now with the Alzheimer’s Disease International umbrella approach of inclusion and a strong ‘rights based approach’, which hopefully will now filter down to national agencies for implementation.
I feel that how ‘successful’ Dementia Friends has been, given the statement below when the initiative was first announced in November 2012, needs to be comprehensively examined.
And ultimately Dementia Friends has to be much more than a successful, easily exportable, marketing campaign – it needs to deliver results on the ground. This is no different for the Alzheimer’s Society and the Government as it is for small social enterprises. The rules of the game must be equally applicable to all, otherwise it’s an “unfair market”.
Dementia enabling communities primarily needs to be for the benefit of people living with dementia and their closest.
I am very honoured to become a Fellow with the England Centre for Practice Development this week. The work of this centre is very much up synchronous with mine.
My profile:
Dr Shibley Rahman
Dr Shibley Rahman became a Queen’s Scholar in 1987, and he graduated from the University of Cambridge in medicine in 2001, where he also received a Foundation Scholarship. A major finding from his Ph.D. research conducted there under Prof John Hodges was the identification of a novel, innovative, cognitive neurological technique for diagnosing at an early stage the behavioural variant of frontotemporal dementia. This influential finding has been replicated extensively in the subsequent decade, such that it is even cited in the current Oxford Textbook of Medicine. Subsequent post-doctoral research was successfully published by him from the Institute of Neurology at Queen Square, in the behavioural and cognitive neurology of idiopathic Parkinson’s disease in the laboratory of Prof Marjan Jahanshahi; he had also done his junior neurology training under Prof Martin Rossor at the National Hospital for Neurology and Neurosurgery, Queen Square. He is a current member of the Royal College of Physicians in London, having completed his Membership in 2005. Notwithstanding a coma due to meningitis in 2007, Rahman subsequently went onto complete, newly physically disabled, his Bachelor and Master of Law, obtaining a commendation in international corporate law. He subsequently completed his MBA at BPP Business School, where he excelled in economics and markets as well as innovation management.
Originally, Dr Rahman was a supervisor at Cambridge in finals for experimental psychology and neuroscience, but latterly he has grown to be a popular (and invited) speaker at numerous public events both nationally and internationally, including at the invitation of the King’s Fund, Alzheimer’s Europe and Alzheimer’s Disease International. He has become influential in English dementia policy, being a keen proponent of rights-based advocacy for dementia, given his substantial medical and legal training. Dr Rahman’s contributions have been particularly well respected by people living with dementia, as well as by global groups in the third sector and by academics and practitioners alike.
A major drive behind Dr Rahman’s work is doing participatory research collaboratively and inclusively. He is passionate about ensuring the public are both aware and knowledgeable what current trends in dementia research are, and how they impact on policy developments. For example, his first book entitled ‘Living well with dementia: the importance of the person and the environment” was generally accepted to be a thought-provoking, original contribution to the field which won best book award for health and social care for the BMJ Awards in 2015. He has also been instrumental in helping to establish an innovative MSc programme in dementia care and leadetship at BPP Health School, aimed at busy professionals who wish to advance their practitioner skills in dementia.
Selected papers
Rahman, S, Dening, K. (2016, in press) Clinical specialist nurses are still desperately needed in English dementia policy, Nursing Times.
Rahman, S., Griffin, H.J., Quinn, N.P., Jahanshahi, M. (2011), “On the nature of fear of falling in Parkinson’s disease”, Behav Neurol, 2011;24(3):219-28.
Rahman, S., Sahakian, B.J., Nestor, P.J., Hodges, J.R., Robbins, T.W. (2005) “Methylphenidate (‘Ritalin’) can Ameliorate Abnormal Risk-Taking Behavior in the Frontal Variant of Frontotemporal Dementia”, Nature (Neuropsychopharmacology), 31(3): 651-8.
Rahman, S., Sahakian, B.J., Hodges, J.R., Rogers, R.D., Robbins, T.W. (1999) Specific cognitive deficits in early frontal variant frontotemporal dementia, Brain, 122 (Pt 8):1469-93
Selected books
Rahman, S. (2016) [foreword by Prof Sube Banerjee, Lisa Rodrigues and Lucy Frost] Enhancing health and wellbeing in dementia: implementing person-centred integrated care, London: Jessica Kingsley Publishers (in preparation).
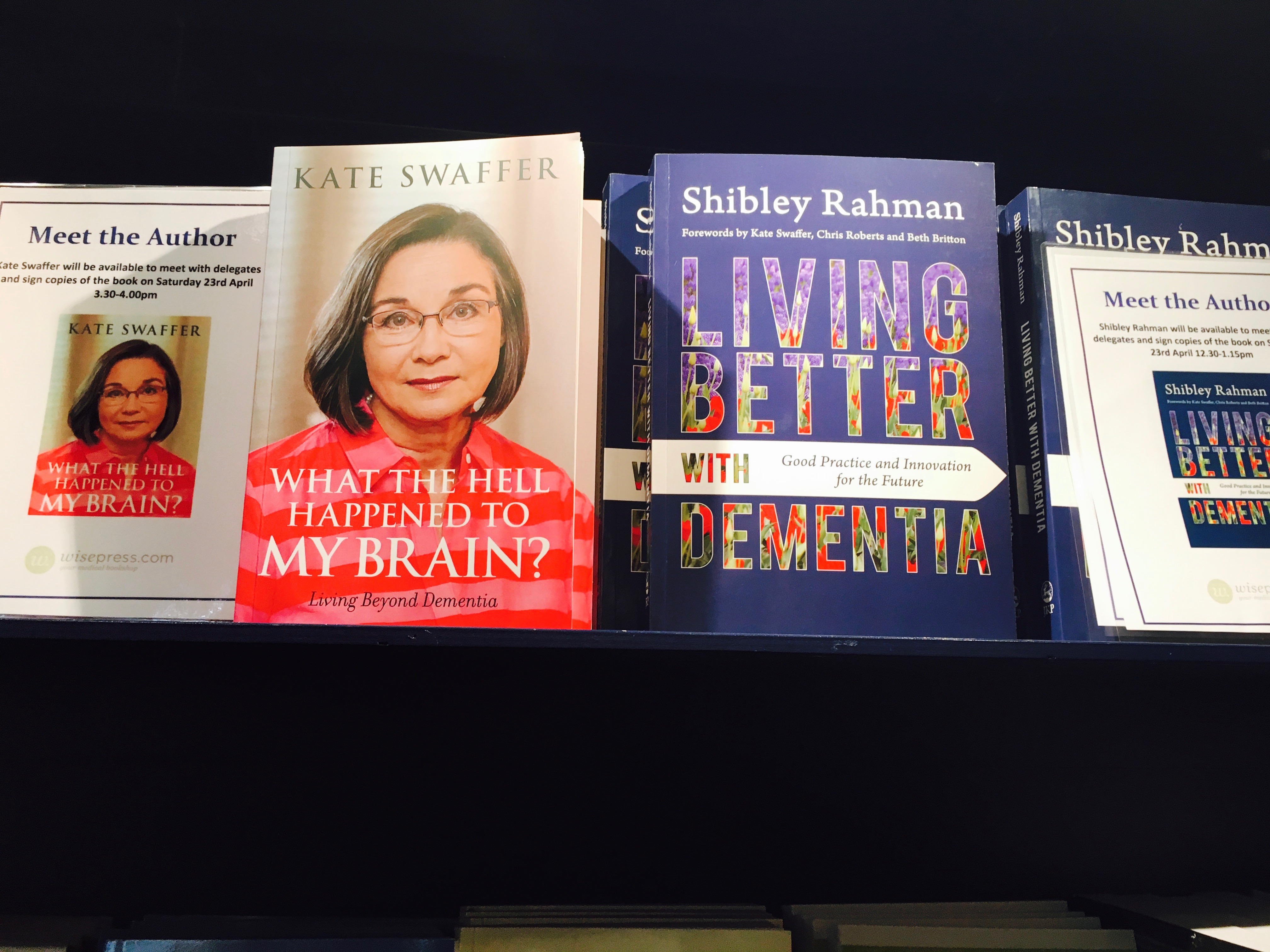
Rahman, S. (2015) [foreword by Kate Swaffer, Chris Roberts and Beth Britton] Living better with dementia: good practice and innovation for the future, London: Jessica Kingsley Publishers.
Rahman, S. (2014) [foreword by Prof John Hodges, Prof Facundo Manes, Sally Marciano] Living well with dementia, Oxford: Radcliffe Health.
**Winner of the Best Book for health and social care in BMA Book Awards 2015 **
Some blatant unintentional mistruths and misdirections.
I didn’t like the primacy of the diagnosis and the ‘doctor knows best’.
In a way what you call dementia is irrelevant in that your focus should be on enablement for problems people have – irrespective of name. On the other hand, knowing the type of dementia is worth knowing from the perspective of anticipating symptoms (e.g. in vision or language) – and in the specific case of lewy body dementia drugs to avoid.
Also memory problems are NOT ESSENTIAL to make a diagnosis of dementia. I assume he’s getting confused with the NINCDS-ADRDA criteria for Alzheimer’s disease. In a sense, he represents what academic physicians in dementia dislike – conflation of all dementia as Alzheimer’s disease. For example, posterior cortical atrophy can be purely vision, behavioural variant frontotemporal dementia can be purely behaviour and personality, logopenic PPA can be purely language, semantic dementia can be purely language.
The idea of diagnosing pre-dementia 30 years before onset of symptoms is hard sell by research sponsored by Big Pharma. A ‘positive’ Pittsburgh compound result he talks about is not a guarantee you’re developing dementia – and I suspect his is extracted from cerebrospinal fluid involving a painful spinal tap with a big needle in your back.
Talking of which – why NOTHING on living beyond a diagnosis of dementia? The tunnel vision of some in the medical profession is truly astounding. There could be have been a discussion of enablement for example or rights of people with dementia.
And none of the wonder drugs have got approval here or anywhere else, further to the usual suspects e.g. cholinesterase inhibitors and memantine, which have limited efficacy.
As for the idea of seeing patients on their own, for cognitive testing, possibly, but for neurological history a definite no no – an informant history is essential and even more so for the behavioural variant of frontotemporal dementia where there may be no insight initially.
I love the campaign as it goes some way into providing basic information about dementia for the general public.
I strongly approve of this, given the stigma and prejudice surrounding dementia from some in the English population
I do not wish in any way to undermine the brilliant ‘Dementia Friends’ campaign from the Alzheimer’s Society and Public Health England, described here.
But please do allow me to say a few words.
I know of the history of the bookcase analogy as used in the ‘Dementia Friends’ campaign.
A description of the crux of this analogy is given by Gemma Jones (2005).
A description of this analogy is given here. The actual drafting of the analogy for Dementia Friends is slightly different albeit precise. I do not a have to reproduce it here.
Problem 1: This bookcase does not hold memory for skills. Please note that the script of the bookcase analogy does not refer to skills.
That drafting of the Dementia Friends analogy is CORRECT.
Park for a moment in the link above – the description says ‘memory or skill’.
This part is very untrue.
Skill learning is thought to take part in the brainstem of the brain – and most affected in parts of the brain called the sub cortex not cortex. Therefore skills learning is most likely to be affected in the dementia from Huntington’s disease (compare in contrast Alzheimer’s disease).
Skills learning is what we refer to when, say, riding a bike – it’s not memory for facts or events. It’s thought to be quite old in evolutionary terms.
Problems with the actual Dementia Friends analogy
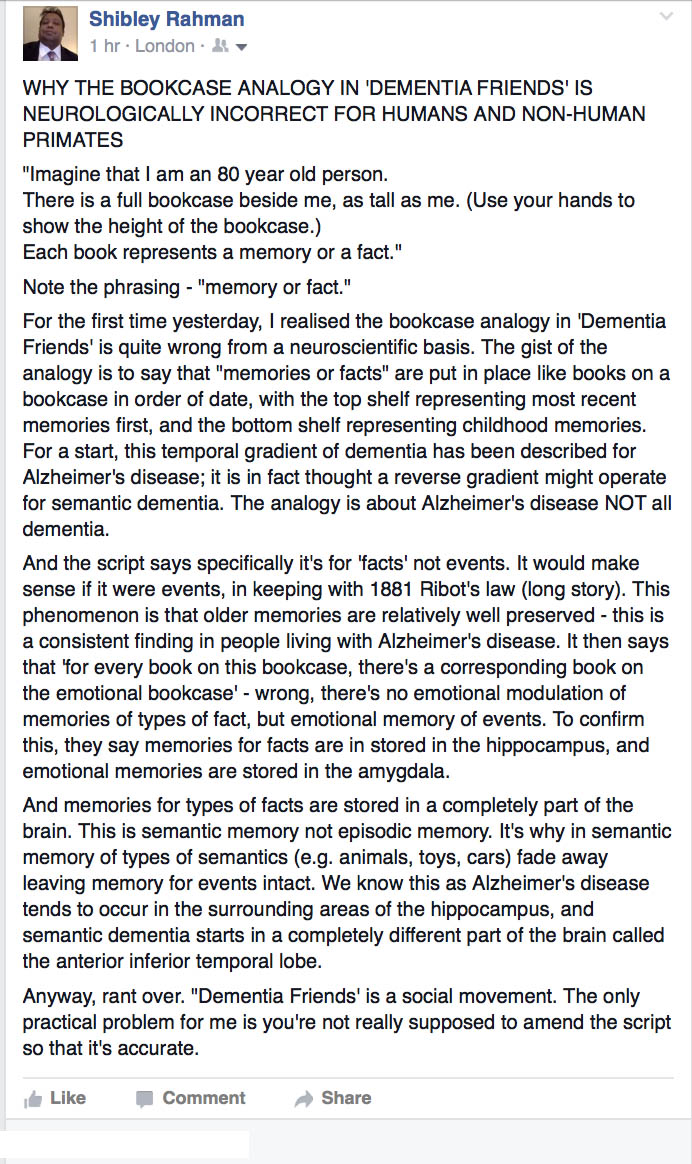
My ‘beef’ with the analogy as given in the current Dementia Friends below I summarised in a Facebook post.
The post is here:
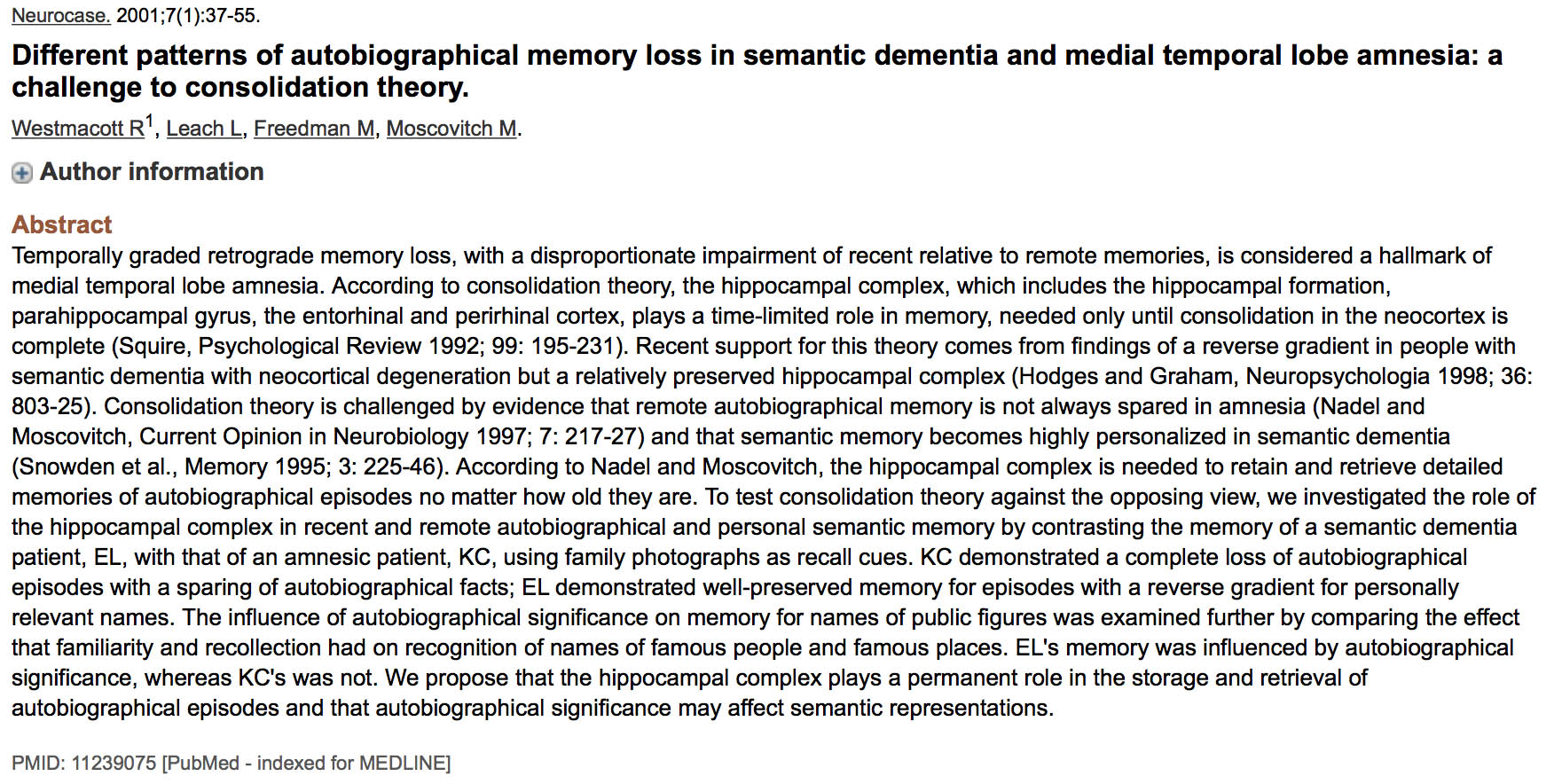
To start off, you have to understand the difference between the organisation of episodic and semantic memory in the brain.
Problem 2 – The issue with the description “memory or facts”
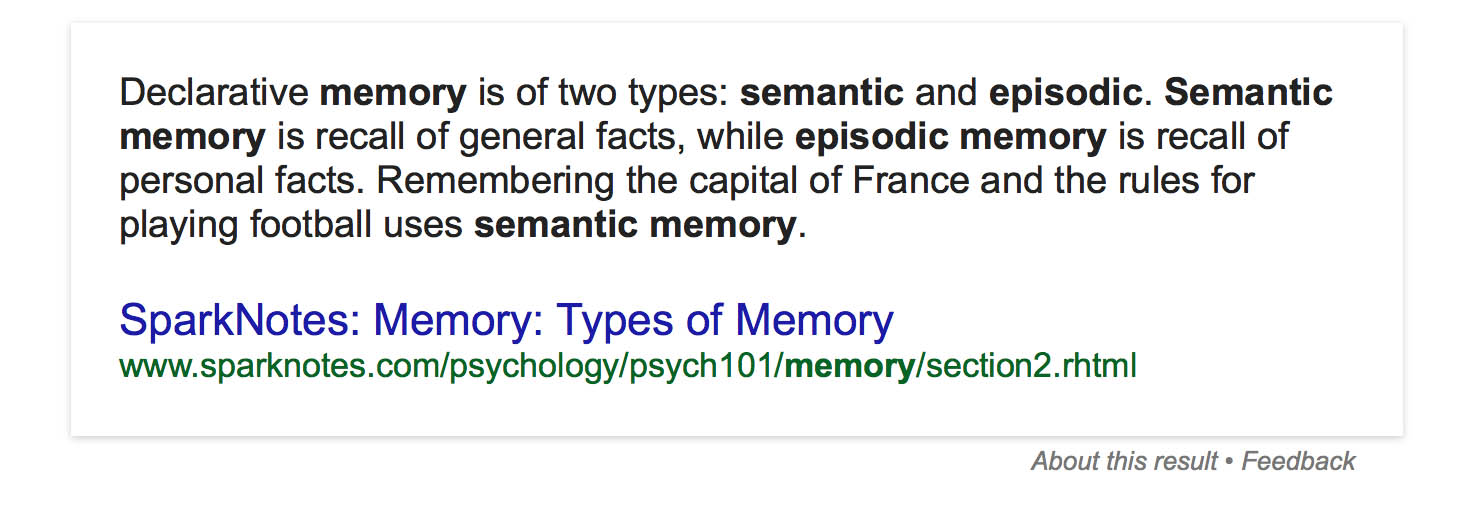
I could immerse you in lots of complicated neuropsychology, but this handy definition I got off Google is accurate and will suffice for the purposes of the blogpost.
This itself is controversial – but say personal facts here include events relating to my past. But you see the point you can’t just conflate this all as “memories and facts” as per the wording of the analogy in ‘Dementia Friends’.
This matters as the part of the brain thought to be implicated in loss of semantic information is in a totally different place to begin with with that implicated in the loss of episodic information.
Semantic memory is really important for our knowledge about categories of things, aka facts.
“In contrast, the term semantic memory applies to our ‘knowledge of the world’, including the meaning of vocabulary, concepts and facts: information which is retrieved without recalling when and where it was learnt (Patterson and Hodges, 2000). Tulving (1972, 1983) proposed that these two types of memory were psychologically and neurologically distinct and that amnesia was the result of damage to the episodic memory system. Moreover, Scoville and Milner’s data suggested a critical role of the medial temporal lobe, in particular the hippocampus, in this type of memory (Scoville and Milner, 1957).”
Problem 3 – the issue to do with loss of memory for facts and where this takes place
The bookcase analogy as drafted in Dementia Friends talks about the hippocampus being where “memories or facts” is pretty wrong – episodic memory fine though.
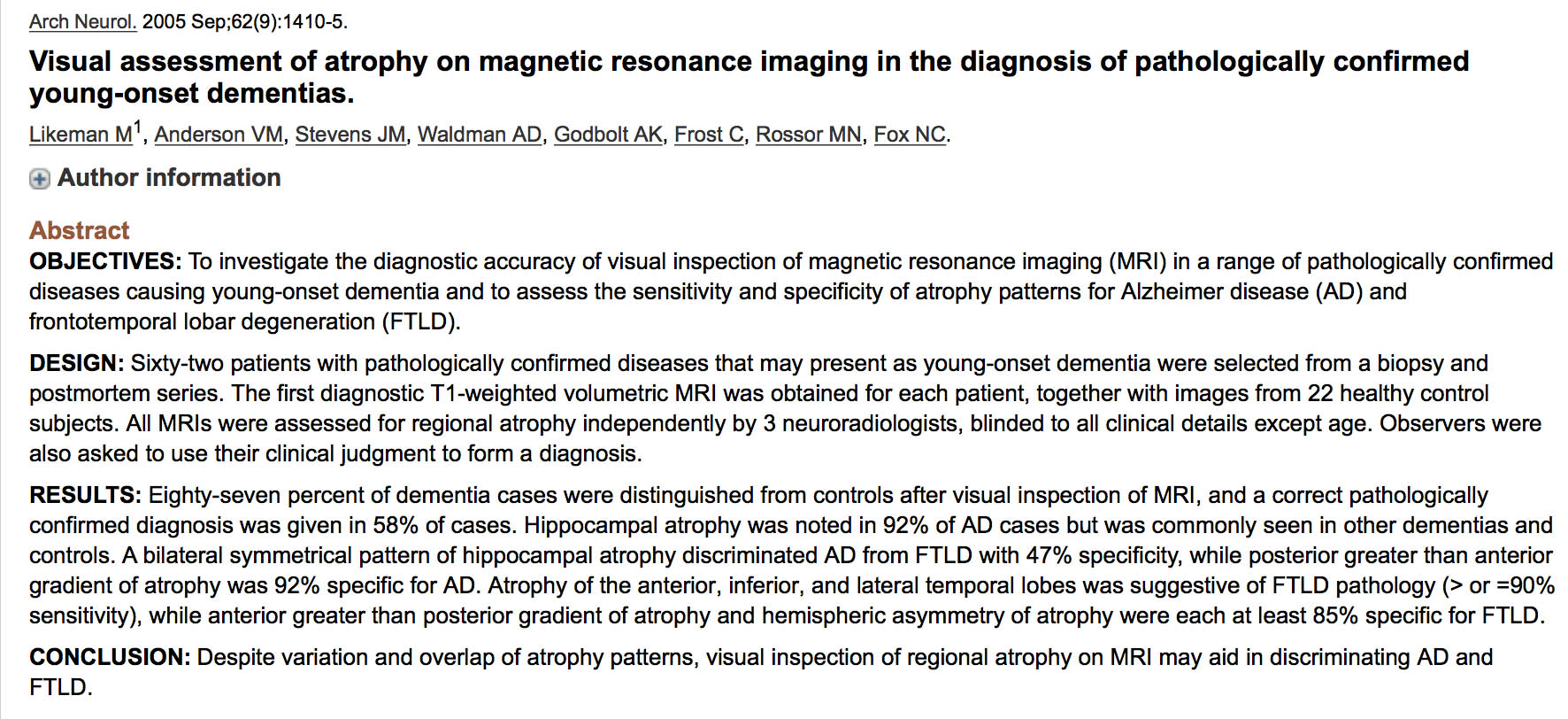
Semantic dementia is thought to start off around the anterior inferior temporal lobe, whereas episodic dementias like Alzheimer’s disease (initially) start off around the hippocampus.
And as I say earlier in this blogpost there are different ‘gradients’ of memory loss according to different types of dementia. The bookcase analogy refers to ‘dementia’, but as we know there are at least a hundred different causes of dementia – not just Alzheimer’s disease.
It’s OK-ish to call it the central part of episodic memory loss “the hippocampus” – though it’s really the general area of the hippocampus (in the medial temporal lobe) – as shown in the classic paper here.
The wider use of analogies in teaching
I don’t have any problem with Gemma Jones’ analogy.
You can read it in her excellent book ‘Care-giving in dementia’ here.
My only problem is that “Dementia Friends” is meant to be a social movement – and not where you literally have clones of volunteers learning a script albeit to fulfil the purpose of an information session.
There is a philosophy that Dementia Friends is delivery of a ‘product’ – conveniently commodified in a standard way to raise ‘awareness’ and to reduce stigma and awareness.
I think the original analogy is useful.
If it is so important for the wording to be homogenised, so that every information session is delivering the ‘same product’ albeit neuroscientifically somewhat wrong, why not just allow playing an official DVD of it?
But there comes a point where versions of analogies can be actively misleading, and does not actually portray accurately what happens in the dementias.
For some not others the truth will matter (particularly if ‘you do research’ another government aim).
The term “challenging behaviours” was a very unfortunate import from the field of intellectual disabilities to dementia, necessitating the query “for whom behaviours are ‘challenging’?” Many people with dementia find behaviours of the medical profession ‘challenging’, being polite.
But a ‘good import’, arguably, would be the notion of “Portage”.
The name Portage comes from the town of Wisconsin, USA where the a home teaching scheme was developed in the 1970’s.
Portage is a home visiting educational service for pre-school children with additional needs. These may be learning difficulties, developmental delay or physical difficulties.
The “Portage Home Visitor” works with parents in their home because young children initially learn best in the security of their own environment, with the people who know them. In this way the best teaching programmes can be developed for every child.
Interesting ‘success stories’ exist elsewhere in the world too.
Founded in the Netherlands in 2006/07, Buurtzorg is a unique district nursing system which has garnered international acclaim for being entirely nurse-led and cost effective.
Prior to Buurtzorg, home care services in the Netherlands were fragmented with patients being cared for by multiple practitioners and providers.
Ongoing financial pressures within the health sector have led to home care providers cutting costs by employing a low-paid and poorly skilled workforce who were unable to properly care for patients with co-morbidities, leading to a decline in patient health and satisfaction. This is a problem which England shares too.
Indeed, a recent report last week from the International Longevity Centre discussed again the significance of co-morbidities in dementia Buurtzorg’s solution has to give its community district nurses far greater control over patient care – a factor which it attributes as key for its rapid growth.
Until recently, neither persons with dementia nor national dementia societies had used their right of access to UN Convention on Rights for People with Disabilities to which they are legally entitled defined by the scope of Article 1.
“Persons with disabilities include those who have long-term physical, mental, intellectual or sensory impairments which in interaction with various barriers may hinder their full and effective participation in society on an equal basis with others.”
Prof Peter Mittler CBE, Advisor for Human Rights for Dementia Alliance International, writes:
“At the recent WHO Ministerial Conference on Dementia, Kate Swaffer [Chair of Dementia Alliance International] set the ball rolling at the opening session by including ‘Access to CRPD’ as one of DAI’s demands.”
It was remarked that an aspiration should be that “policies, plans, programmes, interventions and actions are sensitive to the needs, expectations and human rights of people living with dementia and their caregivers“.
The concept of ‘post-diagnostic support’ (soothing, but in reality weak words for England’s policy in dementia) needs to be re-configured as a rehabilitation pathway.
Essential to the re-framing of the whole discussion is getting rid of the idea that ‘post diagnostic support’ is a haphazard AFTER THOUGHT – and that the medical model is KING through the strategic placement of ‘diagnosis’. Sure, without the diagnosis, nothing further can happen, but the issue is that even with the diagnosis some people are experiencing next to nothing in care in England, and even if they experience some care it is fragmented and disjointed.
There is no better introduction into how the sequelae of the dementia diagnosis can be so positively destructive than Kate Swaffer’s own description of ‘prescribed disengagement™’ in a prominent journal here.
This pathway begins possibly even at the time of contemplation of the diagnosis with extensive support to after when the diagnosis has been given. At all times, the recipients of that diagnosis (including immediate closest) should be opportunities to ask questions and discuss ways in which care and/or support can be given.
Enablement should be the goal now.
Other jurisdictions, for example Queensland in Australia, have been outstanding in leading – see this report, for example, here.
A ‘pathway’ is a somewhat cranky technocratic word, and could be considered entirely inappropriate in the context of an English government intent on cutting state provision of a ‘safety net’. But at best it might provide decision points which might be legitimately and reasonably expected at points in a personal integrated care and support plan following diagnosis.
The lack of national adoption of pathways, entirely due to entirely political reasons, and despite a plethora of evidence to prove pathways can promote health and wellbeing for patients with dementia and carers, has been noteworthy here in England, tragically.
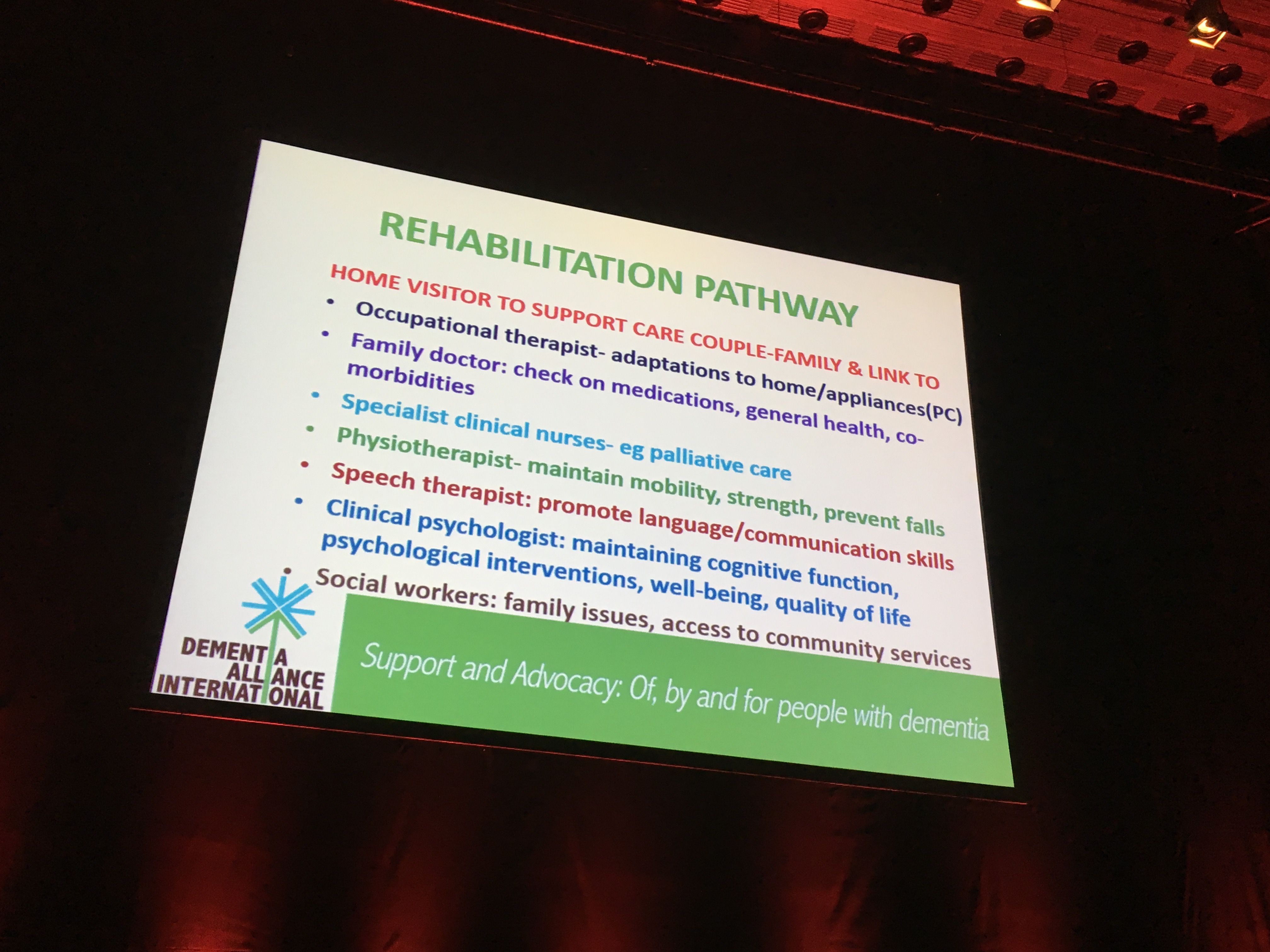
Notwithstanding, a rehabilitation pathway would provide access to a wide range of specialists. These might include, for example, the following personnel, no one part of the ‘workforce’ being “more important” than others, promoting independence as part of an inclusive, accessible community for all.
People with dementia and those closest to them themselves have an important rôle to ply in co-designing pathways in genuine co-production, if they are working on an equal and reciprocal basis.
Specialist clinical nurses who can act from the point of diagnosis providing continuity of care are important are sufficient in themselves. They are especially helpful in applying palliative care principles. For too long, it has been dismissed that dementia is a terminal condition, thus denying many people with dementia equitable access to palliative approaches. Furthermore, it has been insufficiently addressed that people with dementia have a right to the highest standards of health from the NHS, regardless of setting.
These trained clinical nursing specialists are also extremely well placed to sort out issues arising from co-morbidities in health and illness, helping to head off avoidable acute admissions to hospital, or premature inappropriate transfer to residential care. Admiral nurses are also pivotal in helping coping strategies, essential in averting ‘crises’ in dementia care.
Other specialists might include:
Occupational therapists are pivotal, I feel; this rôle could include wider implications of he diagnosis and a discussion possible adaptations to the home and domestic appliances, and various forms of technology and innovations. A particular challenge, for example, might be to negotiate higher order problems in processing of the senses, including vision, as per posterior cortical atrophy.
Physiotherapists to maintain mobility and promote physical exercise.
Speech and language therapists to promote language and communication, especially important in Alzheimer’s disease and temporal forms of frontotemporal dementia, as well as to ensure safe swallowing following particular vascular events.
Clinical neuropsychologists to advise on adjustment to diagnosis, improving and maintaining cognitive functioning, promoting thought diversity and an ‘assets based approach’ where people’s skills can be best utilised.
Dieticians: a healthy diet is relevant in the progression of dementia, and especially so arguably for vascular dementia and Alzheimer’s disease. Also, latterly, particular attention has been given to optimising eating environments as part of the ‘healthy eating’ ethos.
Social workers are much utilised in my opinion, and I should like to see a much wider rôle than in safeguarding or crises, though I think capacity building in the workforce of social workers with a specialist interest in mental health issues might be helpful. I think social work practitioners are vital in the promotion of wellbeing, in enabling and protecting people with dementia, and provide access to community resources perhaps including personal budgets for some,
Pharmacists. Many medications can worsen cognitive symptoms potentially and act as risk to physical health indeed, and inappropriate polypharmacy needs to be reviewed by specialists in pharmacy.
Certainly medical professionals in primary and secondary care are vital where another plank of integration is needed, to ensure people with dementia and their closest genuinely do get the right care in the right time at the right place. I have no doubt primary care, with their wide experience of medicine, and upholding a proactive stance too, would be vital in community based rehabilitation, including general practitioners. But the current service issues in resources for, recruitment to, excessive regulation of, and access to general practitioners in England cannot be ignored.
The UN 2016-2030 Sustainable Development Goals were launched with a commitment to “Leave No One Behind”, a similar theme having been ‘no decision about us without us’. I have a concern that the poorly named “dementia friendly communities”, being aimed at being politically inoffensive by the chief cheerleaders in England, and being so cost neutral, does not do enough to resolve social inequalities in reality.
We know this is a danger, say, for housing. But worldwide extrapolation of inequity would be disaster, particularly when we consider the number of people thought to be living with dementia in low and middle income countries around the world.
All too easily ‘dementia friendly communities’ can become a strapline as a sticking plaster for cuts elsewhere in the Big Society, to secure a quickie competitive advantage in marketing – this is indeed addressed in this briefing from March 2015 here:
“There have been concerns that the target created incentives for governments to focus on‘low hanging fruit’ rather than those most in need.”
As a consequence of sustained advocacy, persons with disabilities are now clearly included in the 17 SDGs and 169 implementation indicators. Although the needs of older persons are recognised, persons with dementia are in grave risk of being overlooked.
It is likely that, if Big Pharma are successful in producing orphan drugs capable of being regulated and distributed, there will be an inequity regarding domestic recommendations about making these drugs available. The ‘economics of rescue’ doctrine means that there should be no stone unturned in providing medications in palliative care; but NICE will have other views on the greatest benefit for the largest number of people in their econometric ullitarian cost-benefit analysis.
It is indeed likely that persons with dementia in Low and Middle Income Countries should be able to benefit from the long established WHO Community-Based Rehabilitation (CBR) Programme described here.
“Community-based rehabilitation (CBR) was initiated by WHO following the Declaration of Alma-Ata in 1978 in an effort to enhance the quality of life for people with disabilities and their families; meet their basic needs; and ensure their inclusion and participation. While initially a strategy to increase access to rehabilitation services in resource-constrained settings, CBR is now a multisectoral approach working to improve the equalization of opportunities and social inclusion of people with disabilities while combating the perpetual cycle of poverty and disability. CBR is implemented through the combined efforts of people with disabilities, their families and communities, and relevant government and non-government health, education, vocational, social and other services.”
As a clear example as what could be achieved by engaging trained professionals too into English dementia policy, the Royal College of Physicians of London have been leaders too.
“This Future Hospital Programme case study describes how the Torbay and South Devon NHS Foundation Trust is fulfilling their aim of achieving stroke rehabilitation 7 days a week in both the Stroke Rehabilitation Unit and surrounding areas.”
Stroke care, like cancer care, is in a different place to dementia.
And we know why. The only hope in English policy appears to be some chosen ones selectively adding fertiliser to a few flowers blooming when the entire garden had actually been devoid of being watered for several years. And this needs fixing the gardener.
Unfortunately, people who are less skilled – but who are ‘advising’ or ‘supporting’ – might possibly insufficient alone to service needs of people living with dementia and carers, even if they meet the needs of certain charities, but they do serve a useful function in service provision. Quality is essential for enablement.
–
Please come to see my talk in the policy stream of the Alzheimer’s Disease International conference this week in Budapest.
It was with a rather heavy heart that I decided to launch my own society on dementia earlier this week.
A few years ago, I applied to be an information officer in a well known dementia society. I wasn’t shortlisted, and at the time it felt to be a personal setback. Nonetheless, I was determined to do something for education about dementia. Last summer, I also applied in good faith for a non-paid position in another dementia charity, which was equally a waste of my time.
I have been a junior physician at the National Hospital for Neurology and Neurosurgery at Queen Square coming close to nearly 15 years ago. I remember as part of my training learning about patients of mine, such as a young man with a progressive decline in memory and change in personality. His diagnosis was HIV dementia.
A few years previously, I completed my own doctoral thesis in Cambridge in quite a common type of dementia for people aged 65, called the behavioural variant of frontotemporal dementia . I was lucky in that my big result from this thesis has now been replicated by many research groups around the world and is even occasionally cited in specialist textbooks in dementia.
In my personal life, a lot has changed for me. I became physically disabled in an acute event nine years ago, and I nearly lost my life. The whole experience, and numerous other events and experiences, has made me quite resilient now. Undeterred, I went on to obtain postgraduate degrees in management and in law.
Some time ago though, I feel I had decided to walk away from the ‘greasy pole’ anyway. I am regulated by both the medical and legal professions – but personal circumstances mean that my goals are very different now to fifteen years ago.
Like many people, I would like to make a difference, but, like some people, I have very limited scope for doing so. Financially challenged, I have saved up money to go to the Alzheimer’s Disease International conference in Budapest in fewer than ten days’ time. I’m giving a talk there on human rights, and my best friend Kate Swaffer arrived there today.
But I have been thinking a lot about Paul Mason’s work entitled ‘PostCapitalism’. It is an epic I feel and definitely an intellectual tour de force.
It has made me think about paid jobs and the public good. There are people who write open source software for hardly any money, and the quality of their work is good.
There is a mismatch between income and performance. I don’t think people who get the highest salaries in dementia and given recognition societally are the people who have contributed most value to dementia. In fact, I think the relationship is sometimes (but not always) the opposite.
There are people who have written Wikipedia pages for nothing for much of their life. As a comparison, I nearly ended up making a financial loss in royalties in my second book on dementia because the index which I paid for myself cost so much. I enjoy writing about dementia though – my first book won best book of the year award in the BMA Awards for the health and social care category.
I do think I.T. has totally changed things around. It is easy to disseminate material for free now; some “goods” are not unreplaceable. If I park in car parking space, that takes up the space for somebody else. If I eat a banana, that deprives somebody else of a banana. If I share pdfs on the internet for free, I deprive no-one.
Back to the main issue, I do not need validation through being important. There are personal issues about the approach of the harnessing of opinion I dislike strongly. Co-production should be equal and reciprocal, not effectively ‘asset stripping’ of social capital to make a profit as Alison Cameron put it earlier today. (I thank Alison Cameron for bringing out the best in me in focusing on codesign and coproduction particularly.)
But while I am still alive, I would like to give something back. Anything can happen to anyone at any time, so I am going to build from scratch a website all about dementia and those closest to them.
I am lucky I have some knowledge about dementia, and I will see where this takes me. I can spot blind spots in policy through medical training which many people in Big Charity can’t. If you have any views on what should be on this website, please do feel free to contact me. I ultimately want to make a society, not concerned with, or looking for surpluses or profits, so any thoughts on that are welcome too.
I am an academic physician specialising in dementia. I write this blogpost as a guide to people who might be interested in my views on where English dementia policy needs to head.
I spend most of my time studying the latest papers around the world in dementia and other cognitive disorders from here and around the world. I also seek out the views of people who’ve received a diagnosis of dementia, and live daily with the condition. I haven’t ‘engaged’ them, or ‘involved’ them. They’re my friends, and I chat with them. I am also interested in the beliefs, concerns and expectations of those closest to them.
I’m slightly fed up of people promoting themselves in English policy to be blunt. These are people who feel their own self importance is more important than the needs of people with dementia and those around them. I am sick of how dementia has become an ‘industry’.
Conversely, people who have a diagnosis diagnosed below the age of 65 need professional help and guidance to help them navigate through the effects of the diagnosis on their social networks and/or employment.
We can’t leave people languishing with such little support in parts of the country – and we don’t just need a high volume of low quality diagnoses. All diagnoses have to be correct as far as possible, and I suggest committing resources for training up GPs or specialist nurses who already have a good knowledge of general medicine to assist with this.
The policy thread of ‘dementia friendly communities’ is well intended. For me, however, it smacks too much of the ‘does he take sugar?’ phenomenon. Maybe it’s the case that I am indeed supersensitive to this. I am physically disabled, and do tend to notice how people’s attitudes can be incorrectly formed on this basis.
One of the most inspiring talks I heard recently was by Simon Baron-Cohen, a chair in psychology at Cambridge. Simon was talking at the LSE, but he was my first ever supervisor at Cambridge. He was talking about his own specialism – autism and Asperger’s Spectrum conditions.
He mentioned Gary Mackinnon – and how despite hacking into the US top security systems Gary wasn’t (and isn’t) intinsically a bad man – Gary had left electronic post it notes every level he had breached for the benefit of the CIA.
Simon urged a reframing of autism as a condition which presented both disabilities but aptitudes. I feel we need a similar reframing and reforming of English dementia policy. I don’t wish to get into an aggressive discussion of social v medical model, but the framing of our policy is poor. The term ‘post diagnostic support’ for many does not inspire confidence. What would inspire confidence is a practical infrastructure for enablement, comparable to what would be provided in rehabilitation following a physical disability.
We need to harness the opportunities of non-medics, but who have a huge amount to contribute – ranging from occupational therapists who can help with assistive technologies, or speech and language therapists who can help with communication or swallowing difficulties?
Dementia not being treated as seriously as cancer is a real problem. We can’t go on producing policy annually for the benefit of one Big Charity, producing one million, then two million, then three million “dementia friends”. We need to have clearly signposted choice points in enablement. Dementia policy needs a substantial consensus on care pathways – to give some certainty, but also to include some flexibility.
There needs to be some structure too. Society should be inclusive, but there are limitations to overegging the ‘dementia friendly communities’. Communities should be inclusive and accessible to all. You can’t “spot” a person with dementia in the community by a sticker on his head, or by the way he’s acting.
Research needs to be more balanced, including good quality research into care as well as the brilliant cellular and molecular research. But humility is needed to accept that all research is worthy in itself, irrespective of whether drug therapies are found.
People who say we don’t have to choose between cure and cure need to factor into their views that social care funding is on its knees. The NHS also has insufficient monies to perform optimally. All persons with dementia are entitled to the best quality healthcare, whether they’re in hospital, at home, in a hospice, or in a care home. Cosying up to government and then complaining to fix dementia care is – no ifs or buts – weak leadership.
Access to the right quality care is important. Some of the work can be done by people with not much more than a NVQ in advising or supporting, but we do fundamentally need more properly trained clinical specialist nurses ensuring continuity of care and higher level care (e.g. in caring for those caring, palliative care, incontinence). One reason for this is a reluctance to consider dementia as a terminal illness – but the other sadly is selfish brutal politics. You unfortunately pay for what you get.
Above all, the lived experience of all people living with dementia and their closest is paramount. We don’t need to pour huge amounts of money into middle men into measuring this. We simply need to listen.