People still want to have their visions, and also their key performance indicators, in the modern NHS and social care. This is otherwise known as “having your cake and eating it”.
For all the ‘feel good factor’ of power transitioning ‘to the edge’, it is still nonetheless the case that people with the long business titles will be invited to give talks at conferences as speakers, and those who don’t won’t (and can’t often attend due to the ensuing financial barrier). Often these are not the people who know the day-to-day running of health and social care.
I am basically hoping that the discipline of ‘change’ will now become paralysed through being over-analysed. The discussion of change, I am sure well intentioned, has become so overcharged with terminology and jargon such as ‘boat rockers’ and ‘change catalyst’, so as to be exclusionary, non-accessible and non-inclusive.
There is little which is certain about life other than death and taxes. But I am sure that junior doctors are too overworked to think about their work as being ‘rebels’. Junior doctors do not enjoy being in a hierarchy, but they are. Otherwise, it would be the case they do not need to go on strike to achieve fair terms and conditions for their huge work commitments.
Contrast this to my experience.
I really enjoyed our ‘meet up’ last week in Llandudno, North Wales. In one session, we were sitting on different tables, with a non-contrived mix of people living with dementia, carers, academics, commissioners, and other interested parties. I found that people living with dementia and carers easily found themselves rising to the top of the most valuable contributions, despite all the talk of ‘flattening hierarchies’.
I think the ‘flattening hierarchies’ narrative is misplaced.
I believe that people with dementia and those closest to them ought to be listened first, when it comes to working out whether processes and systems for research and service provision are working.
I think the ‘don’t ask for permission’ meme is inadvertently wrongly positioned.
I think the ‘don’t ask for permission’ meme inadvertently assumes that the wounded party is necessarily already having to ask for permission. I know plenty of people living with dementia who do not need to be told that they are allowed to be leaders. They are not sitting around waiting to be told – otherwise they would be taking on a rôle of submission.
A ‘call to action’ is fine, but not what is fine is the bandwagon effect of people absorbed into a massive groupthink making it harder to make a very small change at a local level. The group think of becoming ‘dementia friendly’ according to one large organisation can easily see wilful blindness to the closure of respite services or provision of a service of clinical specialist nurses locally.
For me, ‘change’ has become a cult. You can spot identical memes on Twitter, and it is getting nauseating. I dread to think what would have happened if Martin Luther King and Mahatma Gandhi had processed mapped their struggles onto a ‘call to action’.
Likewise, people living with dementia and carers beware.
Over time, I’ve learnt that you can do a lot more harm than good in being critical over other people’s initiatives in dementia. I really do believe it’s essential to be supportive, and to give recognition to other people’s efforts and hard work. The ‘virtual reality centre’ is of course no exception to this for me.
This news article will give you a good introduction to the innovation (as well as the video above).
“Aged care workers can now experience what it feels like to live with dementia at an Australian-first dementia learning centre that uses light, sound, colour, visual content and serious gaming technology to create a virtual reality.
The Perc Walkley Dementia Learning Centre is a key feature of Alzheimer’s Australia Vic’s new facility in Parkville, Melbourne, which was opened by Alzheimer’s Australia National President Ita Buttrose on Wednesday.
The training centre features doughnut shaped mood lighting, a 10 metre by two metre projection wall, an interactive touch screen and gesture-sensor technology.
It allows students to be immersed in the virtual world of someone with dementia and experience the cognitive and perceptual difficulties they might face in their daily life that can make ordinary tasks challenging or dangerous.”
There is much to laud here. How persons living with dementia and carers, very often family members including spouses, deal with risk in the community is of huge interest worldwide. Take for example the brilliant work of the Cognitive Decline Partnership Centre based at Sydney which has this as one of its research goals.
The description of course seems perfectly plausible.
“Aged care workers can now experience what it feels like to live with dementia at an Australian-first dementia learning centre that uses light, sound, colour, visual content and serious gaming technology to create a virtual reality.
The Perc Walkley Dementia Learning Centre is a key feature of Alzheimer’s Australia Vic’s new facility in Parkville, Melbourne, which was opened by Alzheimer’s Australia National President Ita Buttrose on Wednesday.”
But sorry to be the first to rain on this parade but we currently have a very scant knowledge of the perception of objects in dementia.
There’s no doubt that cognitive neurologists have not given due regard to sensory perceptual effects of living with dementia. Agnes Houston and Donna Houston have been educating others about how dementia can affect the senses, in remarkable work which the Life Changes Trust have supported. The feedback from other people living with dementia has shown that many people have experienced sensory phenomena, with the medical profession barely batting an eyelid. Sensory phenomena can indeed be marked phenomena of some young onset dementias, though I am not one to define any person by their medical label. For example, in diffuse lewy Body dementia, sensory hallucinations can be common. In the posterior cortical atrophy, there can be some marked differences in the perception of space. I feel, in common with many others, what we call the posterior cortical atrophy is one common presentation of the dementia of Alzheimer type in an earlier age group (typically 55-60).
But likewise, not everyone living with dementia experiences marked sensory changes early one. It would be very unlikely for somebody with the behavioural variant frontotemporal dementia, known for changes in personality and behaviour, and relatively normal cognition otherwise, to experience marked perceptual changes. In my own Brain paper from 1999, indeed, I found no evidence for sensory disturbances. This would be entirely expected, as this type of dementia affects early on the very front of the brain, very far from the parts of the brain further back which process vision and other senses.
So the sentiments expressed in these paragraphs came somewhat as a surprise to me:
“Aged care workers can now experience what it feels like to live with dementia at an Australian-first dementia learning centre that uses light, sound, colour, visual content and serious gaming technology to create a virtual reality.
The Perc Walkley Dementia Learning Centre is a key feature of Alzheimer’s Australia Vic’s new facility in Parkville, Melbourne, which was opened by Alzheimer’s Australia National President Ita Buttrose on Wednesday.””
The project sits uneasily with the conflation of dementia and ageing. Not everyone with dementia is old, and yet it is an altogether different thing to say someone has visual problems due to cataracts (common causes being age, diabetes and smoking). This can cause fogging of the image and colour changes, as Monet himself noticed. It’s unlikely for somebody just to be living with dementia; for example, somebody might be living with dementia as well as with a previous stroke, and the stroke might cause visual problems of their own such as field defects.
I do not deny the value of public-private partnerships, but I feel I have to raise the scrutiny with which scarce resources for dementia care are allocated into projects such as these with questionable scientific and clinical merit. The initiative raises concerns for me with the due diligence with which other professionals are involved. I feel any reasonable cognitive neurologist would have come to the same conclusions as me. I am more concerned about the ‘engagement’ (suboptimal term) of people actually living with dementia. Sure, it’s not possible to consult all 47 million people living with dementia around the world, but people living with dementia have different ‘faces’, depending on how much a cause of dementia has affected the brain; and there are at least 120 different causes of dementia, medically, depending on how you count them,
So unfortunately this project for me, and freedom of expression is important, raises the grim reality of ‘the wrong type of awareness of dementia’.
But I do agree with the write-up that this is fun, and – ironically – this is the bit of the pitch which has the most scientific validity for me.
“While conventional video games are made to entertain, serious games use traditional gaming technology and techniques to create tools for education or a particular purpose, said Norman Wang, the founder of Opaque MultiMedia, which is developing the virtual dementia experience (VDE).
“Normally people can understand dementia at an intellectual level. We are using immersive virtual reality so people can understand it at a visceral level,” Mr Wang said.”
There’s indeed a lot in ‘gamification‘ to recommend.
The issue here is we are much better at learning stuff if it engages neural circuitry involved in arousal, emotion and motivation (this is simply because it engages different parts of the brain which help to consolidate memories).
And it’s important not to throw the baby out with the bathwater in this case. For any innovation to take off, you need to see what real adoption is like. For all I know, this innovation will be really helpful to carers.
I have noticed that people living with dementia, of whatever background, can have real issues with features in the environment, such as ‘garish’ carpets. This is utterly genuine, and explains the rationale of the global approach of ‘dementia friendly communities’.
This makes sense to me.
““We can create special effects, such as have surfaces that ripple or change colour,” Mr Wang said.”
But above all this innovation does not get round the somewhat philosophical problem of ‘Do you see what I see?’ This problem, often articulated as ‘Will you hear an apple dropping in a forest the same way as me?’, is a very difficult question of philosophy of mind, a favourite of undergraduate finalists in philosophy exams all around the world. We should be very wary of attributing perceptions to people with dementia, in the same way we attribute other functions of the brain, on the one hand. On the other hand, identifying what may be ‘deficits’ in the thinking of others may help us best to retrofit ‘reasonable adjustments’ entirely consistent with the attitude (and legal fact) of dementia as a disability.
Many thanks to Fenella Lemonsky (@organiclemon) for this helpful review of my book in “Mental Health Today) [here is the link to the original article.]
I find reviews like this a useful steer on future work. Academics can be notorious in misjudging the ‘mood music’ of the main drivers behind the service: people who use the services, which in my case are people living with dementia, their friends and family and other carers. I am in a privileged position in having access to thousands of peer-reviewed papers, but also feel that I have learnt a lot about the dementias from people living after a diagnosis. My knowledge of dementia has vastly improved since I took myself away from the medical lens, and adopted a viewpoint of other professionals and practitioners and people living with disability.
Shibley Rahman, 2014, CRC Press, ISBN 978-1908911971, £29.99
There has been much written and spoken about dementia in the media recently as a result of the government’s Dementia Strategy, which aims to help those with dementia, their families, professionals and carers be more responsive to needs.
In this context, Living Better with Dementia, by Dr Shibley Rahman, a dementia expert who is qualified in medicine, neuroscience and law, is highly relevant.
Initially, Rahman talks about the stigma of dementia and how this has remained through the past century, despite dementia becoming better understood and having a more positive outlook in recent years. While dementia and the whole management perspective can appear a challenge as the older population survives longer, this book is encouraging and positive. Specific medication that delays the onset of dementia symptoms and other medication like antipsychotics are discussed at length, including their use in nursing and care homes and how specific practices that have no evidence base can be challenged.
Two chapters that for me stuck out as very important were on young onset dementia and on antipsychotics and innovation. Young onset dementia was first explained to me at the author’s book launch, where nurse lecturer Kate Swaffer from Australia, who has young onset dementia, gave a moving talk. The impact is huge for the individual, their family and peer network as well as professionals. It affects employment, career opportunities and has a huge stigma attached to it as it is still often misunderstood. This is all discussed in the book.
The use of antipsychotics and care homes is also discussed at length. This is an important chapter, especially for those who look after those going into residential care, and it can enable them be on alert to good practice and how to spot where medication is used inappropriately. Antipsychotics use in care homes is a complex issue. In many cases careful use can ease distress and agitation, but there seems to be concerning evidence that there is over-prescribing of antipsychotics where behavioural treatments are more appropriate. Using extensive research, Rahman explains why using antipsychotics needs careful thought.
Other chapters focus on deprivation of liberty, sporting memories, global view and leadership strategies.
This is a well-written, extensively researched, easy to read and important book for anyone interested or working with dementia.
Rating: Highly recommended.
Review by Fenella Lemonsky, mental health service user researcher
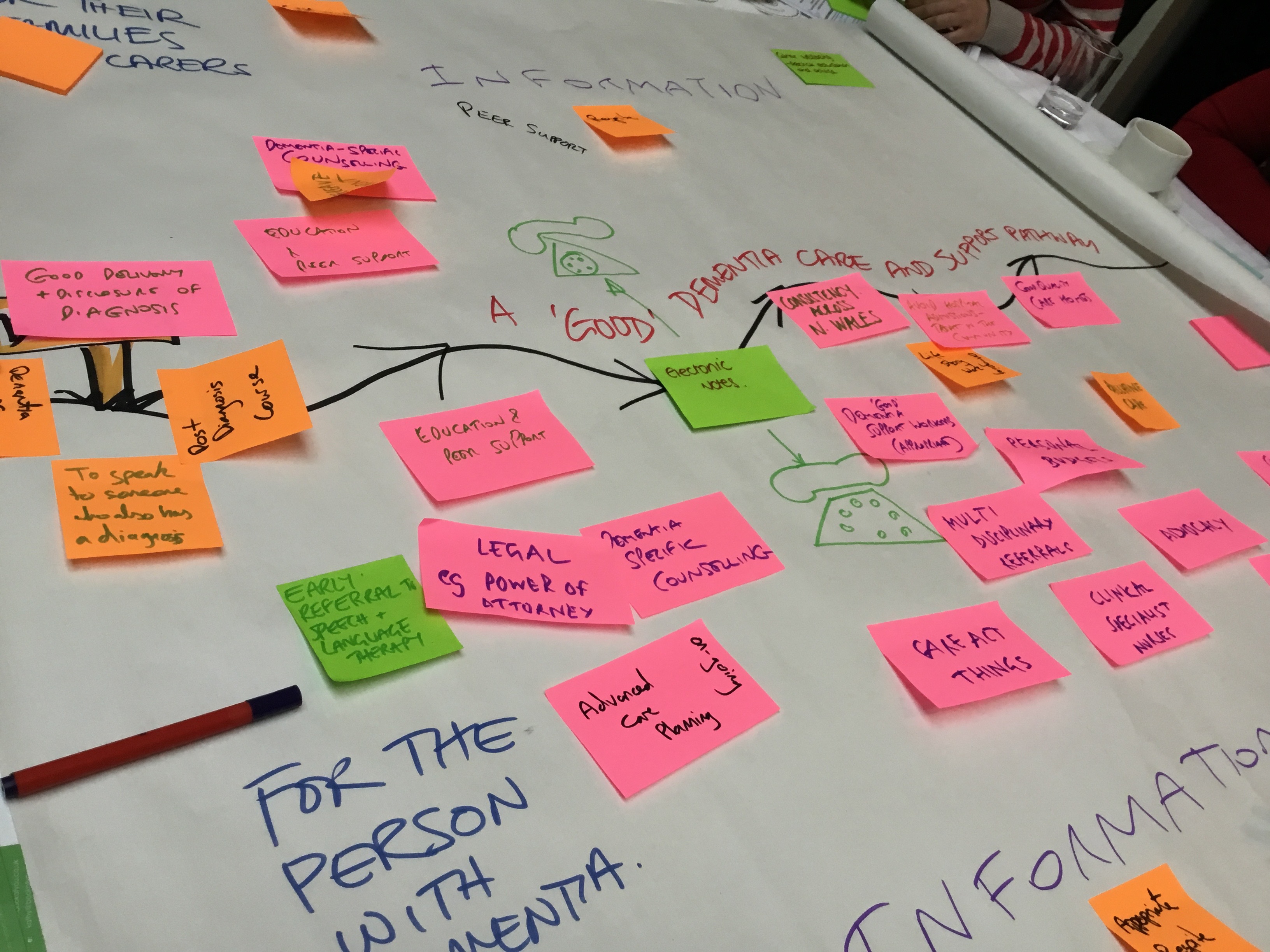
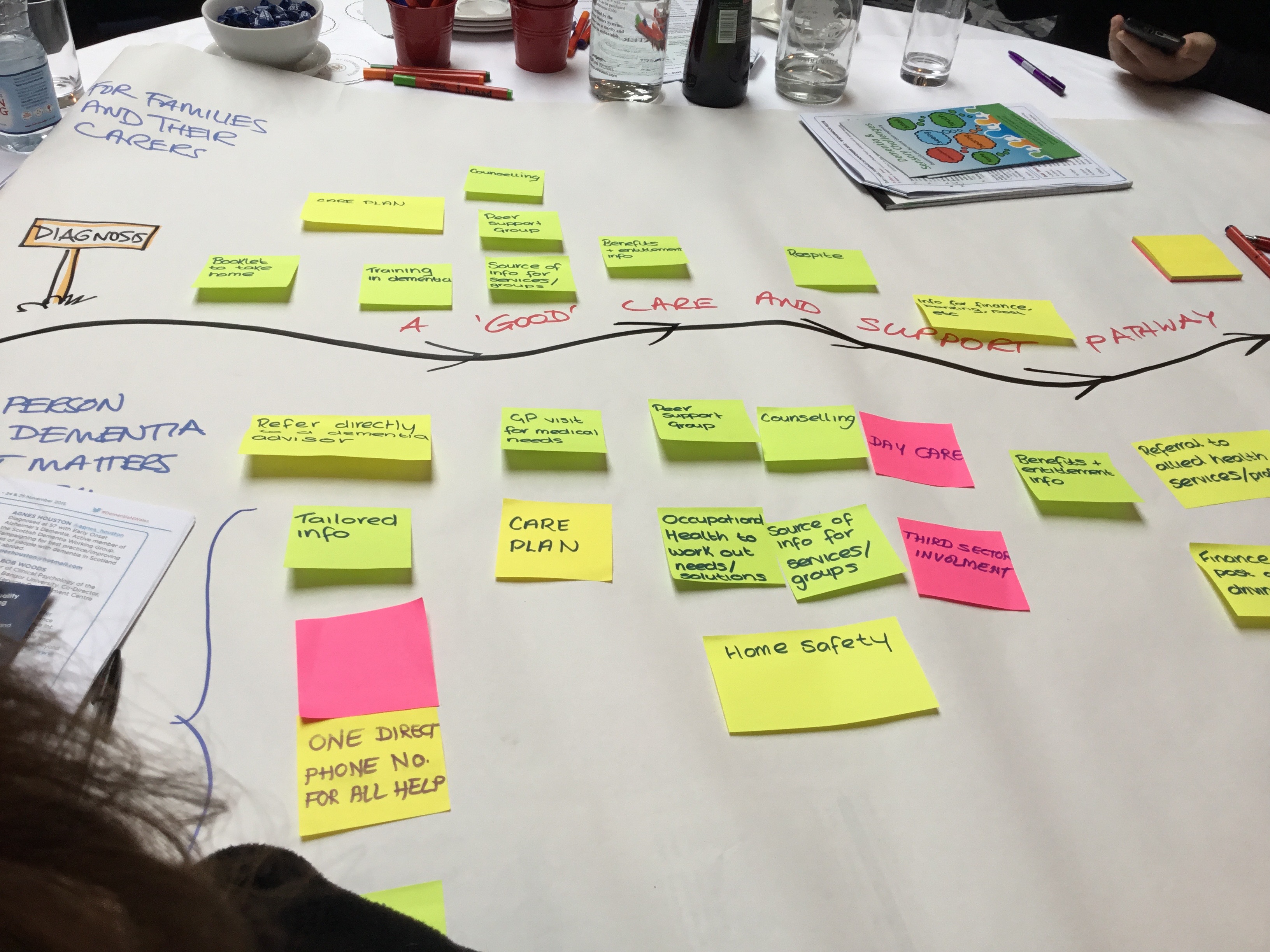
Fran O’Hara, Pam Luckock, Chris Roberts and Jayne Goodrick, about 15 people with dementia, at least 15 family carers, various people in various disciplines in dementia care including the third sector promoting living better with dementia, and other interested parties, proved it this week.
The dementia conference is dead. Long live the meet up.
We got off to a flying start. There was no ‘conference dinner’. We instead all sat where we wanted to in a rectangular circle (you get my drift). My best friend, Chris Roberts, sat next to Jeremy Hughes. I was about to take a photo of Chris talking to the person on his right, whom he really liked a lot, until I realised it was Jeremy. And I thought I’d leave Jeremy in peace – he is after all the CEO of the Alzheimer’s Society!
I adore Prof Bob Woods – his advice to Chris when he left on the last day was, “Watch out for this man!” (laughing, but pointing at ME). Bob is basically an encyclopaedia, but very nice with it. I mentioned to Bob how in fact I was citing him during my own PhD – which was a very long time ago. Bob said, “Good! Cos I started when I was 5.”
I asked Bob whether he ‘believed in’ meaningful activities – “very much so – they’re better than meaningless activities” came the reply.
I can’t really explain it – but there is a huge bond and solidarity when friends of mine living with dementia meet up and their closest ones. You can’t ‘fake it’.
Kate Roberts, Chris Roberts and Jayne Roberts did a wonderful initial session. In a brilliant talk (and it was apparently totally scripted by her), Kate (=Chris’ daughter) included, “Mum is my rock and Dad is my hero.” You could hear Jayne’s voice croak audibly with emotion.
I won’t give the ‘game away’, but George Rook gave a wonderful talk on the communication and disclosure of the diagnosis from a patient’s perspective:
Agnes Houston’s work, discussed too by Donna Houston, was a real hit. Agnes said it had all been possible through people with dementia giving up their precious time, and with generous support from the Life Changes Trust. You see Agnes MBE is the best – Agnes will be going with family to Buckingham Palace on 18th December 2015 – and I’ll be supporting from afar.
Olwen Williams gave a very good mini-speech on a topic which I have a strong interest in – the “Future Hospitals” initiative from the Royal Colleges of Physicians, which looks at the rôle of the hospital in an integrated person-centred care system which sees people in the right place, right time and right way.
Really loved chatting with Ruth Eley for a long time for the first time. Am a big supporter of TIDE, to support family carers (like I was of the previous Dementia Action Alliance Carers Call to Action). Had a lovely chat too with Louise Langham who is the best too. Anna Gaughan, Jean Tottie and Pat Broster were of course supporting on Twitter. Good luck to the book some of them are involved with on life story – I am sure this will be an unique high quality contribution next book to be published by my own publishers of “Living better with dementia”, Jessica Kingsley Publishers.
This meeting was not as good as a conference it was much better. There was a completely flattened hierarchy – that means people who weren’t catalysts or officers in change. People addressed people as people. Simples.
There was mutual respect for other people’s background and experiences, diverse and substantial. People with dementia and closest were pivotal in the table-top activities in co-producing dementia care pathways.
Isabel and John were amazing in their graphic and technical support for their event.
The token slot for the person with dementia or carer was discarded (which often makes the situation of engagement and empowerment worse in fact.) There was no shitty question answer session where the ‘selected few’ asked their questions. No – we all had a chance to contribute.
5o% of the places of this meet up were free of charge. All people with dementia and carers were offered a chance to attend for free.
And we got a lot done.
See – it is possible!
Loved Llandudno and North Wales in general.
Well done to “Framela”, Chris and Jayne (see a previous blogpost for the full programme).
The main rule of the game is simple. No main political party in the UK will wish to enter a general election stating an intention to privatise the NHS. Jeremy Hunt has even laughed away on many occasions the notion the NHS is being privatised, despite overwhelming evidence to the contrary.
The tragedy about the fact that some doctors want to go to Australia is that this possibly will help the vision of the NHS to be dragged out of the public sector kicking and screaming.
Love him or loathe him, Jeremy Hunt is in a long line of Secretaries of State for health who has seen (and, indeed, exacerebrated) the unwinding of the National Health Service from proper funding by general taxation in the public sector to private sector beneficiaries. This process is otherwise known as privatisation.
In as much as there are a number of ways to skin a cat (and of course I should never wish to do due to my love of cats), there are a number of ways to shoo-in the private sector into the running of the NHS.
One might be to have the private sector involved in aspects of procurement. The defence of the privatisation of NHS Logistics by a previous Labour government was magnificently tried by Andy Burnham in front of Iain Dale in one of the LBC election debates. Indeed, that news was at the time, 2006, reported as “Privatisation sparks biggest NHS strike in nearly 20 years”.
Other ways include the private finance initiative, originally worked up under the John Major government at about 1993 but fully torpedoed by the Tony Blair government following his election thereafter. The NHS Trusts saddled with colossal debt are a testament to this legacy, ably continued by subsequent governments.
In ‘balancing the books’, in what is referred to erroneously as ‘lack of sustainability’ (meaning in fact the Government no longer prioritises a well funded NHS and social care), corporate-sympathetic think tanks have largely pointed at the need to cut staff costs to solve the ‘productivity challenge’. The alternative, of course, would be to do something altogether more fundamental: that is, value and invest in staff, and renegotiate the crippling PFI loans. The NHS cannot burn off all bridges of sources of capital for the future.
‘Privatising’ the NHS is unlikely to be achieved in a ‘Tell Sid’ type flotation (initial public offering) in the City. There are no adverts on the telly for you to buy shares in the NHS. Jeremy Hunt and his minions are well aware of that.
But transferring entities within the NHS comes with its own legal considerations, such as ensuring the employment conditions of outsourced employees do not suffer. TUPE (2006) is the Act of parliament which is supposed to take care of that, harmonised through the corresponding EU directive.
I wouldn’t be at all surprised if Jeremy Hunt simply wants to tear up the current contract, and build from scratch his “privatisation-friendly contract”. NHS employees will want to protect their pensions, derogatively called ‘gold plated pensions’ by others. Current legislation will protect the pension rights of current employees being outsourced to the private sector, but it is possible HM Treasury will want to reduce this pension load by a legal carve out in a new NHS contract.
In other words, even though it would be vehemently opposed by the BMA and Royal Colleges, Jeremy Hunt could somehow impose a brand new contract by effectively making the entire workforce redundant and getting the workforce to apply for new jobs. This would be politically dynamite, as the recent solidarity of the BMA poll confirms, but technically possible if (a) Jeremy Hunt really does not care about his or his government’s popularity (in the face of a possibly weak Corbyn-led opposition), (b) Jeremy Hunt gets ‘reshuffled’ sideways onto something different (no SoS health has ever gone to lead his or her political party, to my knowledge) (c) parliament votes through the legislation for brand new NHS contracts.
Despite all the noise from Baroness Williams recently, the Liberal Democrats were instrumental in voting through the disaster-laden Health and Social Care Bill/Act. A possible and likely interpretation of this is that introducing competition promoted privatised markets consistent with a neoliberal interpretation of the doctrine of free movement of capital.
As a Doctor, I have complete solidarity with my colleagues in the medical profession, but I feel instinctively the contract is a bit of a decoy for a much wider agenda. Nothing would make me happier than to be proved wrong, of course.
Redistributing the flour into a few number of bags for less money is #notsafenotfair. The clinical regulator should have this as their prime concern.
Next week promises to be an outstanding conference on contemporary issues in dementia care.
This will be a two day programme (24-25 November) of activity, speakers, spaces and opportunities ‘to bring real, rapid change and improve dementia care and support in North Wales, and to create more informed, inclusive communities.’
It’ll take place in Llandudno, Wales, in a beautiful venue by the seaside.
I am looking forward to it hugely.
Persons who’ve received a diagnosis of dementia are at the heart of the event’s organisation, including Chris Roberts, Wales ambassador for the Alzheimer’s Society, George Rook and Agnes Houston MBE, Scottish Dementia Working Group.
Here’s the ‘Eventbrite’ page, but please do email the organisers in advance as there will be a high proportion of tickets for interested citizens.
It is a spectacular programme, not least because Jeremy Hughes CEO of the Alzheimer’s Society will be speaking. Given how busy Jeremy is, this is wonderful.
The programmes is as follows.
DAY 1: 24 November 2015
9.30am Refreshments, exhibition viewing, quiet space time, Dewis
10.00am Welcome, Chris, Jayne & Kate Roberts ‘Creating inclusive communities,
a place for everyone – what matters to us’.
Kate Swaffer will also join us via webcast from Australia.
10.30am Jeremy Hughes, CEO, Alzheimers Society UK ‘Dementia Friends’
10.45am ‘Using what we have’ asset-mapping dementia care & support in N Wales
Group discussion activity 1
11.50am ‘Dementia care pathway – Identifying issues & gaps’ Group discussion activity 2
12.35am Prof. Bob Woods, Bangor University ‘Arts and Dementia’
1.50pm Agnes Houston, Dementia and Sensory Loss
2.05pm George Rook, patient activist ‘In an Ideal World’
2.20pm First participant choice session: a choice of themed workshops,
informal hosted table conversations, quiet space, exhibition, Dewis
• Young carers • Being a dementia champion/voice • Dementia choirs
• Dementia and the natural environment • Dementia + transgender
• Dementia faith /ethnicity • Dementia and memory tasks/music
• Dementia + sensory loss • Late diagnosis •
Dementia and care homes • And more…
3.40pm Second participant choice session
4.45pm Chris, Jayne & Kate Looking forwards together
DAY 2: 25 November 2015
9.30am Refreshments, exhibition viewing, quiet space time, DEWIS
10.00am Welcome – Chris and Jayne Roberts ‘Creating change together’
10.15am Keynote speaker and Multi-sector panel presentation
The current North Wales dementia care landscape
10.30am Reviewing the asset-map of dementia care and support in N Wales
– developing recommendations for action, group activity.
11.40am ‘A dementia care pathway – Identifying issues and gaps’
Data review & creating recommendations for action group activity.
1.00pm Event close – Chris & Jayne Roberts ‘Looking forwards together’
I am staying at the conference venue itself, St George’s Hotel. I have already got an extremely good impression of them from speaking to them on the phone to organise my stay.
The ‘curate’s egg’ first appeared as a cartoon in an edition of Punch in November 1895. It refers to somebody being served an egg with some poor but some excellent parts.
The term ‘curate’s egg’ was famously described in relation to the Health and Social Care Bill as it negotiated the machinery of parliamentary procedure by Hamish Meldrum of the British Medical Association.
Invariably, people given a diagnosis of dementia react in a number of different ways to the news. Much of it depends on their pre-conception of what dementia is, but some of it arises from the way in which the details of a possible diagnosis of dementia are disclosed.
I have found people’s knowledge of dementia very variable. In the main, though, I find that most people’s views of dementia are derived from close family members. No one person with dementia is the same, and your perception of that one person might well be different to someone else’s perception.
The reasonable expectation is that, if someone were to tell you that he or she has been diagnosed with dementia, this might be reciprocated with some understanding of what dementia is.
People are also different in the way they wish to express their views about dementia. No one person is the same. That’s why there’s no such thing as a ‘best campaigner’ for dementia.
Here Tommy Dunne explains why he likes Twitter but not Facebook:
I have concerns about the prevention arm of policy. I do not dispute the value in people leading lifestyles to minimise the risk of developing the clinical symptoms and signs of dementia, or to minimise the risk of fast progression of dementia.
But we have to be prepared to concede that there are people around who can’t tick off many of the risk factors for themselves. Iris Murdoch who was highly educated developed dementia: thus disputing the adage, “use it or lose it”.
But the issue that all individual voices offering a complementary narrative is useful.
Keith frames it as ‘going beyond telling a person’s story’, viz:
“Whilst personal stories are really useful, and make significant impressions, if a service user can go beyond that and target the audience in seeking to inspire change, then so much the better. The phrase “expert by experience”, when connected to living well with dementia, and person-centred care, can, with support, produce presentations which are harder hitting and consequently move people to change.”
These observations are all taken from “Dementia Diaries”. To read more about the project, please go here.
I was honoured to be invited by Chris Roberts and his family to the National Dementia Care Awards 2015.
Jayne Goodrick, despite the fact the family camper van broke down in full blazen glory, looked dazzling.
I arrived at the Birmingham Hilton Metropole Hotel on Friday afternoon, where I was immediately serendipitously greeted by Lucy Frost and Emma Bulled. I was very relieved to see them both as I knew as I was in the right city. I was pleased that Brighton’s initiatives in acute hospital care had been recognised, in no small part due to Emma and Lucy and their colleagues.
Lucy later that evening introduced me to her friend and colleague Richie who was great to chat with – Richie is a very gifted, thoughtful individual who also works at Brighton.
Entering the event was a bit of a ‘who’s who’.
I feel now as if I’ve got to know Dr Richard Hawkins quite well by now, having spent nearly two weeks back to back in his company (the first week being the UK Dementia Congress in Telford the other day). Richard’s great fun.
At the front of most of our thoughts was Tim Lloyd-Yeates who sadly passed away earlier this year. I really enjoyed the presentation by Alive! which was Tim’s creation.
Was really good to see Zoe Harris and Sally Knocker, longstanding Twitter pals.
It was great to see the Northern Irish contingent, Joanne Agnelli, Jessie McGreevy and Gary Mitchell.
But huge apologies for the accidental photobombing later.
I should like to thank Jessica Harman and Fiona Robb for the huge amount of work they put into the evening, and Jessica especially for getting me access to soft drinks (as I never drink alcohol for various reasons) without any fuss or reservation at all.
I have to say, entirely genuinely, the organisation was immaculate.
We rarely get a chance to celebrate the best in dementia care. Too much of it comes across as firefighting, or even at worst ‘damage limitation’. It was therefore awesome to celebrate people who are at the top of the game.
I said to Joy Watson, an amazing campaigner, and nominee for most exceptional person living with dementia, jokingly, that Tony Husband was enjoying himself at the champagne reception. Joy laughed and said, “Yeah Shibley – he’s driving!”
I think a part of dementia policy which works is ‘dementia friendly communities’. There is no doubt that Nicky Taylor and the team of West Yorkshire Playhouse were deserved winners of best innovation, for the sheer remarkable skill and attention to detail they pay over inclusivity and accessibility.
This is all a fire cry from my memory of clinical training in the cusp of the turn of the millennium where residents with dementia were literally restrained to their chairs, abusing their fundamental human rights, and had set times at which to go to the toilet.
This is not to airbrush bad care, at all, but for us to learn from what works in a constructive manner.
It was an honour to meet Liz Cunningham who won most exceptional person living with dementia, who was praised for her outstanding initiatives in the local community.
I think personally in future it might be sensible for all finalists to be ‘winners’ in this category. All the nominees, including Chris Roberts, Joy Watson, Ken Howard, I personally felt were outstanding – and whilst I am not one for ‘the Dodo verdict’, i.e. “everyone has won and all shall have prizes”, I felt to judge people who have a cigarette paper between them in terms of contribution to campaigning for awareness was unfair to all concerned.
Chris Roberts even got a card later on from the judges praising him for his outstanding work.
But this was a very very nice touch by the organisers of this event.
Meanwhile, here’s “our Ken” – I reminisced with Zoe the old joke, “What do you call a well dressed man in a suit? The defendant.”
The deadline for abstracts submission is November 16th 2015.
Here’s my sole submission for the 31st ADI conference to be held in Budapest.
Title:
The awareness of fundamental international legal human rights underpinning rights-based advocacy for dementia.
Dr Shibley Rahman
Background
An assumption invariably made is that the general public, including people living with dementia and carers, have a good understanding of the fundamental human rights which underpin policy.
To make use of the rights in rights based advocacy, you need to know what these rights are, as they are enforceable. The Mental Health Foundation published in 2015 their much awaited and influential report ‘Dementia, rights and the social model of disability’.
Most significantly, the European Convention for Human Rights (ECHR) and the UN Convention for Rights for People with Disabilities (UNCRPD) apply in Europe and the world respectively.
Dementia is a disability under international law.
Objectives
There are relatively few studies of the level of awareness of international rights.
This study aimed to remedy that.
Methods
A ‘Survey Monkey’ survey took place in the first week of November 2015. Invitations to participate were tweeted regularly. There was no restriction geographically on participation.
Results
The electronic questionnaire contained 11 questions.
A maximum of 54, and minimum of 51, responses were elicited for any one question.
19% stated that they were disabled.
The vast majority (83%) perceived dementia to be a disability (answering 4 or 5 on a scale of 0 (not at all) to 5 (very much)).
A substantial proportion of respondents did not know whether right to a personal budget (47%) or a right to a medical diagnosis (39%) were rights under ECHR.
A high proportion (81%) recognised the right to privacy and family life as a human right under ECHR.
Of four instruments surveyed (human rights act, mental capacity act, UNCRPD and equality act), the respondents felt that all four instruments had approximately equal ‘importance’.
A sizeable proportion did not know the availability of the two separate rights to accessibility or to justice under the UNCRPD (54%, 54%).
48% did not know that a right to live independently and in the community exists under the UKCRPD.
47% did not know that a right to work and employment exists under the UNCRPD.
Of the five PANEL principles (participation, accountability, non-discrimination and equality, empowerment and legality of rights), non-discrimination and equality was viewed as the most important (34%); and accountability the least (4%).
Conclusions
The significance, conceding limitations, of these results for international policy will be discussed fully.
We’ve all done it: preaching to the choir, or pushing on an open door.
Turn back the clock, and you can listen to a recording of a radio programme where Reginald Maudling, Enoch Powell, Michael Foot and Roy Jenkins profoundly disagree on policy.
The timeline is this. It is perceived that the next step of defining the English dementia strategy will be the ‘implementation plan’ for Dementia 2020.
I am told we can probably expect this plan to surface around January 2016.
Indeed, clinical specialist nurses are mentioned on page 27 in the section on support after diagnosis. This is where my original discussion had in fact started, on a recent blogpost on the need to define what exactly we mean by ‘post diagnostic support’ [blogpost here].
I was advised recently that NICE guidelines are of limited value, as CCGs are free to ignore NICE guidelines and other evidence bases for dementia. There is no obligation for CCGs to contain any expertise in dementia, including from dementia specialists including people living with dementia. CCGs are statutory insurance bodies; it is good marketing, however, if GPs happen to be amongst the personnel of CCGs, it’s a “win win”.
I have been to meetings of policy where very senior people, who should remain nameless, say that there’s no point having a plethora of good clinical outcomes unless there is a clear business model for a “cost saving”.
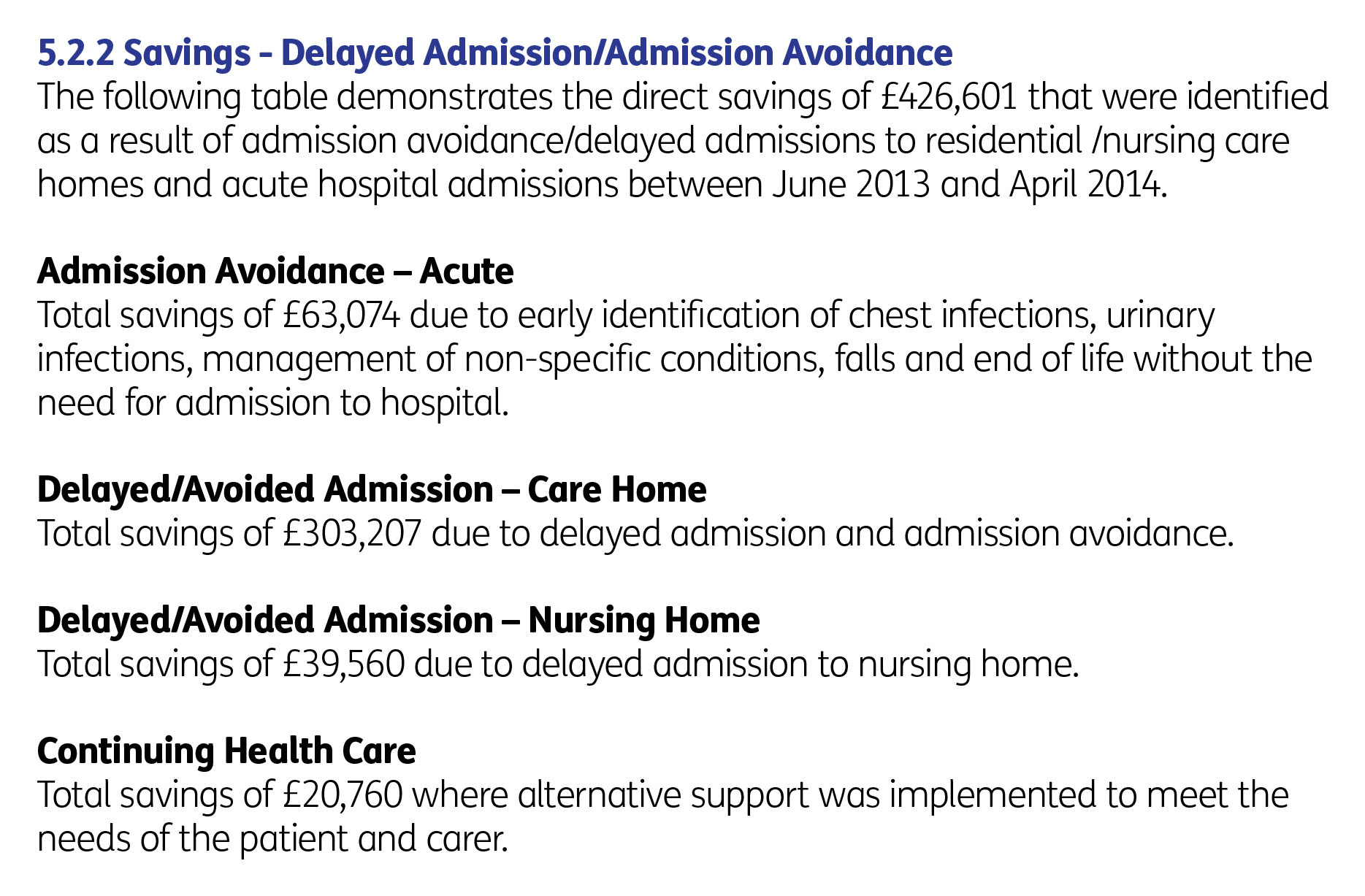
As it happens, numerous reports have emphasised the financial advantage of the Admiral nursing approach. The evaluation of the Norfolk Admiral Nurses programme showed a banquet of cost savings, including on avoidable admissions (p. 31).
Yes indeed as Beth Britton identifies here the central issue is ‘facing dementia and getting support’.
Some of the reasoning is as follows.
The person with dementia must be seen as a unit, with a key friend or member(s) of family. This is the case from the very time the person is given a diagnosis.
The Admiral nurse can advise this unit on the symptoms as they arise.
The Admiral nurse network works in a variety of care settings, e.g. at home, in a residential setting, a hospital; this helps to ensure continuity of care.
The Admiral nurse can, later on, guide the unit through palliative care issues.
The Admiral nurse can make specialist referrals, such as if the medication needs adjustment, or some input is needed on a key aspect of ‘life planning’ (e.g. wills, power of attorney).
Two pivotal events might occur at some stage, for which an Admiral nurse can offer expertise: one when the person with dementia loses the legal ability to make decisions (‘capacity’), or when a person with dementia might choose to go into a residential setting – care home or nursing home.
Caring for people with dementia, as included in marriage vows as well, can be incredibly rewarding. However, caring is the equivalent of a full time job and the system is only kept afloat due to the millions of hours put in per year from unpaid carers (as well as carers, often made, on zero hour contracts and barely meeting the requirements for the national minimum wage). All of this is clinically significant as the wellbeing of the person with dementia is intimately related to the wellbeing of a carer (or ‘BUB’ as per Kate Swaffer‘s nomenclature).
The Admiral nurse can educate the unit, and other professionals, on what dementia is, and how a person with dementia can be best supported to live after the diagnosis.
I am sick of calling for a national dialogue, as national policy after national policy fails to make the argument for good clinical practice.
To be frank, I have become bored of looking for people to blame – apart from the fact that I feel that ‘clinical leaders’ in dementia have failed to lead on this crucial area of policy. I think dementia advisers and dementia support workers are wonderful, but you have to worry as they become overwhelmed in their rôle of signposting to ever dwindling services.
Some players in dementia are too tribal, actually putting their ‘tribal-ity’ ahead of the clinical needs of persons with dementia and carers. This is simply wrong.
I truly want all of this to be ‘in it together’. This means that we work and live together, all, for the benefit of people with dementia and carers. Due to stubborn political obstruction, the momentum for Admiral nurses simply is not there – compared to, for example, Marie Curie and Macmillan nurses – and the resources reflect this.
I sometimes think policy debate is somewhat contrived, and theatrical with everybody playing their expected part. I liken this orchestration to ‘The Truman Show‘.
Well, I have no wish to be a silent bystander to this grave error in policy, from the perspective of two professions. I think this political obstruction is getting in the way of fulfilment of s.1(1) Care Act – the promotion of wellbeing.
But I do think you do need to have discussions with people you profoundly disagree. For example, you might wish to have a discussion with Vladimir Putin over investment in our infrastructure, even if you disagree much with Russia’s human rights record.
Same for Modi.
Same for me and the people in charge of dementia policy.
The late Enoch Powell advises in this radio programme, above, that, only if you understand your opponent’s arguments properly can you understand why you are RIGHT and they are WRONG.
My summary. I think all persons living with dementia, and carers, deserve better.