The HE KSS/BSMS (Health Education Kent Surrey and Sussex / Brighton and Sussex Medical School) have launched the “Primary Care Dementia Fellowship Programme”.
This is a programme for GPs, practice nurses and staff, and community nurses in Kent, Surrey and Sussex.
(Health Education Kent Surrey and Sussex will provide the funding to release Fellows to attend a regional skills development programme that will run from March to September 2014.
The Fellows will join with doctors and nurses from Kent, Surrey and Sussex (KSS) to build the knowledge and skills needed for them to create better dementia services in KSS.
Prof Sube Banerjee and Breda Flaherty of Brighton and Sussex Medical School (BSMS) are leading this initiative based on their successful experience in the NHS London Deanery.
It appears that the main aim is to build a network of Fellows who can act as ‘change catalysts’ (my words not theirs), to spread best contemporaneous practice in dementia care.
It’s important as dementia is one of the top five strategic priorities in the KSS Skills Development Strategy.
Modules will be led by Banerjee and Flaherty, with contributions from clinical experts in dementia; colleagues in social care; people in the care home sector; NGOs; persons living with dementia and carers; specialists in service development; commissioners and researchers.
I believe that such a course will have considerable competitive advantage in being totally disruptive in how traditional training for juniors in dementia is conducted.
The value is clearly in the collaborative ties between members of the network. By lowering the cultural barriers in this way, the team at Sussex have something very special here.
The set-up is perfect for boundary-less knowledge sharing, and this is enormously value as we all get to grips with what the priorities in local and national policy in dementia might be.
There are three modules running from March to June: good practice in dementia assessment and care, good practice in dementia, and changing practice.
These are followed by a ‘Next Steps’ conference and a period of evaluation and research.
Such an approach might become paradigmatic for future learning in the NHS in dementia.
Unknown to me, the title of Prof Banerjee’s talk is an allusion to this famous track from 1979 (when I was five). It’s “Reasons to be cheerful (part 3)” by Ian Drury and the Blockheads.
The Inaugural Lecture – Professor Sube Banerjee (“Professor of Dementia”), ‘Dementia: Reasons to be cheerful’ was held on 26 February, 2014, 6:30 pm – 8:30 pm, at Chowen Lecture Theatre, Brighton and Sussex Medical School, Sussex Campus. BN1 9PX. Details are here on the BSMS website.
I found Prof Banerjee to be a very engaging, ‘natural’ speaker.
I arrived with hours to spare, like how the late Baroness Thatcher was alleged to have done in turning up for funerals.
Brighton are very lucky to have him.
But his lecture was stellar – very humble, yet given with huge gravitas. Banerjee is one of the best lecturers of any academic rank in dementia I have ever seen in person.
Banerjee started off with a suitable ‘icebreaker’ joke – but the audience wasn’t at all nervous, as they all immediately warmed to him very much.
He is ‘quite a catch’. He is able to explain the complicated issues about English dementia policy in a way that is both accurate and engaging. Also, I have every confidence in his ability to attract further research funding for his various teaching and clinical initiatives in dementia for the future.
Most of all, I was particularly pleased as the narrative which he gave of English dementia policy, with regards to wellbeing, was not only accurate, but also achievable yet ambitious.
Banerjee argued that the 1970s which had only given fruit to 209 papers, but things had improved ever since then.
It was the year of course Margaret Thatcher came to power on behalf of the Conservative Party.
In contrast, there have already been thousands of papers in the 2000s so far.
Banerjee also argued that “what we know is more likely to be true” which is possibly also true. However, I immediately reminisced of the famous paper in Science in 1982, “The cholinergic hypothesis of geriatric memory dysfunction”. This paper, many feel, lay the groundwork for the development of cholinesterase inhibitors such as donepezil (“Aricept”, fewer than twenty years later.
It is definitely true that ‘we are better at delineating the different forms of dementia’.
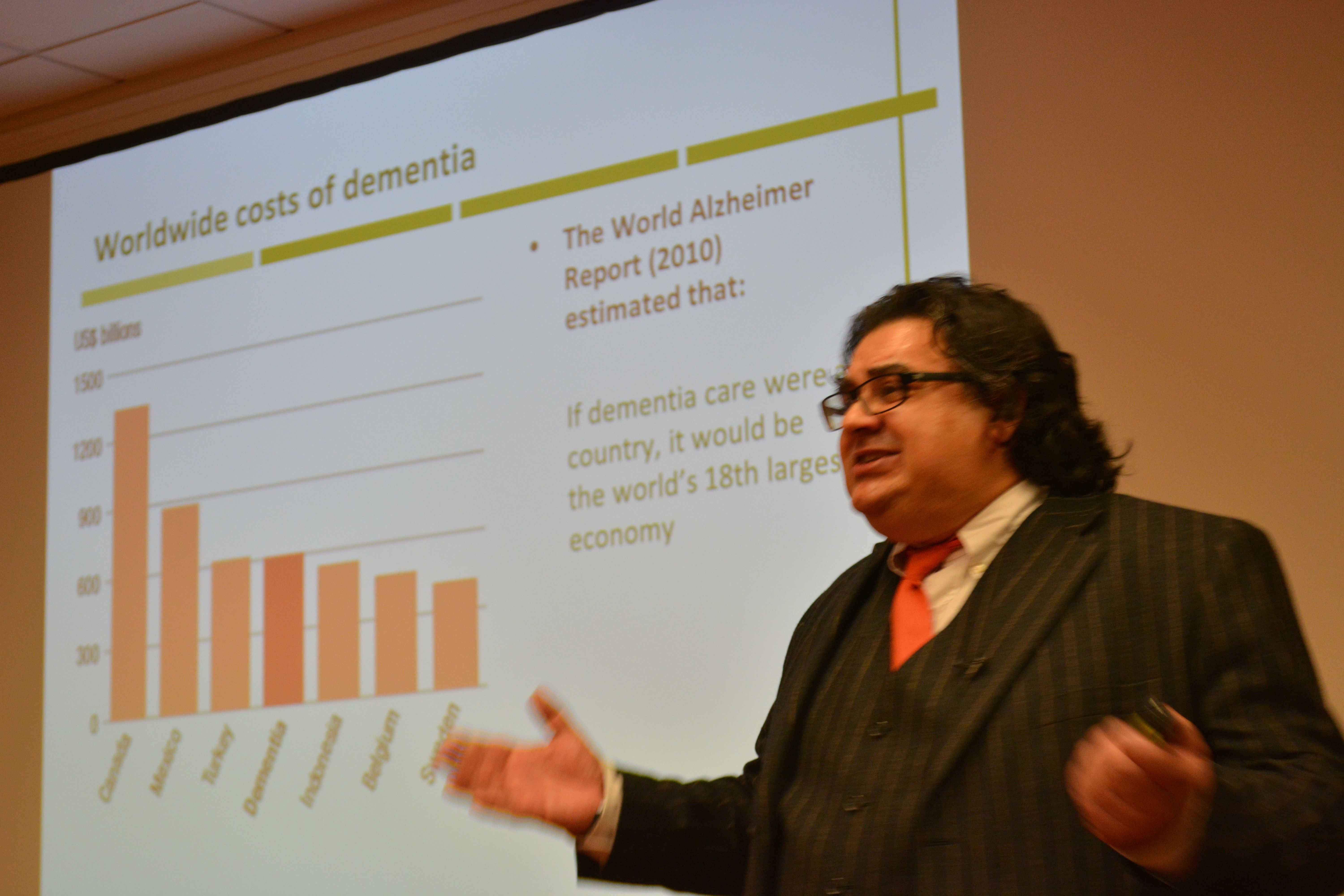
I prefer to talk of the value of people with dementia, but Banerjee presented the usual patter about the economic costs of dementia. Such stats almost invariably make it onto formal grant applications to do with dementia, to set the scene of this particular societal challenge.
I am of course a strong believer in this as my own PhD was in a new way to diagnose the behavioural variant of frontotemporal dementia. In this dementia, affecting mainly people in their 50s at onset, the behavioural and personality change noticed by friends and carers is quite marked. This is in contrast to a relative lack of memory of problems.
Not all dementias present with memory problems, and not all memory problems have a dementia as a root cause. I do happen to believe that this is still a major faultline in English dementia policy, which has repercussions of course for campaigns about ‘dementia awareness’.
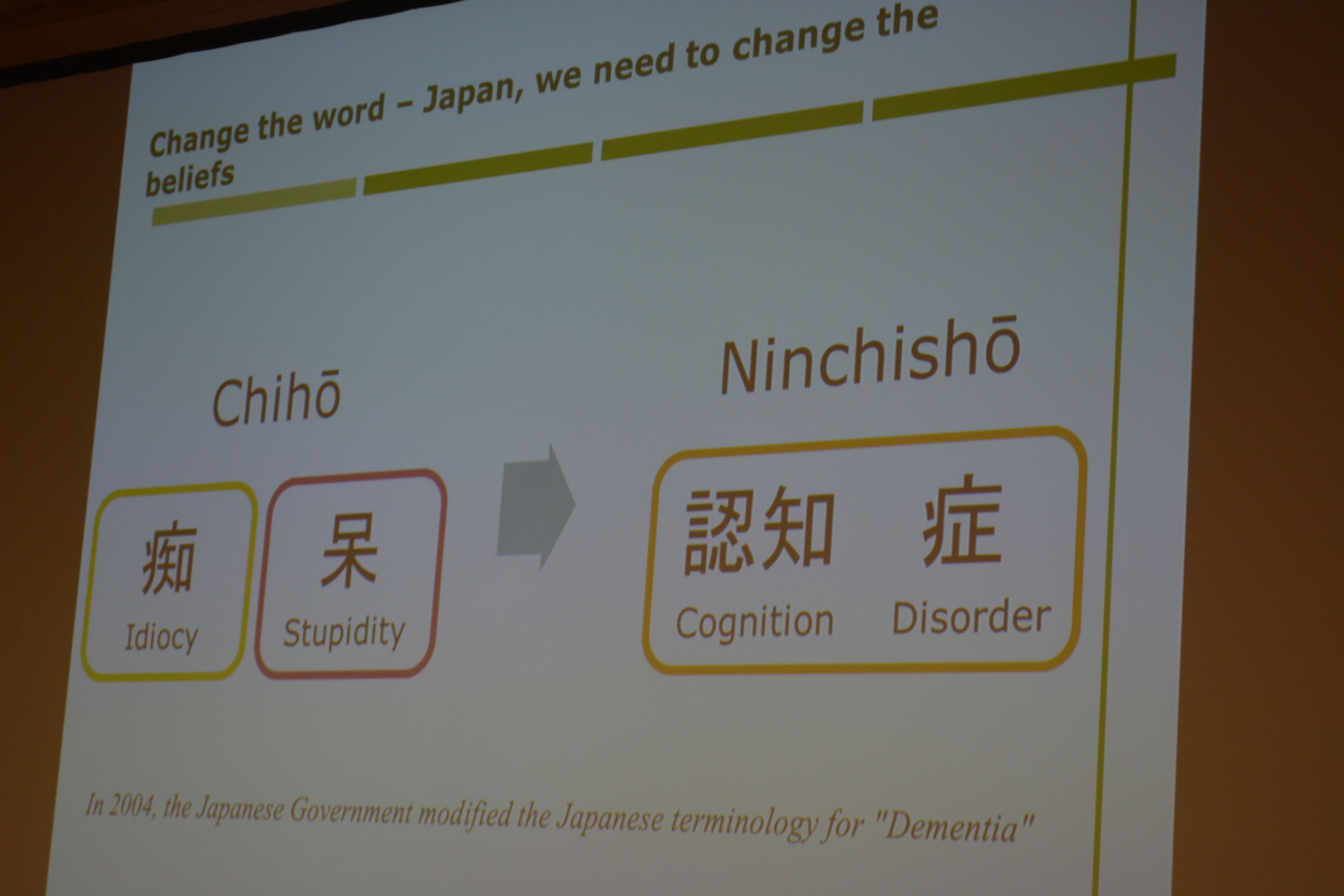
A major drive in the national campaigns for England is targeted at destigmating persons with dementia, so that they are not subject to discrimination or prejudice.
The dementia friendship programmes have been particularly successful, and Banerjee correctly explained the global nature of the history of this initiative drive (from its “befriending” routes in Japan). Banerjee also gave an excellent example to do with language of dementia friendship in the elderly, which I had completely missed.
Raising awareness of memory problems in dementia is though phenomenally important, as Alzheimer’s disease is currently thought to be the most prevalent form of dementia worldwide.
The prevalence of dementia may even have been falling in England in the last few decades to the success prevention of cardiovascular disease in primary care.
The interesting epidemiological question is whether this should have happened anyway. Anyway, it is certainly good news for the vascular dementias potentially.
That dementia is more than simply a global public health matter is self-evident.
I’m extremely happy Banerjee made reference to a document WHO/Alzheimers Disease International have given me permission to quote in my own book.
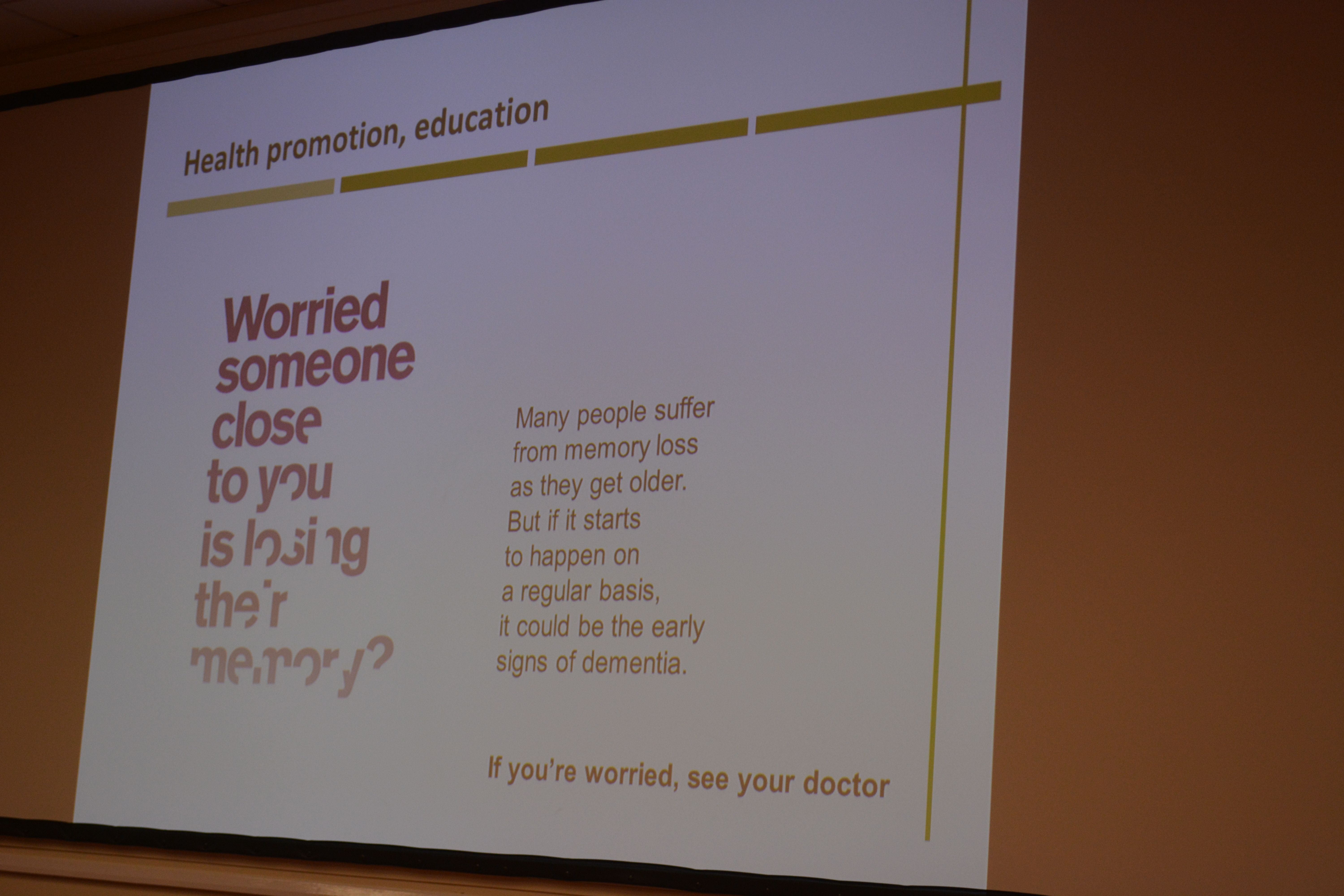
Banerjee presented a slide on the phenomenally successful public awareness campaign about memory.
In developing his narrative about ‘living well with dementia’, Banerjee acknowledged at the outset that the person is what matters at dementia. He specifically said it’s about what a person can do rather than what he cannot do, which is in keeping to my entire philosophy about living well with dementia.
And how do we know if what we’re doing is of any help? Banerjee has been instrumental in producing, with his research teams, acceptable and validated methods for measuring quality of life in dementia.
Banerjee of course did refer to “the usual suspects” – i.e. things you would have expected him to have spoken about, such as the National Dementia Strategy (2009) which he was instrumental in designing at the time: this strategy was called “Living well with dementia”.
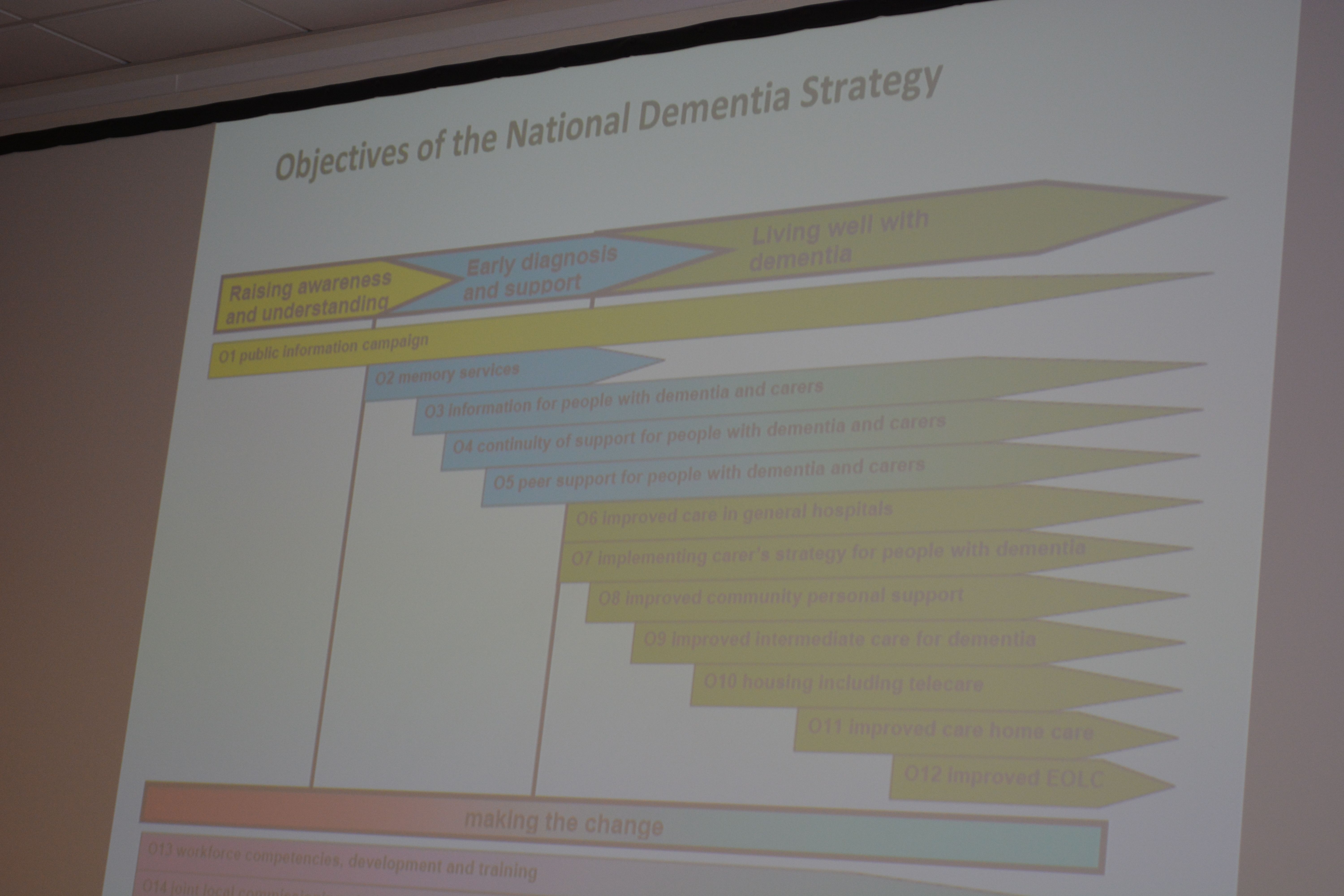
“I’m showing you this slide BECAUSE I want YOU to realise it IS complicated”, mused Banerjee at the objectives of the current English dementia policy.
I asked Banerjee what he felt the appropriate ‘ingredients’ of the new strategy for dementia might be – how he would reconcile the balance between ‘cure’ and ‘care’ – “and of course, the answer is both”, he said to me wryly.
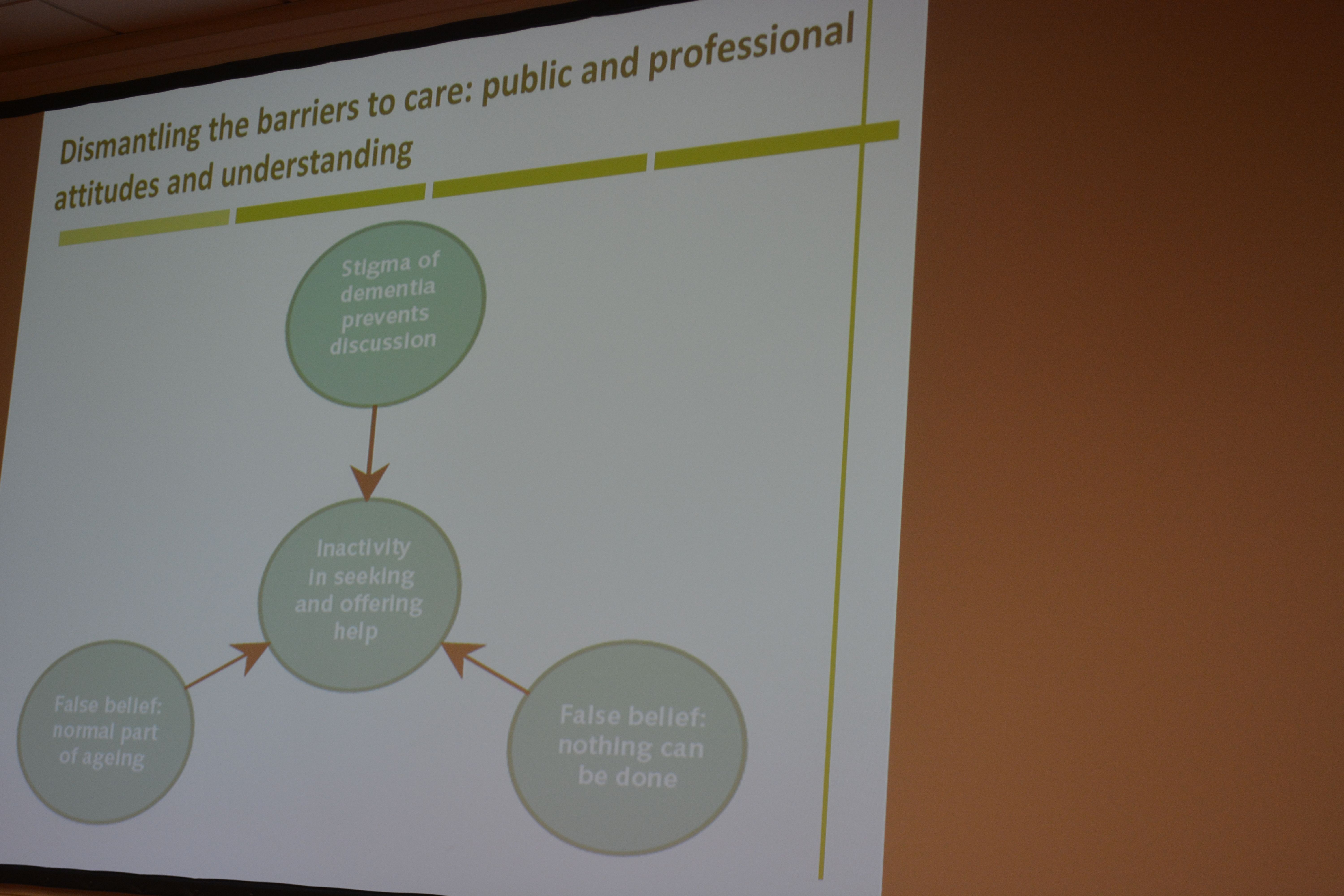
Banerjee acknowledged, which I was massively pleased about, the current ‘barriers to care’ in this jurisdiction (including the known issues about the “timely diagnosis of dementia”.
Clearly the provision at the acute end of dementia care is going to have to come under greater scrutiny.
I increasingly have felt distinctly underwhelmed by the “medical model”, and in particular the repercussions of this medicalisation of dementia as to how grassroots supporters attempt to raise monies for dementia.
I am of course very proud that Prof Alistair Burns is currently reading my book focused on the interaction between the person and the environment in dementia.
And of course I’m ecstatic that Lisa Rodrigues and Prof Sube Banerjee signed my book : a real honour for me.
I signed Lisa’s book which was most likely not as exciting for her! X
At the outset, I would like to say that I am not aware of anyone selling courses on dementia friendship.
But it would perfectly feasible to set up a course with some sort of kite mark or quality standard, where you reach an objective level in dementia awareness, and to sell you a qualification in it.
There’s nothing, arguably, particularly immoral in it in that it’s selling education, such as for plumbing or complicated neurosurgery.
It is indeed a worthy cause – raising dementia awareness.
However, policy in England has recently seen a drive towards commodification of public services.
A number of entities are also working in increasingly corporate ways, in their access to finance, marketing, operations management and strategy.
However, policy in England has recently seen a drive towards commodification of public services.
Various organisations are also working in increasingly corporate ways, in their access to finance, marketing, operations management and strategy.
So there’s nothing to stop people ‘selling’ how to do dementia friendship. Even though it’s hard to value dementia friendship, it would be pretty easy to cost it.
People have found increasingly innovation-worthy ways of selling water.
Dementia friendship is a wide-ranging policy across a number of jurisdictions. Many people have befriending an individual with dementia without making a song or dance of it.
However, unfortunately, dementia friendship is open to commercial abuse.
It reminds me of the law on foraging – as such picking berries on farms is not against the law, but selling them by the bucketload for commercial gain is in fact a theft offence potentially under the Theft Act (1968).
“Mother Nature’s Son” was an episode of “Only Fools and Horses”, first transmitted on Christmas Day 1992.
Rodney is concerned that Del has lost his drive. When confronted, Derek explains that on top of his woes, the council have approved his application to buy their flat in Nelson Mendela House, doubling the rent. On top of that, Grandad’s allotment has become a health hazard and he has to clear it.
Finally spotting a gap in the market, Del decides to bottle tap water and sell it as Peckham Spring Water.
It is a legally interesting question as to whether you could rebottle tap water, which you’ve paid for, and sell it under your own branding.
Yes – it’s all about rent-seeking as usual; this is defined as is spending wealth on political lobbying to increase one’s share of existing wealth without creating wealth. The effects of rent-seeking are reduced economic efficiency through poor allocation of resources, reduced wealth creation, lost government revenue, national decline, and income inequality.
A ‘Big Mango’ has just gone missing, but will people notice if Big Data suddenly goes missing for the purposes of research into dementia?
A large ceramic mango is of course tangible property, whereas the information itself of ‘Big Data’ isn’t. But the recent furore over ‘caredata’ has illustrated how meticulously careful if you have to be about consent.
Twitter is amazing.
During infectious disease outbreaks, data collected through health institutions and official reporting structures may not be available for weeks, hindering early epidemiologic assessment.
In contrast, data from informal media are typically available in near real-time and could provide earlier estimates of epidemic dynamics. Many people for ‘breaking news’ nowadays prefer to do a Twitter search than wait for a news bulletin.
Rumi Chanara and colleagues (Chanara et al., 2012) assessed correlation of volume of cholera-related HealthMap news media reports, Twitter postings, and government cholera cases reported in the first 100 days of the 2010 Haitian cholera outbreak.
Trends in volume of informal sources significantly correlated in time with official case data and was available up to 2 weeks earlier. They found that informal data can be used complementarily with official data in an outbreak setting to get timely estimates of disease dynamics.
The English law does pride itself, however, on some sort of law on the protection of information (hence the enactment of the Data Protection Act 1998).
Long before that, Oxford v Moss (1979) 68 Cr App Rep 183 was an English criminal law case, dealing with theft, intangible property and information. The court ruled that information could not be deemed to be intangible property and therefore was incapable of being stolen within the Theft Act 1968.
The defendant, Moss, was a University student and managed to obtain a proof copy of his forthcoming exam paper. It was accepted that he always intended to return the proof itself, and therefore could not be convicted of theft of the proof itself, however he was charged with stealing information belonging to the Senate of the University.
How confidential medical data are dealt with has been cause for a broohaha recently.
Informed consent is an ‘opt-in‘ model:people have to sign up to donate organs. In this model, donors must also be made aware of what they are signing up for and have the option of withdrawing their consent at any point.
Informed consent contrasts with presumed consent (used in association with organ donation, the assumption that an individual is happy to donate organs after death unless he or she has explicitly said that they do not wish to).
At the beginning of February 2014, it was reported that the Information Commissioner’s Office had been concerned that the information provided to patients on care.data is not clear enough about how to opt out of the programme.
According to Prof Brian Jarman, an expert statistician whose interests data and public health, the arrangements concerning ‘caredata’ do not sound like informed consent.
“The Data Protection Act (DPA) usually requires organisations by default to offer opt-in. Yet for the confidential care.data opt-out is the only option. This suggests a lack of informed consent. The leaflet sent to people in their junk mail gives little information about the drawbacks. To have informed consent patients need to be told of the risks as well as the benefits.”
This was a bit of a public grab, but possibly competing in publicity with the latest finding that thieves have just made off with a 10 metre high, 10 tonne mango replica from a town in northern Queensland, Australia.
A crane was used to rip the three-storey giant fruit from the concrete platform on which it had stood since 2002.
Just as people are now vigilant about the theft of giant mangos, the theft of Big Data has come under justifiable scrutiny.
Already there has been the massive plastic card data theft in South Korea, affecting about 60 million cards; the Target Corp. credit card disaster involving up to 40 million customers; the hacking of 16 million German e-mail accounts; data securitybreaches at Nieman Marcus Inc. and Easton-Bell Sports Inc.; and a group of Russian hackers who compromised the computer systems of Western energy and defense companies, governments, and academic institutions.
Cybercriminals, of course, abuse less obvious vulnerabilities, such as those in site-building software. In these cases, they often buy malware rather than develop it themselves.A specialised field, the grab of Big Data has particular relevance to people worried about hackers of a giant database of NHS clinical data.
So are Big Data important? An article in Wired Magazine “The End of Theory: The Data Deluge Makes the Scientific Method Obsolete ” cited provocatively that, “All models are wrong, but some are useful.”
So proclaimed statistician George Box 30 years ag.
In this article, it was stated that the scientific method is built around testable hypotheses but some of the models have not actually been that good, in comparison with real data.
Mendel and Newton are cited.
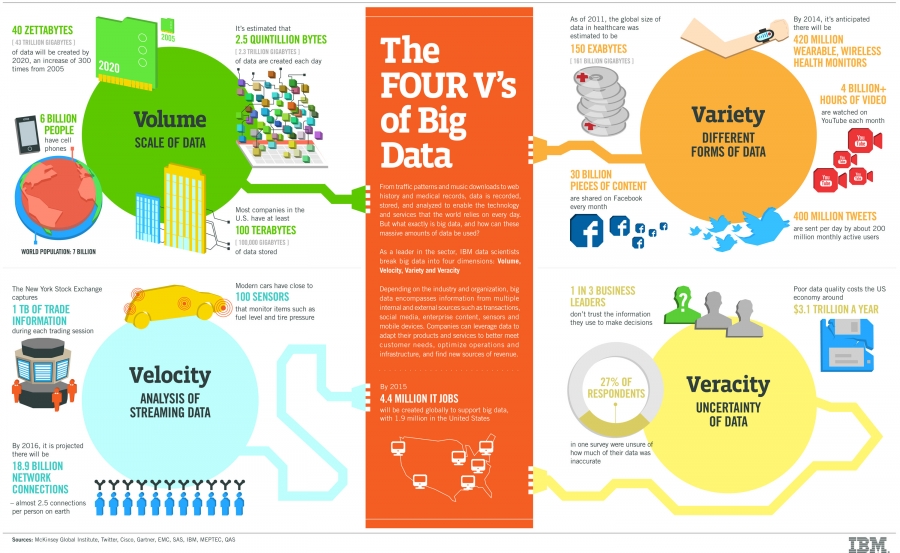
According to McKinseys, the amount of data in our world has been exploding, and analyzing large data sets—so-called big data—”will become a key basis of competition, underpinning new waves of productivity growth, innovation, and consumer surplus”.
In October 2012, it was reported that Massachusetts General Hospital would receive $5.4 million from the nonprofit Cure Alzheimer’s Fund, in what the fund said was the largest single private scientific grant ever invested in Alzheimer’s whole-genomesequencing.
The Alzheimer’s Genome Project would obtain complete genomic sequences of more than 1,500 patients in families that have Alzheimer’s, and will include over 100 brain samples. The genomes of family members with Alzheimer’s will be compared to those members who have been spared the disease to identify sites in the genome that influence risk for Alzheimer’s.
And it does seem as if people are generally moving with the times,.
In January 2014, for the “Nuffield Council on Bioethics: The linking and use of biological and health data” a response by the Wellcome Trust from January 2014 provided a number of interesting points.
“The linking and use of biological and health data is central to a wide range of biomedical research. There is a strong need to ensure a legal and regulatory environment in which these data can be used and linked for the purposes of research that aims towards improving health.”
However, the following was also noted.
“There are legitimate ethical concerns about the privacy implications of the use and linking of such data and future developments in using these data cannot necessarily be anticipated. Participants’ wishes are paramount, and there is a need for strong governance mechanisms for the use of participant data in research that can appropriately protect participant confidentiality.”
“Now, with a few years of experience, we’ve observed that Google Health is not having the broad impact that we hoped it would. There has been adoption among certain groups of users like tech-savvy patients and their caregivers, and more recently fitness and wellness enthusiasts. But we haven’t found a way to translate that limited usage into widespread adoption in the daily health routines of millions of people.”
Of course the grab of a giant mango can only put down to a publicity stunt; sharing of data for the public good in no way constitutes theft if done with the informed consent of people involved, although regulators have ingenious ways of making certain things permissible as they wish.
Stealing a giant mango is hardly likely to be legislated for in the near future, however.
As of 2013, there were an estimated 44.4 million people with dementia worldwide.
This number will increase to an estimated 75.6 million in 2030, and 135.5 million in 2050. There are currently 800,000 people with dementia in the UK. There are over 17,000 younger people with dementia in the UK. There are over 25,000 people with dementia from black and minority ethnic groups in the UK. It is thought that there will be over a million people with dementia by 2021.
People are living longer. While this is good news, an ageing population also presents a number of serious challenges for the health and social care system. Both the proportion and absolute numbers of older people are expected to grow markedly in the coming decades. The greatest growth is expected in the number of people aged 85 or older – the most intensive users of health and social care.
It’s likely that we will be able to test for genetic risk factors for the dementias with much greater certainty in the decades ahead, due to advances in technology. This will be, most likely, a particularly powerful tool in those families where dementia appears to affect a number of generations.
Alzheimer’s disease is the most common form of dementia and, of all the main types of dementia, the genetics of Alzheimer’s is the best understood.
We can currently, perhaps, consider the disease to have two forms: the rare early onset Alzheimer’s disease, where first symptoms appear before the age of 65; and the much more common late onset Alzheimer’s disease, where typically the first symptoms develop after this age. These two types of Alzheimer’s disease generally have different patterns of genetic inheritance.
Vascular dementia is the second most common form of dementia. There are no established direct genetic causes for the more common forms of vascular dementia, but researchers are looking for risk genes for the disease. The most recent findings suggest that APOE ε4 is a risk factor for vascular dementia, but with weaker effects than for Alzheimer’s disease. There are also known genes that contribute to some of the underlying risk factors for vascular dementia, such as high cholesterol levels, high blood pressure and diabetes.
Frontotemporal dementia (FTD) often runs in families: about one third of people with it have a family history. In 10–15 per cent of all people, FTD is inherited as a mutation in a single gene, most notably in the genes for the proteins tau and progranulin.
The architects of the NHS recognised that equity in health care could only be achieved by sharing the risks and costs of care across the whole of society from rich to poor and from healthy to sick. It is well established that poverty and ill health are closely associated. Risk sharing means that those with the highest needs must not be penalised for being both sick and poor.
It was for this reason the architects of the NHS embedded solidarity and collective provision into the structures for the funding and delivery of care. The Health and Social Care Act (2012), on the other hand, put some competition jet engines on the NHS so that it could be easily worked up as a privatised market.
In the April 2002 budget, the then Chancellor Gordon Brown had reaffirmed the UK commitment to central taxation as being the most progressive and efficient way of risk pooling in the NHS. It allowed those with the greatest health and wealth to share the benefits of their good fortune with those who are not so fortunate. Importantly, it removes the stigma of charity by making health care an entitlement to which we all contribute.
But there has a growing lobby in support of funding alternatives.
The Adam Smith Institute have in the past proposed a switch to insurance funding and along with the private sector have lobbied for private insurance. The argument is that alternatives would leave more resources for those with greatest need within the NHS or would increase efficiency. But the consequence of the alternatives is market-oriented health care – decreased access, reduced quality and increased cost.
In contrast to universal public services, which consolidate and strengthen the risk pool through integration, markets work by dividing the population into winners and losers. Genetic make-up can in the future be used to determine who the likely winners and losers might be, when it comes to the risk of developing a dementia.
Of course, dementias are governed by an interplay of genetic and environmental factors, so it’s not altogether clear-cut. But as research develops, these answers might become a lot clearer.
Profit is maximised where providers can pick the winners and reject the losers. In health this means selecting the profitable patients and the profitable services.
A possible alternative, if you’re not going to entertain the free at the point of need system, embraces ‘co-payments’ or ‘top-up payments’. In a survey reported by the Patients’ Association as “NHS Co-Payments: How popular are they among healthcare users?”, 1018 people replied.
Clear support for the principle of free at the point of use with 89.9% saying that they thought the principle of an NHS free at the point of use was a good one. However, support for the principle of ‘ free at the point of use’ falls to 69% when respondents are asked to take into consideration economic factors when considering the issue of co-payments.
Even in ‘whole person care’, if NHS and social care budgets get merged, it may not be so obvious how much the State is actually providing, particularly if the system allows the provision of ‘co-payments’. So, if the ‘universal, free at the point of need’ principle gets eroded by the introduction of co-payments, even if no political party is ultimately brave enough to go for private insurance provision, it could still be costly for an individual who develops a dementia.
To coin a phrase by Harold Macmillan, you may never have had it so good.
I don’t have particularly strong views either way about the diagnosis rates of dementia in England, other than the fact I am mindful that some people wait unacceptably for years before they are formally diagnosed.
This is a concern that some persons with dementia may not wish to have a diagnosis of dementia.
There is some evidence to support this in fact, because of the documented delay in times for people to seek medical help.
There is still unquestionably a stigma for a person receiving a diagnosis of dementia, which is a huge life-changing event for the person involved and those closest to him or her.
GPs are brilliant professionals. My late father was one for about 25 years in fact.
However, some may be mutually colluding with persons who don’t wish to receive a formal diagnosis of dementia, in that either party may prefer to attribute memory problems to ‘normal ageing’.
We do run the risk of pathologising memory problems. Already, receipt of a diagnosis of dementia takes you down a medicalisation pathway as Prof Iliffe states. Pathologising ageing is problematic for very obvious reasons.
I also think this letter touches upon a number of ‘misunderstandings’ of dementia care.
Just because the medications for memory and attention aren’t that successful for many, there’s a huge danger that people are left with the impression that nothing can be done.
Much can be done to improve living well with dementia, including addressing the needs of a person as well as optimising the design of the immediate and built environments.
I must admit that I am biased towards the ‘care’ end of making sure care homes are properly affordable, and something to be proud about. I think that preserving the dignity of a person who happens to be living independently well with dementia, such that he or she exerts control and choice, is a perfectly reasonably one.
I am reproducing Prof Iliffe’s letter below, with kind permission of Prof Iliffe whom I caught briefly at lunchtime today.
Martin Brunet (Rapid response 31st October) adds an important point to the timely and perceptive critique of dementia policy and practice by Le Couteur and colleagues (1). The apparent under-diagnosis of dementia in general practice is presented as a problem needing urgent solution. In my experience few are interested in why diagnoses rates are low. Contrary to the rule of no intervention without a diagnosis, remedies and targets are proposed and pursued energetically.
I suggest eight reasons why there is a diagnostic gap. Changes in thinking, memory and behaviour are not recognised as significant by the individual experiencing them, or by those around them, who may normalise changes as being part of ageing, due to life events or expressions of the personality. Symptomatic individuals may not accept that anything is wrong and resist further investigation. General practitioners may misattribute changes to ageing, well beyond the point of plausibility. General practitioners may protect symptomatic patients from a stigmatising diagnostic label which could place them on an escalator into disability; in doing so they will protect themselves from the consequences of mislabelling. General practitioners who believe that there are few resources to support their patients with dementia may be slow to diagnose. In some patients diagnosis may appear to make no difference to care, or may perversely worsen it by blocking access to rehabilitation or threatening residency in a care home. Memory clinics may have long waiting lists, which lengthen as demand increases. And finally, a formal diagnosis may be made by a specialist but not get recorded in a way that is captured for the Quality & Outcomes Framework reporting.
Different combinations of these (and other) factors may occur in different contexts, making local understanding important. This is not necessarily how the NHS works. The over-emphasis on diagnosis may divert resources away from much-needed community services, in another turn of the Inverse Care Law. Sceptical GPs will be vindicated if low-level support for patients early in the disease course, or palliative care for those at the end of life, fail to meet their needs whilst memory clinics seek extra funding to deal with their backlogs.
(1) LeCouteur DG, Doust J, Creasey H, Brayne C Political drive to screen for pre-dementia: not evidence based and ignores the harms of diagnosis BMJ 2013;347:f5125
To be honest, I was quite happy in my own little world.
I was a house physician at the National Hospital for Neurology and Neurosurgery once. I also did my Ph.D. at Cambridge, and published some seminal papers on frontal dementia.
But I’ll be totally honest with you.
I’m finding the ‘creating commercial opportunities’ narrative of some involved in raising dementia awareness extremely nauseating.
I don’t wish to tar everyone with the same brush – there are some outstanding learning resources and innovations out there, and I can only express my complete admiration for them!
I find it nauseating with some others, however, not least because there’s a lot of factual inaccuracies which creep in on an all too frequent basis.
I’m sickened by the relentless branding of dementia ‘initiatives’.
We all know what “rent seeking” is, but luckily I can spot who the genuine people are. Others may not be so lucky.
It’s clear to me how the real campaigners are, like my friends Thomas Whitelaw, Kate Swaffer or Norman McNamara.
There are also some incredibly talented individuals running community interest groups in this jurisdiction, with remarkable innovations in dementia, such as Zoe Harris or Anna Gaughan.
I’ve written in my own book about how Gill Phillips ‘Whose Shoes’ fits snugly into the personhood narrative influentially shaped by the late great Tom Kitwood.
So none of the following applies to them one jot.
I’m talking about certain people ‘swinging the lead’ blatantly.
This is not a case about whose emblem is more powerful, who has more pledges for NHS Change Day, or how many friends you have in your dementia community.
This is not about how much revenue you’re making, to fund your videos or national campaigns.
This is not about competing for commissioning bids using your strong brand, so that smaller social enterprises never get a look in.
All I want is truth about some of the ‘facts’ presented about dementia.
I don’t want a ruthless competition, where I hear details on an almost daily basis reports of “local activists” standing up in meetings and saying rude and snide remarks about persons with dementia.
I don’t want the invisible army of unpaid family caregivers to become airbrushed from a sober discussion about the shortfall in our social care.
I want the drug companies to be completely open about how close they are with their new drugs for dementia , but also to be very clear about side effects such as liver toxicity. We’ve just seen a national fiasco in how patient choice was totally ignored, in the case of obtaining valid consent, in ‘caredata’, and such managers (or entrepreneurs) have added a new meaning to ‘reap what you sow’.
We are all in it together, but to different depths.
If you carry on with your little games, don’t expect me to be part of them.
Under our law, a mental health condition is considered a disability if it has a “long-term” effect on your “normal day-to-day activity”. This is defined under the Equality Act 2010.
Your condition is ‘long term’ if it lasts, or is likely to last, 12 months.
‘Normal day-to-day activity’ is defined as something you do regularly in a normal day. For example – using a computer, working set times or interacting with people.
There are many different types of mental health condition which can lead to a disability, including dementia. This Act makes it unlawful for service providers to unreasonably discriminate against disabled people. Since the Act was introduced, things have improved for many people with disabilities.
Traditionally, services that discriminate unfairly against disabled people face the wrath not only of the law, but of new generations of disabled people prepared, encouraged and empowered to fight for their rights.
Living well with dementia is therefore not just a societal aspiration. It is a legal necessity.
However, we know that the rights of people with dementia can seem to disappear after the diagnosis. This can happen in small ways. For example people in authority including health and social care professionals may only consult a carer and may make assumptions about what people with dementia want.
This occurs when an organisation (for example, the University, or a member of staff at the University) makes a decision, or puts in place a particular policy or practice, which, on the face of it appears to treat everyone equally, but which actually, in practice, leads to people from a protected group being treated less favourably than other people. This is unless the person applying the provision can justify it as a proportionate means of achieving a legitimate aim.
On a less serious note, does a policy of ‘Dementia Dogs’ unfairly indirectly discriminate against Cats?
Comparing the intelligence of animals of different species is difficult although there are certain tests and problem sets that have proved to be useful. Making the tests equivalent, however, has proved difficult. Dogs are designed to be more efficient runners while cats have better ability at manipulating things with their paws. Thus a test that involved pulling strings or operating levers would tend to favor a cat, while a test involving moving from place to place, where speed is a measure of performance, would favor a dog.
Charles Darwin claimed, “Intelligence is based on how efficient a species became at doing the things they need to survive,” and one might argue that by this definition all species that stay healthy, remain numerous and avoid extinction are equally intelligent.
In the late 1970’s the psychologist Harry J. Jerison developed an alternative measure that he called the Encephalisation Quotient or EQ. It is a mathematically sophisticated comparison of the actual brain weight of an animal compared to the expected brain mass for that animal’s body size. This compensates for the fact that bigger animals tend to have bigger brains and basically shifts the question to one of whether the animal has a larger or smaller brain size than what we would expect for an animal with its body mass.
Based on the encephalisation quotient, the brightest animals on the planet are humans, followed great apes, porpoises, and elephants. The dog is close behind elephants in its EQ. Descending down the list we find cats lower than dogs, followed by horses, sheep, mice, rats and rabbits.
However, a real surprise occurs in some recent data provided by Suzanne Shultz and Robin Dunbar at Oxford University.
They wondered about whether there had been evolutionary changes in the Encephalisation Index. For example, when we domesticate animals, especially a companion animal like a dog, we are placing new demands upon it. Some of these demands are social in nature, such as understanding human communication gestures and words. Dogs are subjected to more of this pressure than are cats. Thus it might be expected that dogs would show a greater rise in their EQ than cats.
This was indeed verified by the Oxford researchers using 511 different samples ranging from extinct species only available as fossils, up through current living examples. Thus it appears that based on their EQ dogs are becoming progressively more intelligent over time while cats have remained at much the same level of mental ability that they had when we first domesticated them. This means that not only are dogs smarter than cats, but the gap between the species is increasing over time.
At the risk of starting another argument, these data may explain why we never hear about such things as a “seeing eye cat,” “police cat” or “search and rescue cat.”
Dementia Dog, one of the five innovative solutions developed through the Living Well with Dementia Design Challenge, is a service providing assistance dogs to people with dementia, helping them lead more fulfilled, independent and stress-free lives.
A sense of routine can often break down for people with dementia. Dogs can be trained to live to a consistent routine. Ultimately, each dog will be trained with the person with dementia and their carer so all three can operate as a team.
In certain cases, functional effects dementia causes can be diverse: forgetting to eat, drink or sleep can increase disorientation, medication can be forgotten and confusion can heighten anxiety about the outside world, increasing isolation. This is a factor to consider for caregivers too.
The dogs are taught to support existing patterns of waking, sleeping and eating for people with dementia.
Through responding to sound alerts they can also help with regular hydration, medication and toilet use.
The social and emotional benefits are potentially huge. Just by being able to get out more independently, in certain cases, the person with dementia can widen his or her circle of support.
If the policy of ‘Dementia Dogs’ does unfairly discriminate against ‘Dementia Cats’ on the grounds of equality, it can be argued that this is legally justified on the grounds of cats having a lower emotional intelligence than dogs.
This would need to be supported by suitable corroborative evidence, such as survey results.
Of cats and dogs aren’t humans, so the Equality Act (2010) doesn’t apply to them.
So I do apologise for wasting your time – but the first bit of this blogpost was important, I humbly submit.
I held a private book launch for guests of mine, who are interested in dementia at the grassroots level.
The talk was dedicated to Charmaine Hardy (@CharBHardy), whose husband has a very rare type of dementia known as primary progressive non-fluent aphasia. The publishers picked her poppy to be the cover of my book.
This for me, as was later suggested, as the book itself is dedicated to the memory of my late father (who did not have dementia but had a severe back pain which severely limited his quality of life in his final years.)
A special mention to Thomas Whitelaw (@tommyNTour) – a true gentleman and a Scot (!)
It was wonderful to meet Darren (@MrDarrenGormley) for the first time. Darren’s clearly someone who sees the person; with superb empathy skills, Darren and colleagues will need to be the change catalysts to break down obstructive silos.
It was a massive honour Beth Britton (@BethyB1886) could make it. Beth, like many in the room, of course knows this subject inside-and-out, and I am personally grateful to Beth for campaigning for the use and validation of more effective assessment of wellbeing approaches.
Here are some happy photos of my book launch.
I really couldn’t have been happier.
I am strongly against promoting my thesis about wellbeing with involvement of people as marketing ‘window dressing’
On the other hand, it gives me enormous pride to present to you the video presentations recorded by Norman McNamara, Kate Swaffer and Dr Peter Gordon which I played to my guests at the Arlington Centre in Camden on Saturday.
Friends of mine, who happen to be currently living with dementia, are also reading the book.
I mention during my presentations the ‘Purple Angels’, including Lynette Richards, Julie Line, Kim Pennock, Jane Moore, and of course Norman McNamara.
And no I am not a retainer from Ostrich Care! x
I feel it would have been it would have been “defeating the object”, if the book could not be read by people living lives with dementia.
Dr Peter Gordon is the only one of the three who does not have a dementia. He is a Consultant Psychiatrist working in this field. It was incredibly nice of him to put together his film for me, shown below.
Dedication • Acknowledgements • Foreword by Professor John Hodges • Foreword by Sally Ann Marciano • Foreword by Professor Facundo Manes • Introduction • What is ‘living well with dementia’? • Measuring living well with dementia • Socio-economic arguments for promoting living well with dementia • A public health perspective on living well in dementia, and the debate over screening • The relevance of the person for living well with dementia • Leisure activities and living well with dementia • Maintaining wellbeing in end-of-life care for living well with dementia • Living well with specific types of dementia: a cognitive neurology perspective • General activities which encourage wellbeing • Decision-making, capacity and advocacy in living well with dementia • Communication and living well with dementia • Home and ward design to promote living well with dementia • Assistive technology and living well with dementia • Ambient-assisted living well with dementia • The importance of built environments for living well with dementia • Dementia-friendly communities and living well with dementia • Conclusion
Amazing … A truly unique and multi-faceted contribution. The whole book is infused with passion and the desire to make a difference to those living with dementia…A fantastic resource and user guide covering topics such as communication and living well with dementia, home and ward design, assisted technology, and built environments. Shibley should be congratulated for this unique synthesis of ideas and practice.’ Professor John R Hodges, in his Foreword
‘Outstanding…I am so excited about Shibley’s book. It is written in a language that is easy to read, and the book will appeal to a wide readership. He has tackled many of the big topics ‘head on’, and put the person living with dementia and their families at the centre of his writing. You can tell this book is written by someone who ‘understands’ dementia; someone who has seen its joy, but also felt the pain…Everyone should be allowed to live well with dementia for however long that may be, and, with this book, we can go some way to making this a reality for all.’ –Sally-Ann Marciano, in her Foreword
Extracts from my talks
This talk was given by me (Dr Shibley Rahman) on Saturday 15th February 2014 to a group of personally invited guests. Guests included persons with dementia, carers (past and present), campaigners, academics in social care, innovation and service provision, dementia club coordinators, and dementia nursing specialists.
1. This is the first segment of the first talk.
Particular things to look out for include:
James Murray-White (@sky_larking) 6 mins
Beth Britton (@BethyB1886) 7 mins
and their @AlzheimersBRACE work
Norman McNamara’s message at 15 mins
@mason4233 (Chris Roberts)’s tweet at 19 mins
2. I start off by thanking Prof John Hodges for his kind Foreword (0) and a clear description from Sally Marciano (@nursemaiden) why she, kindly, felt the book might be helpful. I am honoured at Sally’s personal contribution to my book.
I introduce the topic of personhood, using Tom Kitwood’s seminal work as a brief introduction only, but clearly the topic is huge. I then touch upon the practical difficulties academics and practitioners have had for their definitions of ‘living well’, and the implications therefore for its measurement.
There’s a clearly a debate to be had about why diagnosis might have been so problematic, using @edanaming’s research (Edana Minghella) as a springboard. At around 9’55”, I then use the problems in giving a potential diagnosis of dementia to a person is LGB or T as an illustration.
Gill Phillips (11′ 30″) kindly gives a brief description of the background and philosophy behind ‘Whose Shoes’, a modern application of personalisation which allows service users, including persons and patients with dementia, a say on what they wish to achieve from their person-centred care.
At around 16’30” Lucy Jane Masters (@lucyjmasters), a specialist nurse in dementia, explains the remarkably successful ‘Dementia is my business’ initiative, innovative badges which have acted as an ‘ice breaker’ for bringing about a cultural change in dementia care even amongst health professionals.
This next segment concludes with a brief discussion of the ethical issues of diagnosis, through Dr Peter Gordon’s contribution (@PeterDLROW). I use Peter’s letter to the BMJ as an introduction to the seminal four ethical principles of Beauchamp and Childress (1979), i.e. autonomy, beneficence, non-maleficence and justice. I also include Peter’s video which I will also separately upload elsewhere.
3. I then give an overview of some essential topics germane to this academic debate.
The contributions by the medics have not been a complete farce.
There’s been a lot of scrutiny about the ethical framework regarding dementia from people who are medically qualified, such as Dr Peter Gordon (@peterDLROW), Consultant in dementia. This was been necessary to neutralise some of the potent fraudulent memes in the media from elsewhere.
There’s been wonderful work too by @nchadborn on including service users’ views and opinions into the design of health services, from an applied perspective, as part of Nottingham University.
And the cognitive neurologists have been important in delineating the diverse cognitive presentations of dementia. Prof Facundo Manes’ group in Buenos Aires (@manesf) have been identifying how social cognition in the behavioural variant of frontotemporal dementia can be heavily dependent on context. As an example of this, I explain the Ebbinghaus Illusion and Titchener circles. Prof Manes is a colleague of ours in cognitive neurology, and wrote one of the Forewords to my book.
4. Particular things to look out for now include:
12″ Personal dedication to Charmaine Hardy [@CharBHardy] from England for the poppy on the front cover of my book, and being a key member of the #dementiachallengers
15″ The “Purple Angels” in raising dementia awareness and dementia friendly communities worldwide narrative. Jane Moore and Norman McNamara jointly designed this motif.
21″ beginning of the message by Kate Swaffer (@KateSwaffer), based in Adelaide, Australia, to my guests. (this is the beginning of the pre-recorded message; the second half of the message is in a different video.)
5. This last segment of my recordings contains the second part of Kate Swaffer’s message to my guests, and my film ‘Love is a wonderful thing’ for my community of delegates for the book launch.
The book
The book’s Amazon page, with some testimonials, is here.
The publishers’ page (Radcliffe Publishers) is here.
Independent blogposts by Gill Phillips (one of my guests) about my book launch at the Arlington Centre
These blogposts capture for me what was an extremely happy occasion for me.
One of the biggest illusions, and this is not a ‘complaint’ about this jurisdiction only, is that large dementia charities represent the views of persons with dementia.
They have a myriad of different influences, and certainly it has become dangerous that they legitimise policy directions from which many persons with dementia and caregivers can become totally disenfranchised.
This leaves persons with dementia two options.
The first option is that they can hope to influence large dementia charities better, but this is an impossible task. They act in organised corporate ways, with much marketing and branding power, so if they decide not to adopt the agenda of persons with dementia and carers it would not be altogether surprising.
The second option is to form strategic alliances with general patient groups, but not all persons with a long term condition are ‘users’ of healthcare services which thus far have typically concentrated on illness rather than health.
The third way, and this is in my opinion the most realistic option is to organise better a national and international network of groups focused on the needs of, and run by, persons with dementia.
There are, however, very impressive carers organisations, and many of their competences and aims align with the person-driven agenda for wellbeing.
The uphill task for those of us pursuing a living well with dementia agenda is truly formidable. Cholinesterase inhibitors, the frontline drugs for treating memory problems in Alzheimer’s disease, have annual sales in the billions, but have very modest effects in the vast majority of patients. They do not reverse or markedly slow down the disease either.
I feel that getting in lost in a definition of wellbeing, and how we measure it, is not the way to win the argument, although clearly relevant to how commissioning for integrated care might happen in future, say through value-based commissioning.
I feel arguments based on cause and effect will be more compelling (and easily supported by supporting evidence). That is, memory reminiscence techniques, improving the design of homes and wards, and introduction of innovations such as the ‘Dementia Dog’, which clearly have had a beneficial outcome for many, are options worth pursuing.
The ’cause’ of attracting monies for high quality research, acting as a foundation for pharmacological interventions, is a very worthy one. As someone who has published in this arena in international journals, I certainly don’t have any weird ideological objection to such work.
But we have to acknowledge, albeit reluctantly, that the world is changing, and whether some of us like it or not becoming more “consumer-driven”.
Citizens have become consumers with status proportional to purchasing power, and there’s now a fine line between data gathering of your personal lifestyle preferences through the ‘recreational’ social media and direct targetted marketing of things to improve your health or prevent illness.
The ultimate prize for industry is to determine government policy, but smaller organisations cannot compete against the large corporations, many of which contribute generously to political organisations too.
Where wellbeing campaigners lobbying may not succeed on economic power, their organising ability might succeed on the basis of facts and logic, in seeking out a constructive alternative to the existing policy, practice, or product.
It is often said that the basic rule of pressuring targets is that politicians react to publicity that reflects on their character, bureaucrats react to disrupting their provision of services and programmes, and corporations react to loss of their product’s reputation.
Wellbeing is an agenda for which politicians could have, and have had, much affinity.
If regulations are to be implemented, it’s often possible, hijack or “capture” the regulatory process. This can become easy if the regulatory process is biased towards a medical model of dementia, e.g. the General Medical Council and NICE, rather than social care institutions which are tacitly not given parity.
A committed opponent, who for the most part we’re not interested in reaching because debate with this individual tends to harden his or her position. Big Pharma, the General Medical Council, NICE and large dementia charities are clearly not targets to promote the wellbeing agenda.
The focus in parliament, through the All Party Parliamentary Group, and to some extent helped by powerful allies in the charity and corporate sector, has been relentlessly medical too.
Prof Felicia Huppert, to which my book is dedicated, ran a Royal Society meeting on wellbeing. There is no doubt that this was very succcessful, but we have never had a corollary in parliament.
A legislative hearing, however, gives the lawmakers the opportunity to hear all sides of an issue and to ask questions and challenge witnesses in a relatively brief span of time.
In 1991, the author Michael Frayn wrote a book, A Landing on the Sun, about a British prime minister who tasked his advisers with looking into happiness and what the government could do to promote it. The prize proved elusive, the adviser went mad and died.
Even in November 2010, speaking at the Google Zeitgeist Europe conference, David Cameron suggested, “Wellbeing can’t be measured by money or traded in markets.”
“It’s about the beauty of our surroundings, the quality of our culture and, above all, the strength of our relationships. Improving our society’s sense of wellbeing is, I believe, the central political challenge of our times.”
And this agenda has not sprung out of nowhere.
Aristotle talked about “eudaimonia” – happiness as human flourishing and purpose to life – rather than the modern hedonistic concept. John Maynard Keynes talked about the “art of life” in 1930, and in 1968 Bobby Kennedy told a student audience in Kansas: “We cannot measure national spirit by the Dow Jones average, nor national achievement by the gross domestic product.”
Tacrine was the prototypical cholinesterase inhibitor for the treatment of Alzheimer’s disease. William K Summers received a patent for this use (US Patent No. 4,816,456). Studies found that it may have a small beneficial effect on cognition and other clinical measures, though study data was limited. and the clinical relevance of these findings was unclear.
Tacrine was ultimately discontinued in the US. Unfortunately, it is associated with transaminase elevation in up to 50% of patients. The mechanism of tacrine-induced liver damage is not fully understood, but earlier studies have suggested that genetic factors may play a role.
And now leading Big Pharma companies are involved in an ‘arms race’ to get their drugs to market, and they have powerful allies in large dementia charities worldwide.
Both the AstraZeneca and Merck medicines work by blocking an enzyme called beta secretase that is involved in production of beta-amyloid, a protein that creates brain plaques considered a major cause of Alzheimer’s disease.
Such oral drugs are known as BACE inhibitors and are viewed as a promising new approach to fighting the memory-robbing condition.
BACE inhibitor drugs have taken centre stage after an injectable class of medicines targeting beta-amyloid plaque failed or fell short in trials conducted by Pfizer and Eli Lilly.
Not all experts accept that reducing beta-amyloid is the key to defeating Alzheimer’s, however, and the safety of the new BACE drugs has also been a subject of concern after Lilly pulled the plug on its product due to liver toxicity.
Unlike heart disease and cancer, no major advancements have been seen in Alzheimer’s drug research since the first treatment was approved in 1993 by U.S. regulators.
Of course, the push away from the relative failure of the drug industry should not be the only reason to pursue living well with dementia.
Being disciplined and organising specialist groups to represent only the needs of persons with dementia, both nationally and internationally, will be the only way to promote living well with dementia in the current environment.
They need to ‘capture’ research grant processes, such that we know what psychological interventions work too. They need to ‘capture’ service provision design.
A problem has been the cosiness between the large charities and the Pharma agenda. It is virtually impossible now to detect and act upon material conflicts of interest.
It’s not impossible that the sheer numbers of interested people can act as one large external radical for change. A new organisation, Dementia Alliance International, holds already substantial promise for advocacy for people living with dementia. There is also monumental size of influence of ‘the Carers’ Call to Action’ from the Dementia Action Alliance in this jurisdiction. And size is power.
But I don’t really feel that it should be a competition. The risk, nonetheless, of totally ignoring persons with dementia, their friends, family, or carers, is that the more you ignore them, they more they’ll come back.
Or as Labi Saffre said, “”The higher you build your barriers, the taller I become.”