One of the most difficult issues in mental health is how it is very hard to do ‘outreach’ for people with certain conditions.
You can’t, as such, force people with alcohol dependence syndrome in remission or relapsing to go to support groups such as Alcoholics Anonymous.
A real issue for national policy is how there are individuals who do not wish to have a diagnosis of dementia.
Some feel that they do not memory symptoms severe enough actually to warrant a diagnostic label of dementia. And – to be fair – they could be living with a ‘mild cognitive impairment’ instead.
In an ideal world, you’d want specialist services to be able to work out whether a person is likely to be developing a dementia. This might include the appropriate thinking tests (called ‘cognitive neuropsychology’), a brain scan (such as CT or MRI), or even other investigations (such as fluid off the spinal cord, or blood tests).
Such individuals do a ‘cost benefit analysis': of thinking how much they achieve by telling their friends that they might be developing a dementia, and receiving support or medical treatment, compared to being alienated and being offered no support or treatment.
The fact is that the drugs used primarily to treat dementia do not slow progression, and can help with symptoms for earlier forms of the condition for a few months on average.
So, public health policy faces a situation where some people with dementia prefer to have their diagnostic label ‘invisible’ to others. And this is why this new public health advertisement is so intriguing.
The ad can be criticised in that it gives a very stereotyped picture of a person with dementia: old, pictured against a background of sinister music.
This ad is clearly aimed at increasing the diagnostic rates, which is ultimately one of the key factors by which The Baroness Greengross and the rest of the All Party Parliamentary Group will assess the impact of “The Prime Minister’s Dementia Challenge”.
Oddly enough, the ad says, “He’d started to forget things. It could not just have been old age”. This is one of the five messages of ‘Dementia Friends’, a Public Health initiative delivered by the Alzheimer’s Society.
However, the ad screws up in the sense that dementia does not only present with memory symptoms: in fact people with early stages of semantic dementia, primary progressive non fluent aphasia, behavioural variant frontotemporal dementia, and posterior cortical atrophy can present with plum normal memory.
This leads naturally onto another related faultline in national policy.
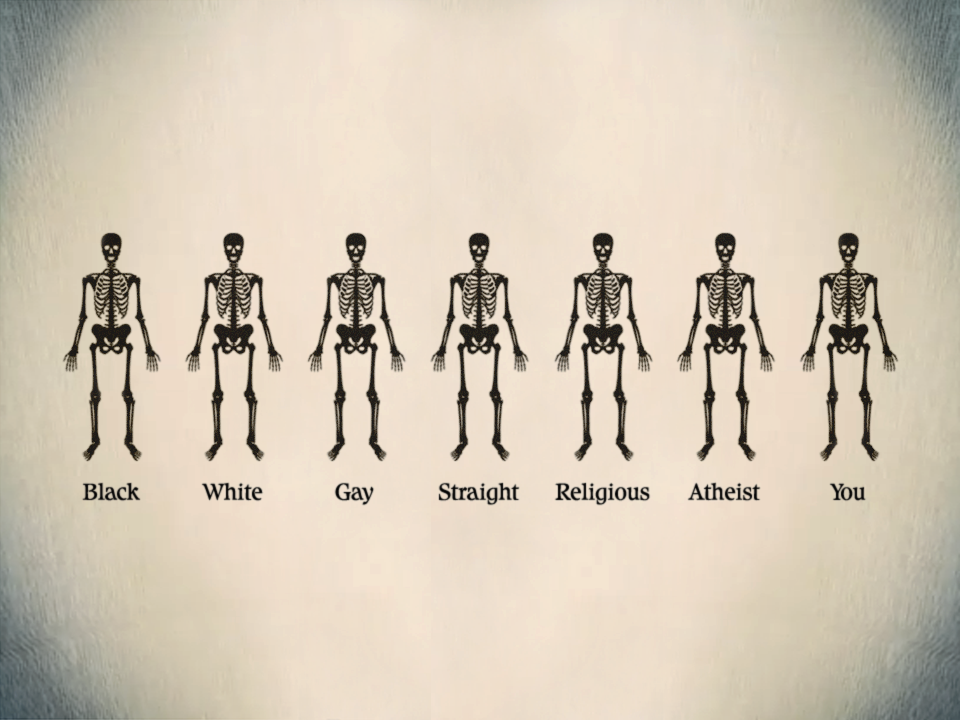
One of the common questions apparently asked in Dementia Friends sessions is “How can you tell a person definitely has dementia by looking at them?”
The actual answer is that you can’t.
And there are clearly ethical limitations to asking people to ‘out themselves’ in saying they are living with dementia, and as such mental health policy mostly does not engage in outreach.
So if you’re building ‘dementia friendly communities’, for the aim of embracing equality (which you have to do anyway under the law), are you somewhat ignoring diversity?
Thanks for this picture shared by Kate Swaffer.
[The picture in the top left corner is from the “Invisible Friends” project, which is something totally different.]
Unknown to me, the title of Prof Banerjee’s talk is an allusion to this famous track from 1979 (when I was five). It’s “Reasons to be cheerful (part 3)” by Ian Drury and the Blockheads.
The Inaugural Lecture – Professor Sube Banerjee (“Professor of Dementia”), ‘Dementia: Reasons to be cheerful’ was held on 26 February, 2014, 6:30 pm – 8:30 pm, at Chowen Lecture Theatre, Brighton and Sussex Medical School, Sussex Campus. BN1 9PX. Details are here on the BSMS website.
I found Prof Banerjee to be a very engaging, ‘natural’ speaker.
I arrived with hours to spare, like how the late Baroness Thatcher was alleged to have done in turning up for funerals.
Brighton are very lucky to have him.
But his lecture was stellar – very humble, yet given with huge gravitas. Banerjee is one of the best lecturers of any academic rank in dementia I have ever seen in person.
Banerjee started off with a suitable ‘icebreaker’ joke – but the audience wasn’t at all nervous, as they all immediately warmed to him very much.
He is ‘quite a catch’. He is able to explain the complicated issues about English dementia policy in a way that is both accurate and engaging. Also, I have every confidence in his ability to attract further research funding for his various teaching and clinical initiatives in dementia for the future.
Most of all, I was particularly pleased as the narrative which he gave of English dementia policy, with regards to wellbeing, was not only accurate, but also achievable yet ambitious.
Banerjee argued that the 1970s which had only given fruit to 209 papers, but things had improved ever since then.
It was the year of course Margaret Thatcher came to power on behalf of the Conservative Party.
In contrast, there have already been thousands of papers in the 2000s so far.
Banerjee also argued that “what we know is more likely to be true” which is possibly also true. However, I immediately reminisced of the famous paper in Science in 1982, “The cholinergic hypothesis of geriatric memory dysfunction”. This paper, many feel, lay the groundwork for the development of cholinesterase inhibitors such as donepezil (“Aricept”, fewer than twenty years later.
It is definitely true that ‘we are better at delineating the different forms of dementia’.
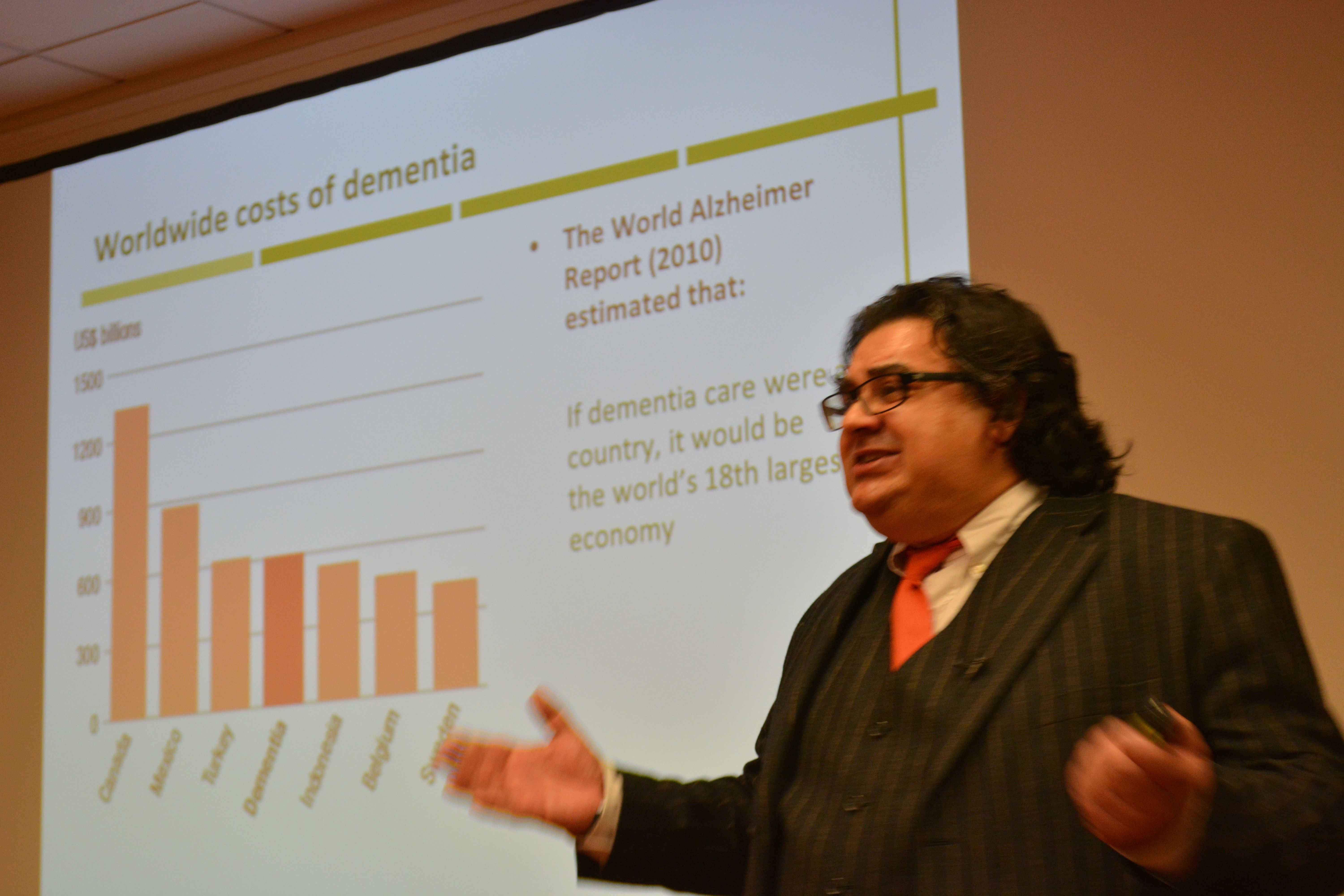
I prefer to talk of the value of people with dementia, but Banerjee presented the usual patter about the economic costs of dementia. Such stats almost invariably make it onto formal grant applications to do with dementia, to set the scene of this particular societal challenge.
I am of course a strong believer in this as my own PhD was in a new way to diagnose the behavioural variant of frontotemporal dementia. In this dementia, affecting mainly people in their 50s at onset, the behavioural and personality change noticed by friends and carers is quite marked. This is in contrast to a relative lack of memory of problems.
Not all dementias present with memory problems, and not all memory problems have a dementia as a root cause. I do happen to believe that this is still a major faultline in English dementia policy, which has repercussions of course for campaigns about ‘dementia awareness’.
A major drive in the national campaigns for England is targeted at destigmating persons with dementia, so that they are not subject to discrimination or prejudice.
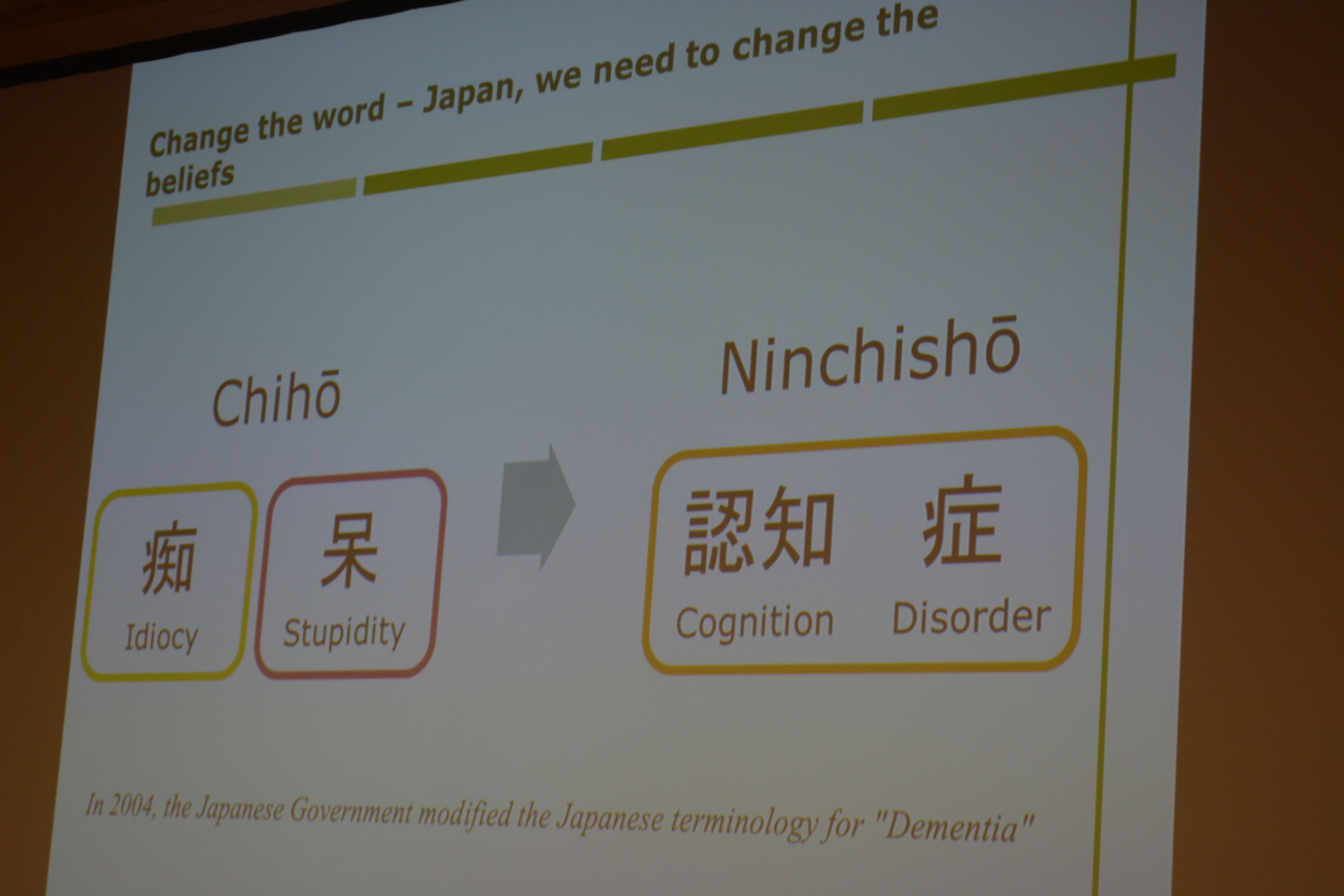
The dementia friendship programmes have been particularly successful, and Banerjee correctly explained the global nature of the history of this initiative drive (from its “befriending” routes in Japan). Banerjee also gave an excellent example to do with language of dementia friendship in the elderly, which I had completely missed.
Raising awareness of memory problems in dementia is though phenomenally important, as Alzheimer’s disease is currently thought to be the most prevalent form of dementia worldwide.
The prevalence of dementia may even have been falling in England in the last few decades to the success prevention of cardiovascular disease in primary care.
The interesting epidemiological question is whether this should have happened anyway. Anyway, it is certainly good news for the vascular dementias potentially.
That dementia is more than simply a global public health matter is self-evident.
I’m extremely happy Banerjee made reference to a document WHO/Alzheimers Disease International have given me permission to quote in my own book.
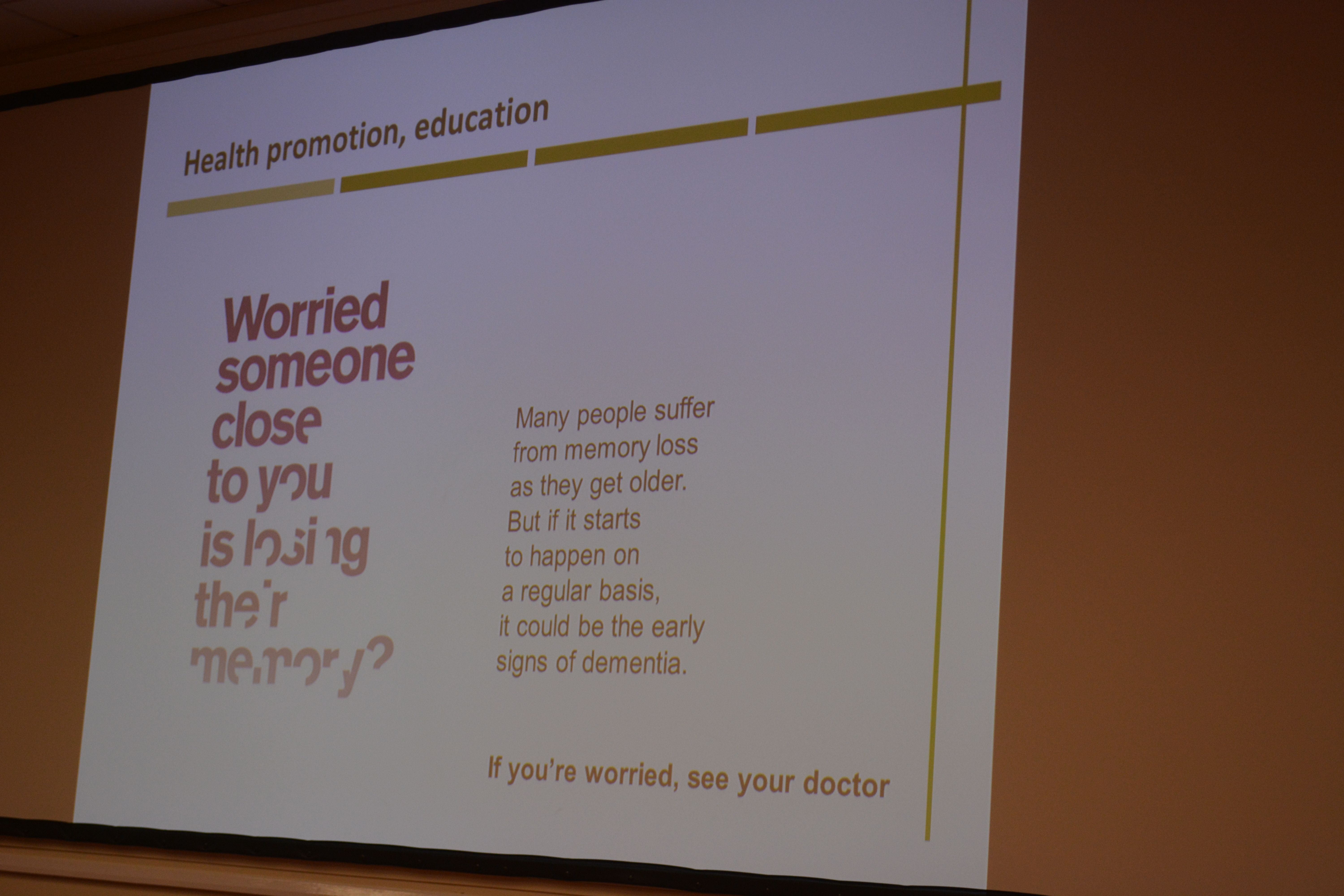
Banerjee presented a slide on the phenomenally successful public awareness campaign about memory.
In developing his narrative about ‘living well with dementia’, Banerjee acknowledged at the outset that the person is what matters at dementia. He specifically said it’s about what a person can do rather than what he cannot do, which is in keeping to my entire philosophy about living well with dementia.
And how do we know if what we’re doing is of any help? Banerjee has been instrumental in producing, with his research teams, acceptable and validated methods for measuring quality of life in dementia.
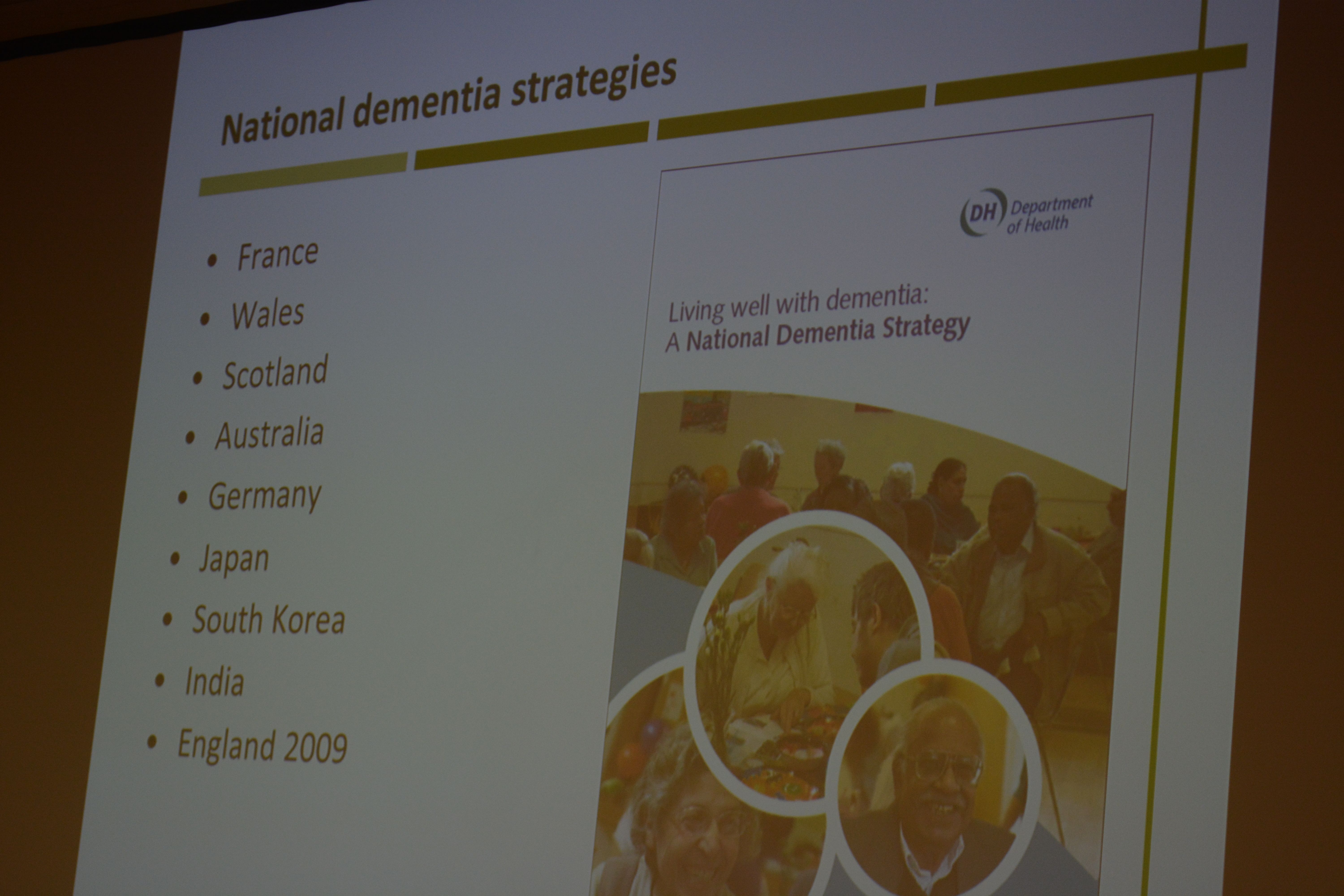
Banerjee of course did refer to “the usual suspects” – i.e. things you would have expected him to have spoken about, such as the National Dementia Strategy (2009) which he was instrumental in designing at the time: this strategy was called “Living well with dementia”.
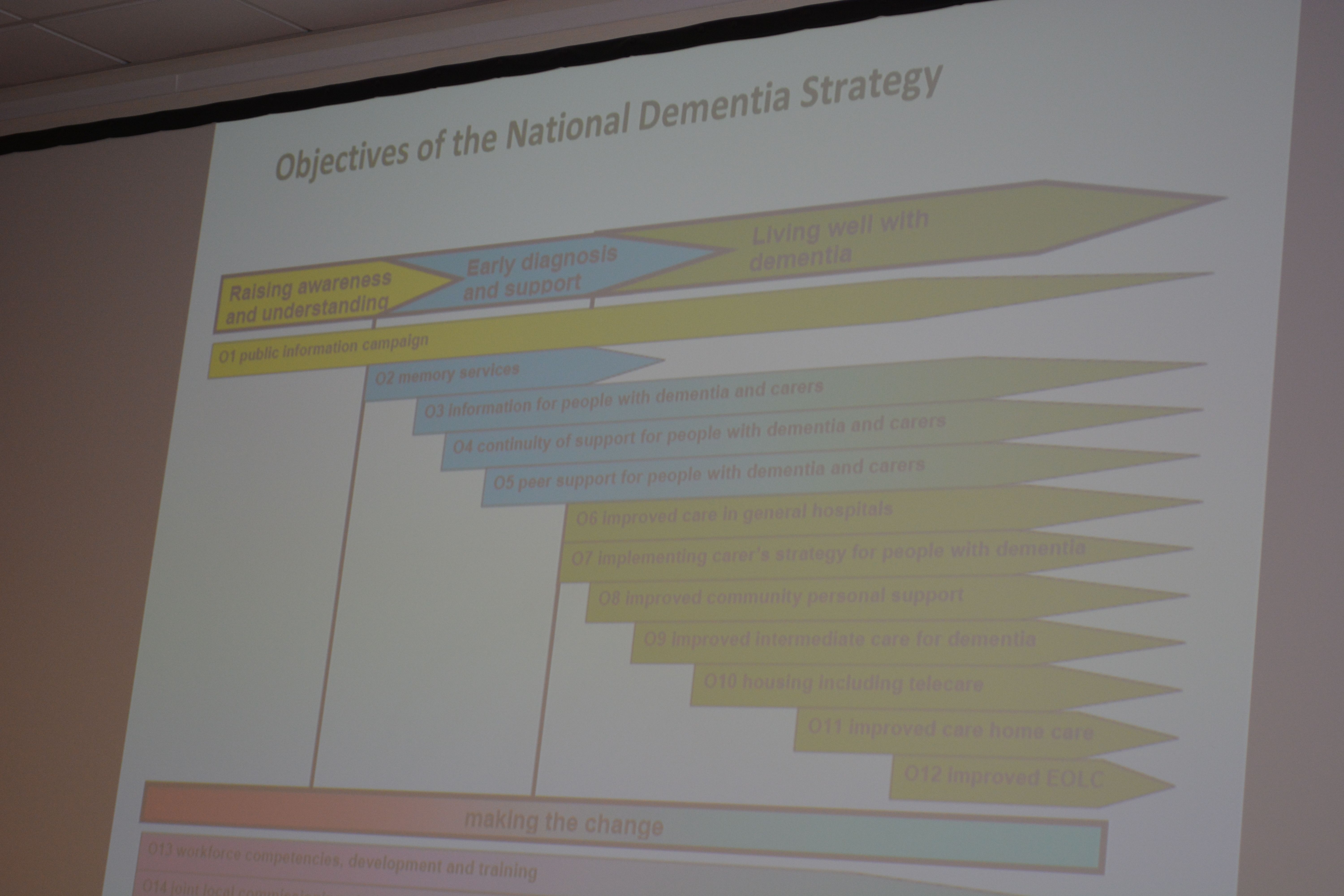
“I’m showing you this slide BECAUSE I want YOU to realise it IS complicated”, mused Banerjee at the objectives of the current English dementia policy.
I asked Banerjee what he felt the appropriate ‘ingredients’ of the new strategy for dementia might be – how he would reconcile the balance between ‘cure’ and ‘care’ – “and of course, the answer is both”, he said to me wryly.
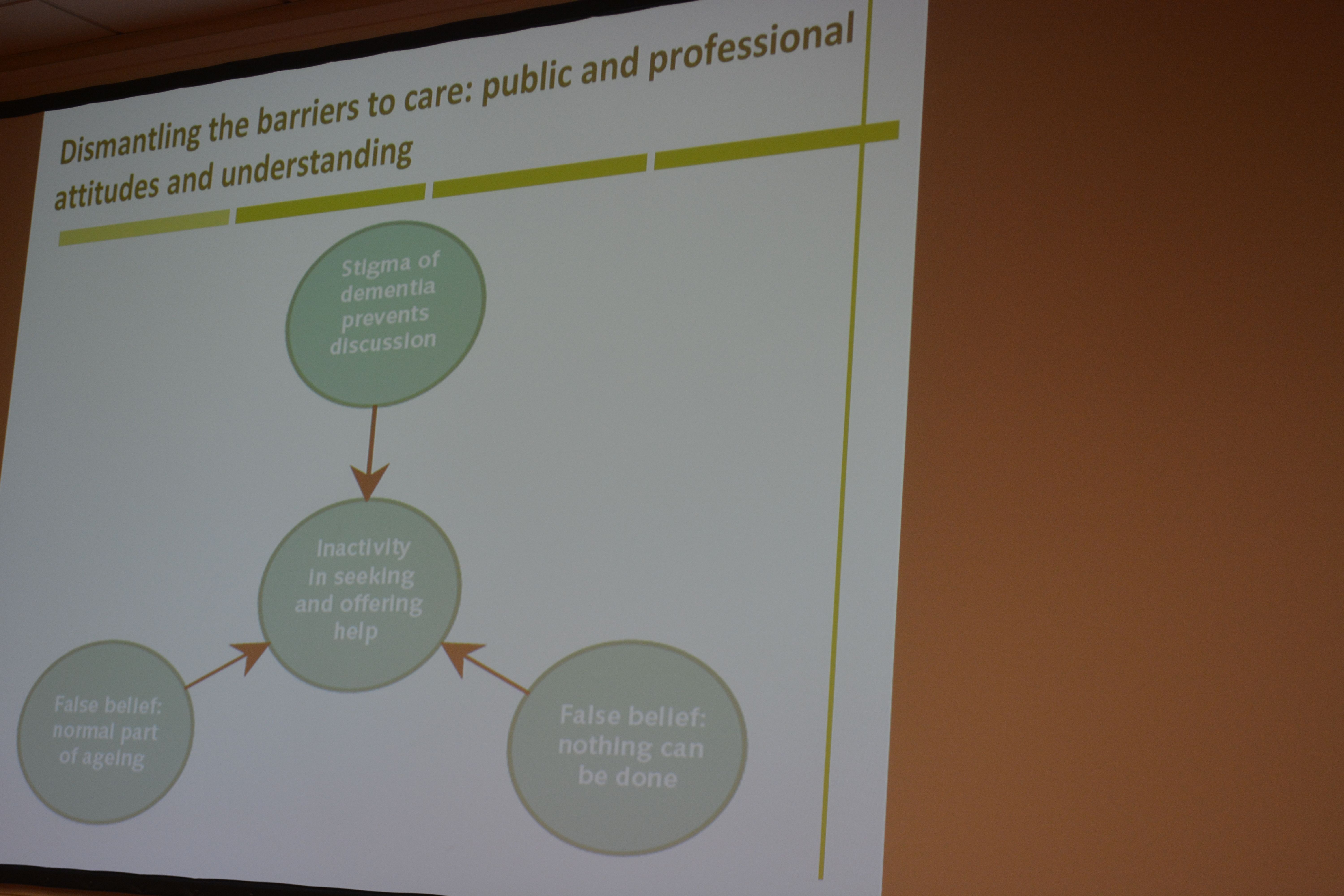
Banerjee acknowledged, which I was massively pleased about, the current ‘barriers to care’ in this jurisdiction (including the known issues about the “timely diagnosis of dementia”.
Clearly the provision at the acute end of dementia care is going to have to come under greater scrutiny.
I increasingly have felt distinctly underwhelmed by the “medical model”, and in particular the repercussions of this medicalisation of dementia as to how grassroots supporters attempt to raise monies for dementia.
I am of course very proud that Prof Alistair Burns is currently reading my book focused on the interaction between the person and the environment in dementia.
And of course I’m ecstatic that Lisa Rodrigues and Prof Sube Banerjee signed my book : a real honour for me.
I signed Lisa’s book which was most likely not as exciting for her! X