Everyone’s personal experience of care of dementia is different.
My description of living well with dementia borders on the super-sanitised, but at the time I wanted to neutralise some of the more fear-based campaigning using metaphors such as ‘battle’ and ‘flood’.
Here are three people pretending to enjoy my book.
Sorry if you’ve just overdosed on “cheese”.
I was brought back down to earth with a thud at the Freud Museum in Hampstead this evening., in “Making Sense of Dementia”, film screenings and concurrent discussion.
The first film, “Ex Memoria”, by Josh Appignanesi, starred Sara Kestelman and Natalie Press. It was based on actual, real life experiences.
Developed with the Bradford Dementia Group, and funded by The Wellcome Trust, ‘Ex Memoria’ has already been distributed to hundreds of careworkers, residential home managers, charities and specialists in the field.
I find it useful as a talking-point of how the care system at worst can refuse to interact with a person with dementia, writing off everything as delusional, even if there is a coherent framework for a belief pattern deep down.
Based on real events, “Ex memoria” takes us into a day in the life of Eva, putting us face to face with one person’s experience of old age and dementia as she moves in and out of the momentary, the half-remembered and the partly imagined.
The spectacle of care staff in communicating in a less-than-meaningful way with persons with dementia in the care home in this film is intensely agonising.
The film was brilliant in demonstrating a culture of exclusion of people being ‘looked after’.
I found the second film “The Waiting Room” intensely depressing, but superbly presented, produced and directed by Jane Harris and Jimmy Edmonds.
First screened at the 8th Annual Conference on Dementia and End of Life (London, December 2013), Jane Harris’ film “The Waiting Room” is about the last four years of her father’s life, spent on a psychiatric ward in his home town of Ayr.
In fact the short film had me in tears.
It describes the filmmaker’s father as effectively left to live in an emotional colourless cubicle.
Her father was left to play at dismantling the bed and counting his clothes, as he was so bored.
For somebody who had won a John Logie Baird prize once upon a time, the audience felt the pain of his degrading treatment, a specific scenario of institutionalised care.
And yet the care staff ensured he was groomed, shaved and washed. But it seemed totally to disempower him of any expression of him as a person.
It illustrates the frustrating experiences of people living with dementia, and the continual confrontation with a system of treatment that can appear, at worst, to fail utterly to make sense of the person’s individual life or experience.
Jane remarked was the care staff ‘treated him like any other patient’.
Somebody further remarked that it was if he was being treated as dead, even before he had died.
Finally, the short film “Keeping mum” by James Murray-White is a fascinating insight into the life changes experienced by his mother.
It does produce glimpses into activities which are indeed promoted in the current national policy on supporting wellbeing in dementia.
These activities might include pottery (James’ mum was a keen potter in her youth), and enjoying opening spaces and gardens.
The film shows too glimpses into his mother’s sense of humour, which was much appreciated by the audience.
To call this short film superb would be an understatement, I feel.
In writing this article, I have no intention of ‘sanitising’ dementia. I’m mindful of two recent comments which fell in my path indirectly: “Dementia is such a cruel disease” (by a daughter of someone living with dementia), and “I don’t know of anyone who doesn’t suffer something as a result of his or her dementia”. The purpose of this article is just to review common motifs in dementia media communications.
When will know when the “war against dementia” is over? This is not an altogether frivolous question, as a MP once famously asked Tony Blair in Prime Minister’s Questions, “When will the war against terrorism be over?”
On 28 November 2013, about dementia, Jeremy Hunt wrote in the Telegraph: “It is a truly horrible disease“.
This set the ‘mood music’ for some of the G8 dementia conference, but the G8 conference was indeed a very positive occasion.
Recently, in “The Loss of Sadness”, Horwitz and Wakefield (2007) wrote that, while depressive disorder can certainly be a devastating condition warranting medical attention, the apparent “epidemic” in modern culture reflects the way the psychiatric profession (perhaps under the influence of pharmaceutical companies looking to widen markets) has understood and reclassified normal human sadness in the DSM-IV as a largely abnormal experience.
The popular metaphorical framing of dementia seems to operate on two levels. It is generalised as a vast, natural or monstrous force that we must “fight”, and it is also located as a very specific condition that affects individuals in extreme ways. In both cases, the effect is to make us feel both terrified and relatively powerless. As Terry Pratchett, who is reported in the public media as having a condition akin to posterior cortical atrophy, viewed: “People seem to think of Alzheimer’s as something rather terrible and dreadful, almost as if witchcraft is involved”
Literally meaning ‘‘away’’ or ‘‘out’’ of ‘‘mind’’ or ‘‘reason’’ in Latin, the actual term ‘‘dementia’’ entered the English language from the French ‘‘de ́mence’’ via the French psychiatrist Philippe Pinel, who made notable contributions to the categorisation of mental disorders in the late 18th and early 19th centuries. Over the centuries, the phenomenology of dementia has been causally associated with witchcraft, moral degeneracy, bad blood and a dissipation of vital energy from the brain, among other factors.
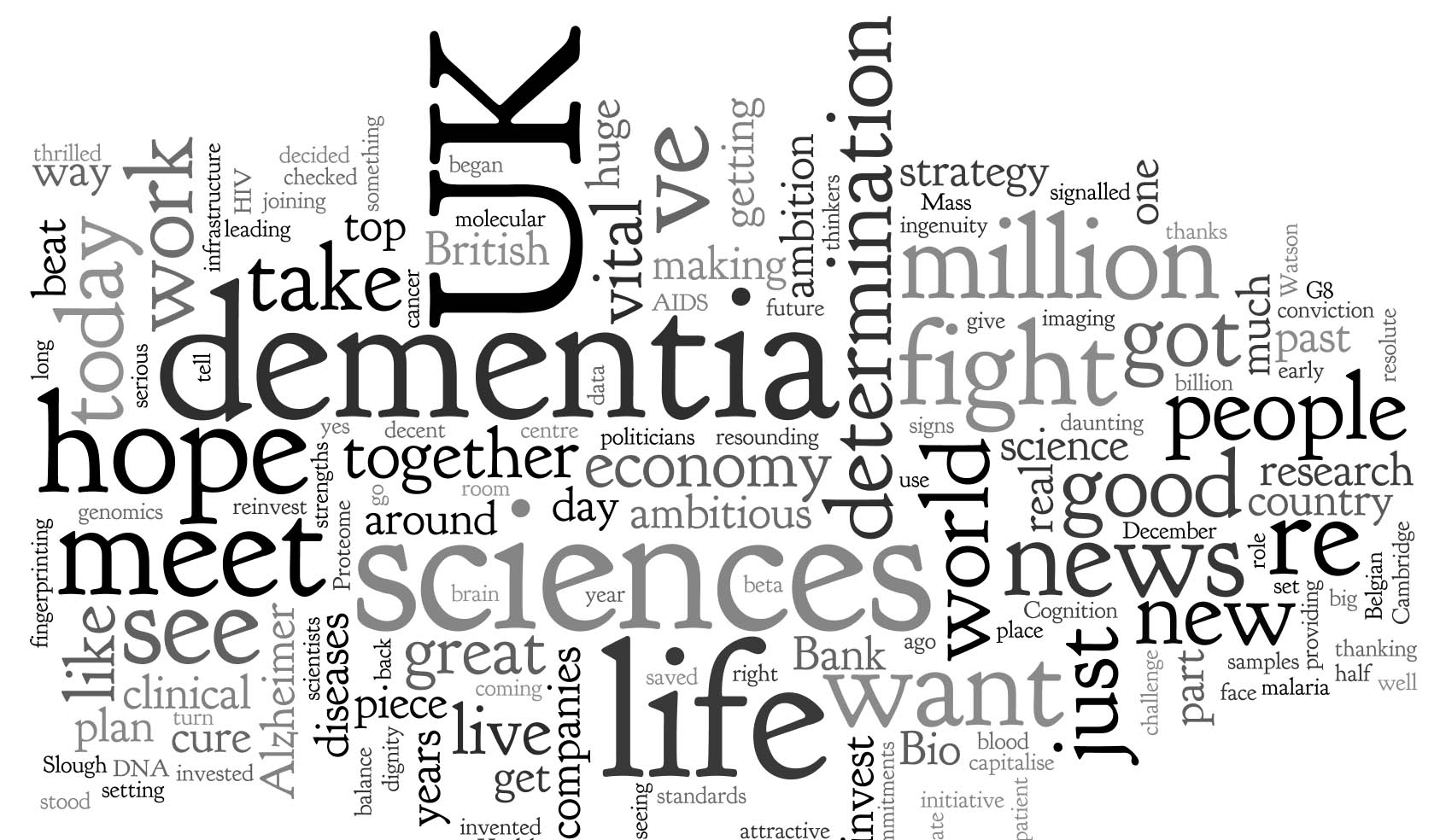
The Wordie for David Cameron’s speech at the G8 summit is indeed interesting, and to be fair in the vast majority is largely upbeat and positive. Whilst there is no recording of the speech on YouTube, the full text of the speech at the ‘G8 dementia summit’ at Lancaster House on 11 December 2013 is available here.
The opening to this speech was pretty chilling, however:
“It doesn’t matter whether you’re in London or Los Angeles, in rural India or urban Japan – this disease steals lives; it wrecks families; it breaks hearts and that is why all of us here are so utterly determined to beat it.”
What exactly is this “it”? What kind of creature is it which steals, wrecks and breaks? This is the fundamental problem. Dementia is not a creature, it’s not an alien, it’s not a mega monster even. It’s an umbrella term covering about 200 different conditions where parts of the brain lost structure and function, leading to problems for that individual; however certain functions remain in the earlier stages, which is why it is potentially unfair to use such graphic language.
“With advances in medical science, the commitment of governments across the world and a willingness from everyone to change attitudes, we truly can be the generation that beats dementia.”
And it’s not the first time David Cameron had used this turn of phrase. In his keynote speech about increasing funding for dementia, the U.K. Prime Minister talked about “the quiet crisis, one that steals at lives and tears at the heart of families” (March 26, 2012). As was noted at the time, this language echoes descriptions of primeval monsters such as Grendel in the Anglo Saxon poem “Beowulf”. Dementia becomes an invader or evil monster that creeps up on people and steals them from themselves. Correspondingly, people living with dementia correspondingly become “victims”.
Noticeably, the Wordie includes “malaria” and “AIDS”. This is because of the following line:
“In generations past, the world came together to take on the great killers. We stood against malaria, cancer, HIV and AIDS and we are just as resolute today.”
“In the Sixties people were too scared to talk about cancer. In the Eighties the same happened with HIV/Aids. After a long and painful journey, we are now much more open about both – and better able to tackle them.”
It seems that this parallel with HIV/AIDS and cancer has been very carefully choreographed. There are indeed some successful treatments for many cancers, but cancer like dementia is an umbrella term covering a wide variety of conditions. A “cure for dementia” is meaningless as a term, as the frontotemporal dementias particularly common in the younger age group are a different pathological entity to the most common type, the dementia of the Alzheimer type.
And how exactly has cancer done? According to the world statistics from WCRF, there were an estimated 12.7 million cancer cases around the world in 2008, of these 6.6 million cases were in men and 6.0 million in women. This number is expected to increase to 21 million by 2030. How is a similar “war” against HIV/AIDS doing? According to AmfAR, more than 35 million people now live with HIV/AIDS, 3.3 million of them are under the age of 15; in 2012, an estimated 2.3 million people were newly infected with HIV, and 260,000 were under the age of 15. Every day nearly 6,300 people contract HIV—nearly 262 every hour.
Dementia has replaced cancer as the “scourge of modern times”. The discourses of the scientific community reinforce this pervasive sense of horror about the dementias. For example, the prevalence of dementias is described in dramatic terms as an “epidemic”. The prevalence of dementia in the UK has in fact thought to be falling in recent times (hence explaining the formidable Prof Burns’ relative unease about dementia being called a ‘timebomb’ by Emily Maitlis on BBC News, a ‘timebomb’ which crucially scientists have failed to address.)
In 2011 in an article entitled “Dementia crusade’s £20m breakthrough”, the Care Services Minister at the time announced a multi-million pound boost in funding for the fight against dementia. The word “crusade” achieves an interesting multiplicity of effects, including an emphasis on faith and battle and on something that not only is metaphysical but can also be “won.” The overall impression is of dementia as huge and ancient, and of massive significance. It appears beyond our grasp and can only be understood through reference to massive natural phenomena (usually disasters) or in biblical/mythical terms.
Flooding is a particular popular literary turn. The danger of flooding has long been associated with dementia. A 1982 UK report was entitled: “The rising tide: Developing services for mental illness in old age“. Rising tides continue to inform the language of contemporary politicians when discussing dementia.
Cameron likes it too, apparently. He referred to the need for Britain to change its attitude to the “rising tide of people suffering with dementia” (May 26, 2012). Alistair Burn’s article “The number of people with dementia in England: turning the tide – Alistair Burns” continued this “tide” theme.
The press and television documentaries abound in “personal” stories about dementia and in tales of cures that are imminent or preventative measures that can be taken to ward it off. Classifying the hundreds of different types of dementia has also been politically powerful. It has undoubtedly facilitated funding and research into diseases for which it is implied that there will eventually be a cure. Ultimately, this broad brush approach is now being used to argue for a “one glove does not fit all” approach: the big corporate winner of personalised medicine, as explained by Cameron thus:
Take just one initiative – Bio Bank. More than half a million people have volunteered to take part in this providing blood samples, getting their vital signs checked, so we can see how diseases like dementia get signalled. The plan is to use Bio Bank to take brain scans of up to 100,000 people – allowing us to see the earliest stages of Alzheimer’s and other diseases. That is the kind of ambition we’re seeing here in the UK ambition that should give hope to people right around the world.
There’s something subtle at work here with the words “ambition” and “ambitious”. Of particular concern to those worried about overmedicalisation is that some experts are now arguing for treating asymptomatic (‘‘normal’’) people with ‘‘abnormal’’ imaging and cerebrospinal fluid biomarker profiles with long-term preventative therapies. This is exactly what seems to be happening here with Cameron’s comment. In a sign of desperation of Pharma wishing to resurrect an ‘ailing industry‘, multi-national Big Pharma believes that early treatment is key to finally achieving a treatment success of any meaningful magnitude.
There are some expected financial memes: like “economy”, “genomics” and “reinvest”. Whilst the spokesmen officially don’t officially promote particular ‘brands’, the speech explicitly mentions UK life sciences companies, like Ixico, Cambridge Cognition, Psychology Online and Proteome Sciences, in developing new tests for Alzheimer’s Disease. As such dementia can’t be seen as “wealth creating”, so the need to promote private markets and innovation is a delicate one to take. However, David Cameron has increasingly appeared giving speeches in the manner of CEO wishing for corporate investment. As such, ‘cure’, not ‘care’, is where the money is at possibly. Cure’s in the wordie; care is not.
“Fight” is THE BIG prominent word. This recurring linguistic device in the cultural framing of dementia is the reliance on military and war-like metaphors. Cameron has been fighting for some time, it’s a wonder he himself isn’t exhausted. On March 26, 2012, he proclaimed rather triumphantly: “We need an all-out fight-back against this disease; one that cuts across society.”
The dementia “time bomb” crops up frequently in U.K. broadsheets and other tabloids. Time bombs are devices that could go off at any time; their most common use has been in politically motivated terrorism. The association of dementia with terrorist tactics is fascinating, invoking the sense of a threat. So when will we know when the war against dementia is over..?
Now listen carefully. As sure as night follows day, academics won’t be able to fight these horrible journalists, destroying the ambitions of people trying to live with dementia in a positive light. Whilst the electoral timebomb continues to tick tock, we can find a cure for this government and their partners trying to demonise those people currently trying to live with dementia. While the war will be long, we can turn the tide on the Pharma companies destroying minds with their false promises, and encourage a new dawn after this crisis where wellbeing interventions are treated seriously at last.
Language is very important. Only this week, the media was stuffed full of talk of dementia being a ‘horrible disease’, and people ‘suffering’.
A recent Telegraph article cited, “Health Secretary Jeremy Hunt says it is “utterly shocking” that only half of people suffering from dementia are being formally diagnosed.”
Society has a certain image of dementia. It really is no use denying that this image is horribly negative, and feeding on this fear can be low-hanging fruit for raising funds through charity.
In this scheme of thinking, those with the dementia are only viewed through the prism of their illness, and this is often reduced to the image of its last and most tragic phases.
It is as if as soon as a diagnosis of a progressive dementia is made, the person in question, it is perceived by the rest of society, automatically becomes incapable of taking any autonomous decisions, loses his/her personality and identity and immediately needs to be cared for.
In reality, however, this illness can develop quite slowly: between the moment when it is diagnosed and the terminal phase, there may be years of development. Moreover, people living with the illness can rarely have the opportunity to express their thoughts and feelings about it: there is communication about them, but only rarely with them. The individual sadly disappears behind the blanket label of an illness.
The term “suffering”, however, sounds negative, and does not support the concept of “personhood”, and certainly does not fit with a philosophy of “hope” and “wellness”.
The way the NHS has latterly been structured as a market also reinforces this customer-supplier master-servile relationship. Dementia care is a ‘service’ you can pay for, with or without a personal health budget.
The dominant notion itself that the need of people with dementia to socialise should be met by “services” is disempowering, for the concept of service incorporates the notions of “providers” and “recipients”; of the “helpers” and “the helped”, of “us” and them”.
These notions further perpetuate the stigmatising assumption that people with dementia are only able to participate in relationships as “receivers”, and that relating to them is a problem for those who do not have the disease: they further advance the widespread perception that people with dementia are, essentially, a “burden” on their families and society.
This term “burden” can perhaps help validate the ‘burden’ some caregivers experience, but should not be assumed and should be avoided when speaking in generalities such as public presentations.
This language and terminology are in desperate need of change, and the prevailing perception of people past the first stages of dementia as just receivers of care, and users of services, needs drastic reframing.
The truth is that, as the symptoms of the disease progress, people with dementia can still play an active role in society, if provided with support, and this support can very often be provided by fellow citizens, rather than by professionals paid to deliver a service.
The purpose of person-centred language is to recognise the impact of language on thoughts and actions, to ensure language does not diminish the uniqueness and intrinsic value of each person.
Personhood is pivotal. This is the standing or status that is bestowed upon one human being by others in the context of relationship and social being. It implies recognition, respect and trust.
The aim is to create the positive conditions where the person can live without stigma; where people are treated with warmth and authenticity, listened to without judgment and are given opportunity for self-expression.
There are, however, ways to ‘reframe’ this debate.
Framing is a fast developing concept, as much in communication sciences as in other disciplines. This is partly due to the fact that it is a rather flexible approach that lends itself to many applications.
When there is a question relating to knowing how a particular subject is presented, in the media for instance, framing immediately springs to mind.
Instead of painting the illness as a homogenous and unchanging totality, it would be preferable to place the accent on its progressive and developmental nature.
One can put the accent on continuing to be a real person despite the decline due to the illness: acknowledge the personality, the identity and the life journey of those with a progressive dementia.
One can also develop empowerment and social inclusion with people with a progressive dementia. Such individuals are more than passive and dependent consumers of help and care services. They have resources that should be mobilized. The principle of inclusion implies that society is composed of all its citizens. However, this needs competent leadership.
Let those who living with dementia speak. It will provide others with one of the most powerful counter-examples in relation to the current dominant image, which often makes the individual disappear behind his/her illness.
Let your respect for those living with the dementia be obvious in what you have to say.
It is useful also never to forget that people with Alzheimer’s disease also have their own life story, their own personality and character. This is because their long-term memories are relatively preserved, due to a phenomenon first characterised by the French neurologist Ribot in the 1880s. Enable these aspects to be expressed too.
Those who disseminate messages, especially via texts designed to influence people, may deliberately choose a frame that the reader is supposed to pick up and appropriate so as to henceforth view reality in this way.
Given that frames form part of any culture, many of them are common to both the sender and the recipient of a given message.
The question of whether framing is a conscious process remains open to discussion: how far will the writer of a given text deliberately choose a frame that serves his own interests?
As we approach the G8 leading on the subject of what is important in dementia diagnosis, research and care, it is all the more important that we frame the discussion properly.
There are so many stakeholders in English dementia policy, it can be quite uncertain know where the current dementia policy has come from.
David Cameron has often argued that ‘it is not where you’ve come from, it’s where you’re going to’. If one of the goals is destigmatising dementia in society, how we articulate the present debate today is vital to our progress tomorrow.
This means not talking about ‘horrible’ and ‘suffering’ in a way as to encourage ‘moral panic’.
This means treating people with dementia, living at all stages with any particular condition, with the dignity they deserve; this will enormously help carers too.