I enjoyed the opening ceremony – though some delegates remarked to me how ‘fit’ the dancers were, maybe indicative of long plane flights to get to the conference venue.
Yesterday, I remarked to the CEO of Alzheimer’s Disease International (ADI), Marc Wortman, as Marc was leaving the hotel, that the Alzheimer’s Disease International conference had ‘interesting dynamics’.
What I actually mean is this.
Speakers from Dementia Alliance International were outstanding. I think Prof Peter Mittler’s talk on how people with dementia must demand access to their rights under the UN Convention for People with Disabilities was a game changer for many. For me, it was the best lecture I’ve ever attended in my lifetime.
I mentioned to some separately that for me Prof Peter Mittler was the equivalent of a premiership footballer, in terms of lecturing ability, when many lesser mortals in comparison look in lower divisions.
I reckon I would’ve actually made it to Dennis Frost’s talk on time especially, not wandered through accidentally half-way through by accident, had Dennis not been advertised as ‘A person with dementia’. This billing on the programme was complete nonsense – as ridiculous as having ‘A person without dementia’ to describe the billing of someone like a policy wonk from WHO.
This was a worthy project which caught my eye.
It was lovely to be recognised by so many at the conference – people whom I had never met before, as well as longstanding close friends of mine. The conference expectedly did have the atmosphere of a family wedding – with people I like and respect there.
I think Jeremy Hughes and George McNamara, senior people at the Alzheimer’s Society, gave excellent presentations. George’s one is particularly relevant to my next book, and contained many many useful avenues for future directions. I think Dementia Friends on principle has good aims, but a real concerted effort must be put now into making meaningful sense of this high cost campaign.
Dementia Alliance International (DAI) is a group essentially run by people with dementia to advocate for people with dementia. But the sheer individual brilliance of the presenters shone through – including Prof Peter Mittler and Prof Mary Radofsky whose contributions were incredibly interesting. There’s no doubt ADI hugely benefited from their presence in the conference, including in the programme list. But I do also feel this is a beginning.
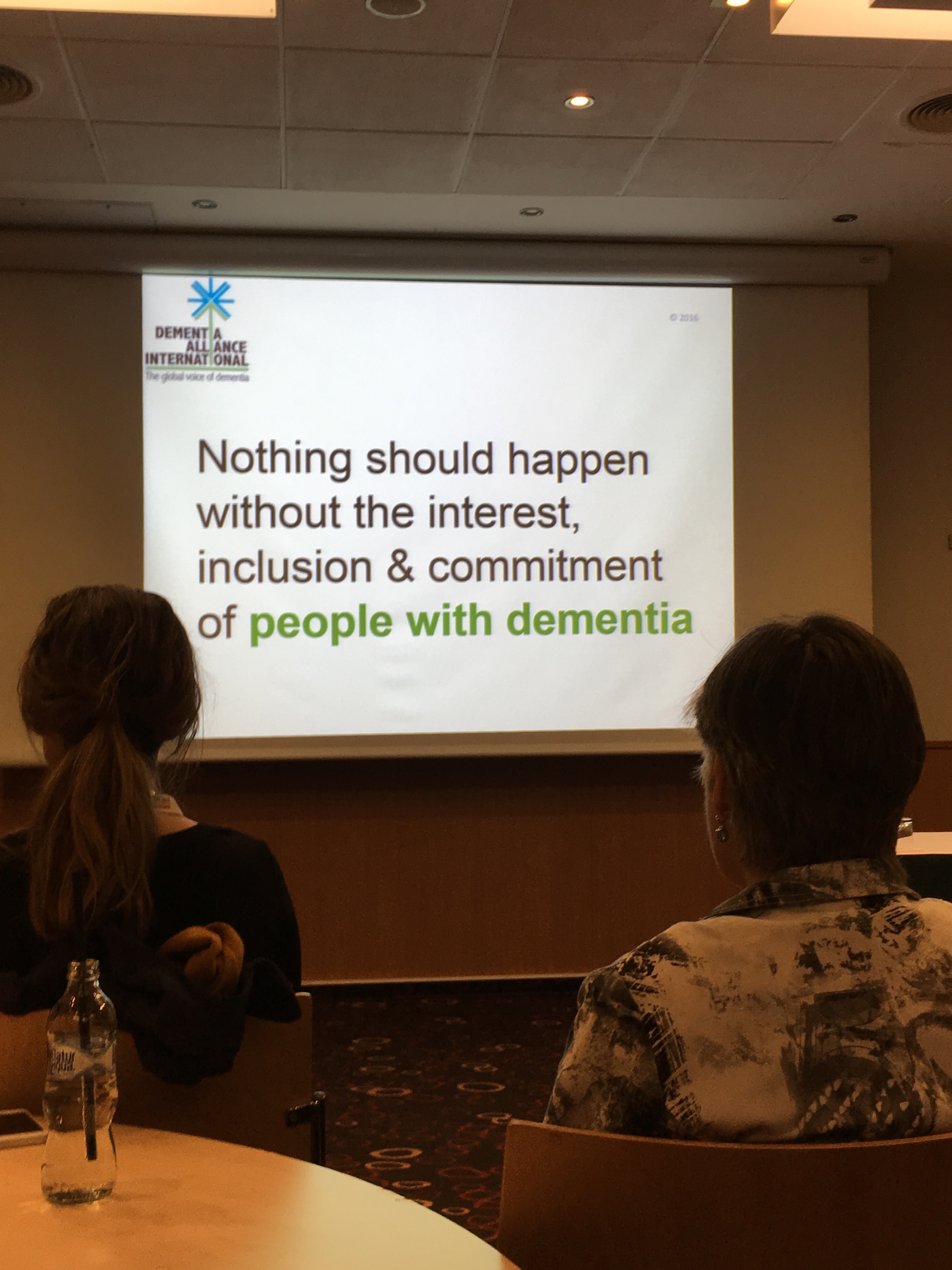
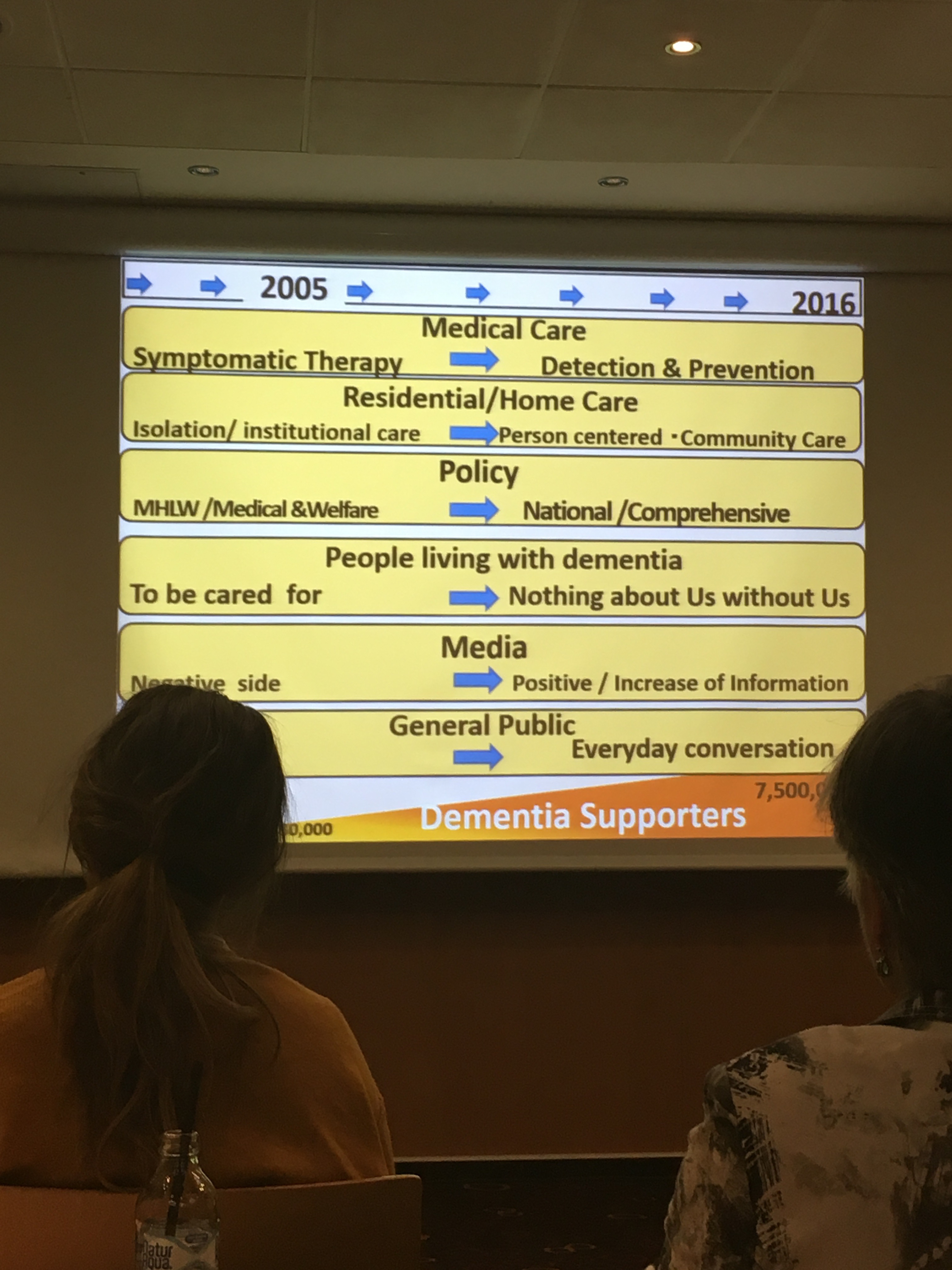
The mood music has changed. DAI has a scarce resource other people want – individual expertise by people with dementia – which many people do not have. It’s clear that the future direction of dementia policy now can be ‘no decision about us without all of us’, and can move from dinosaur lobbying techniques and hospital-dominance to representing the sincere views of people living with dementia.
A day before the first full day, Glenn Rees AM, Chair of ADI, let us know that his Board had approved DAI’s proposal to promote Convention rights, and this would now become their official policy, such that it would be left up to individual national organisations as to how best implement rights-based advocacy. Rights-based approaches, including rights to independent living and right to health, have huge implications for dementia care and support worldwide.
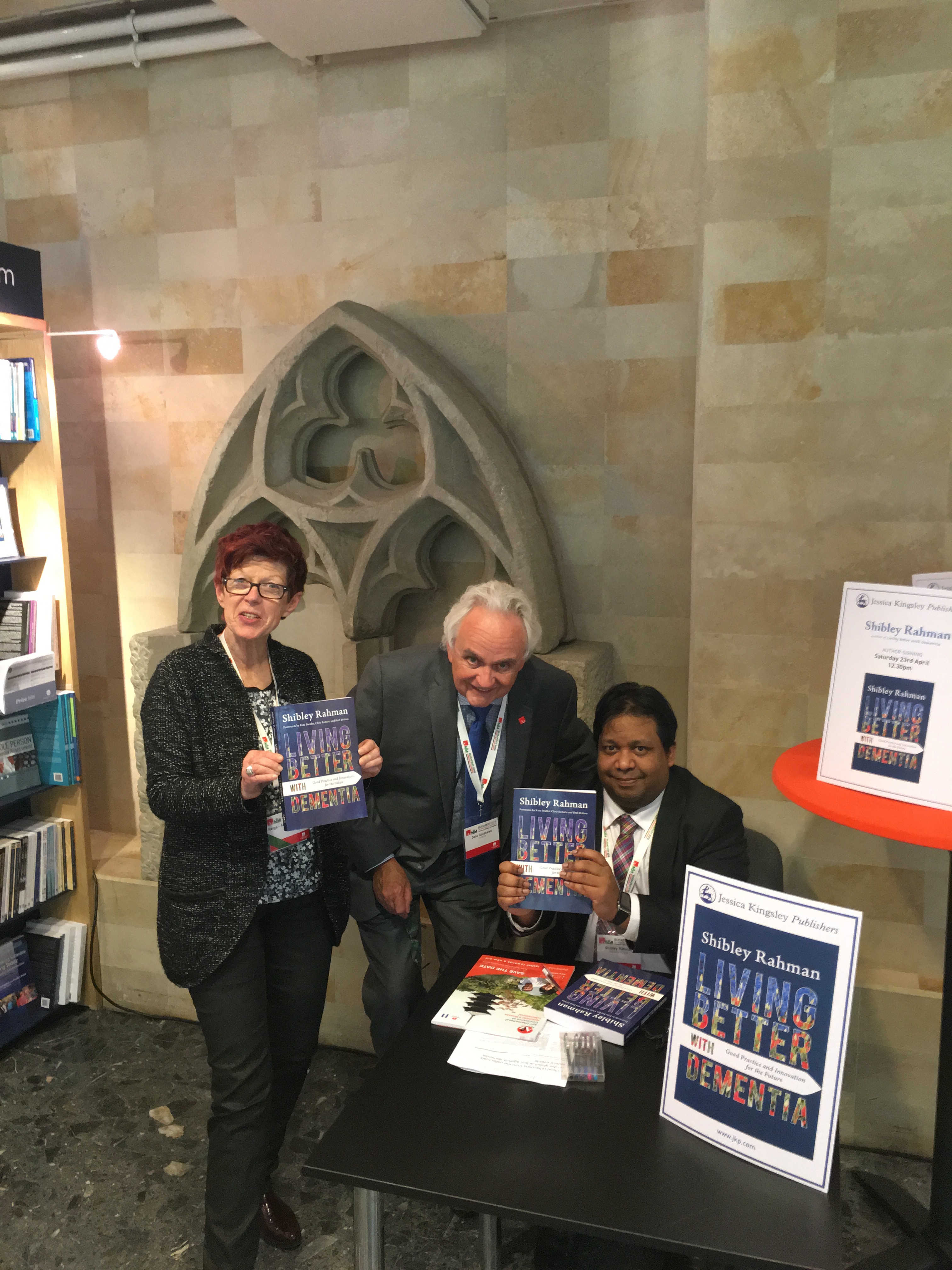
Helga bust a gut to help me with my book signing session.
Thanks very much to Peter Macfarlane from Wisepress for his help for this. Dale Goldhawk, Vice Chair of ADI, even bought a copy!
I had great feedback from my presentation on the awareness of international human rights. Thanks very much to John O’Keefe for chairing this.
Some photos I took are here.
I suppose my favourite ‘times’ of conference was when Agnes Houston made a ‘selfie’ photo of herself for the first time.
And also I think Agnes and Nancy McAdam talking about how they felt really included in Scottish dementia research (#whywedoresearch) on a boat on the Danube was much fun too. A sort of “Alas Houston and McAdam” moment.
Whether or not interventions and initiatives are worthwhile demands long term scrutiny. This is to make sure that initiatives such as ‘Dementia Friends‘, the provision of mass information sessions for the public on some basics about dementia, or accreditation schemes for dementia friendly communities aren’t done, ‘signed off’, and silently disposed of when it’s unclear what the outcomes have been.
It’s always been said that “Dementia Friends”, not ‘training’ but provision of information about dementia, unsuitable for anything higher than tier 1 (in comparison specialist healthcare staff might be trained to tier 3), is a ‘social movement’ “turning communication to action”. In other words, armed with your new knowledge of dementia, you might do something constructive in response.
I have never convinced of a reason for this programme, say, is in improved detection by you of someone slow with their change ahead of you in a shopping queue because of dementia. In fact, getting frustrated at an old person in front of you due to slowness in counting change might be a phenotype of outright ageism, irrespective of the presence of dementia, or simply bad manners. There has been an issue of how the programme might encourage you to behave a certain way towards ‘a person with dementia’. But that is to assume you can identify a person with dementia as if they were wearing a sticker on their forehead with the word “DEMENTIA” in big letters. Many disabilities, including dementia, are indeed invisible. This is akin to not judging a person as ‘normal’ who happens to have an indwelling catheter due to continence issues in multiple sclerosis.
The late Conservative health minister, J. Enoch Powell, famous for various other things too, always warned against the ‘numbers game’. In a break-out session for the Alzheimers Disease International conference yesterday, four speakers from four jurisdictions, including England, Japan, India and Australia, described their perception of what a ‘dementia friendly community’ might be. Kate Swaffer, Chair of Dementia Alliance International, emphasised how such a community should be seen as enabling and inclusive, citing Kiama as an example of good practice.
But other jurisdictions clearly lapsed into “the numbers game” – Japan cited a growing number of ‘dementia caravan volunteers’. the state of Kerala in India offered 100,000 “dementia volunteers”, and Jeremy Hughes, CEO of the Alzheimer’s Society, cited how the Dementia Friends “With a little help from your friends”, slickly produced by professionals, had garnered over a half of million ‘hits’ on YouTube.
Particularly having met Gina at the Alzheimer’s Society conference in London last year, I can say I love the Dementia Friends video as a creative pitch.
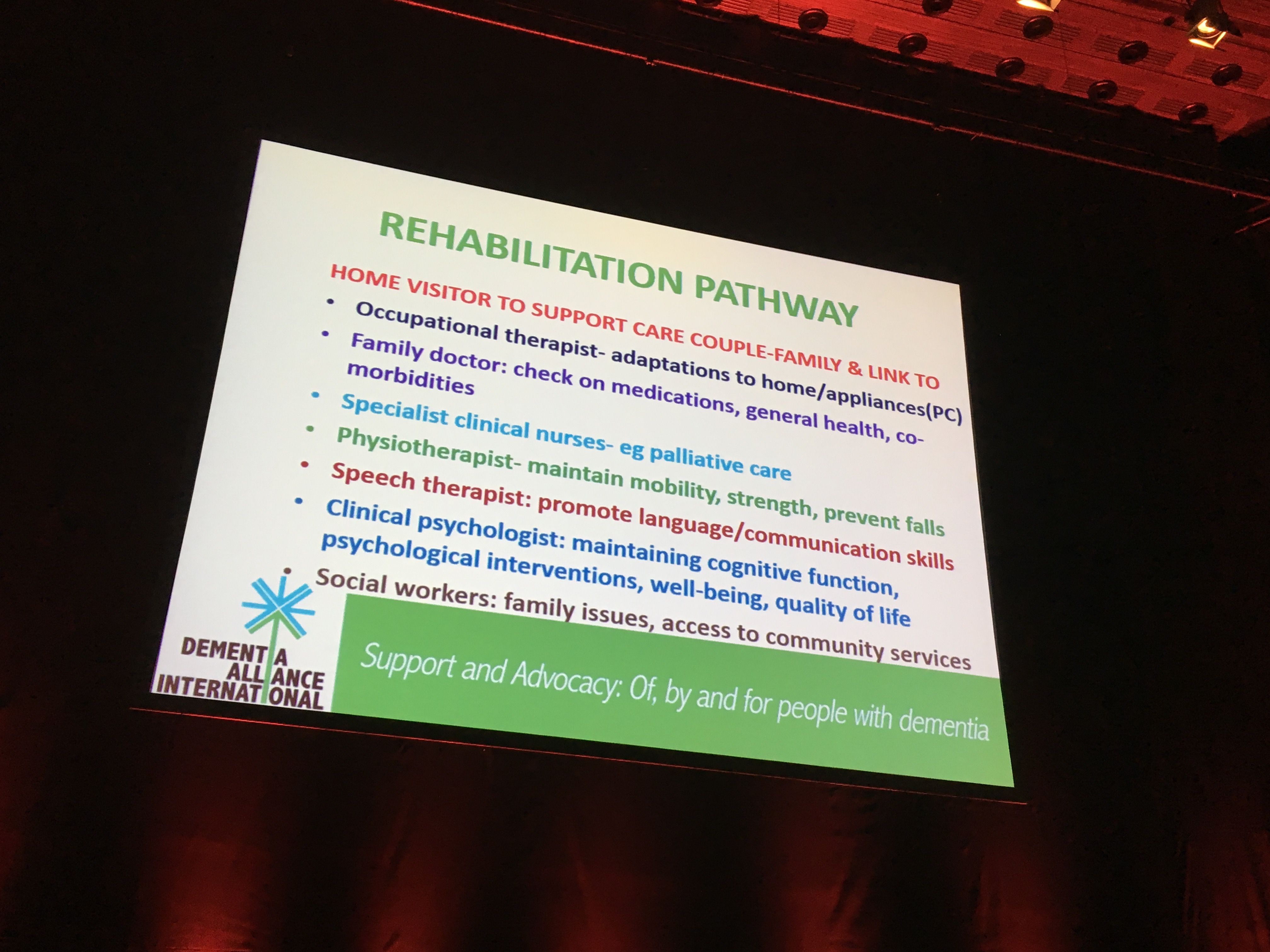
But there is a moral imperative to see what these dementia programmes are doing, not least because the substantial cost of a public backed initiative might be at an opportunity cost to other equally meritorious approaches, such as improving rehabilitation services for dementia. Also, there is a fundamental wish, surely, to know whether the initiative has met any of its original ambitions.
The original English dementia strategy, “Living well with dementia”, was supposed to last five years, and indeed did so from 2009. There was never a renewal of this strategy. There was instead an overwhelmingly underwhelming‘implementation plan’ for ‘Dementia 2020′ from the Department of Health, which did not address the Baroness Greengross’ stated wish to log the ‘lessons learnt’ from the successes and failures of the original strategy.
In this strategy, it was clearly stated that English dementia policy had to prioritise mitigation against stigma and prejudice towards dementia. Of course, there can be ‘unintended consequences’ of so-called ‘dementia awareness’ – a substantial number believe that queuing in a shopping queue called ‘dementia friendly checkout’ or parking in a ‘dementia friendly car parking space’ in fact markedly exacerbates stigma, and is potentially quite offensive.
Even a badge, rather than encouraging inclusion, can impose an unintended ‘them and us’ distinction.
So the idea of “Dementia Friends”, or any other jurisdictional attempts to emulate this, being a ‘social movement’ is deserving of scrutiny, and should not glibly assumed.
Consider this. Say there are 2 million people who go out each to buy a Mars Bar, a homogeneous product, following an intense publicly funding marketing campaign set up by top quality marketing agencies. Could be said that 2 million purchases of Mars Bars was a social movement of Mars Bar friends – or simply an anticipated benefit of a mass marketing ‘top down’ broad sweep campaign?
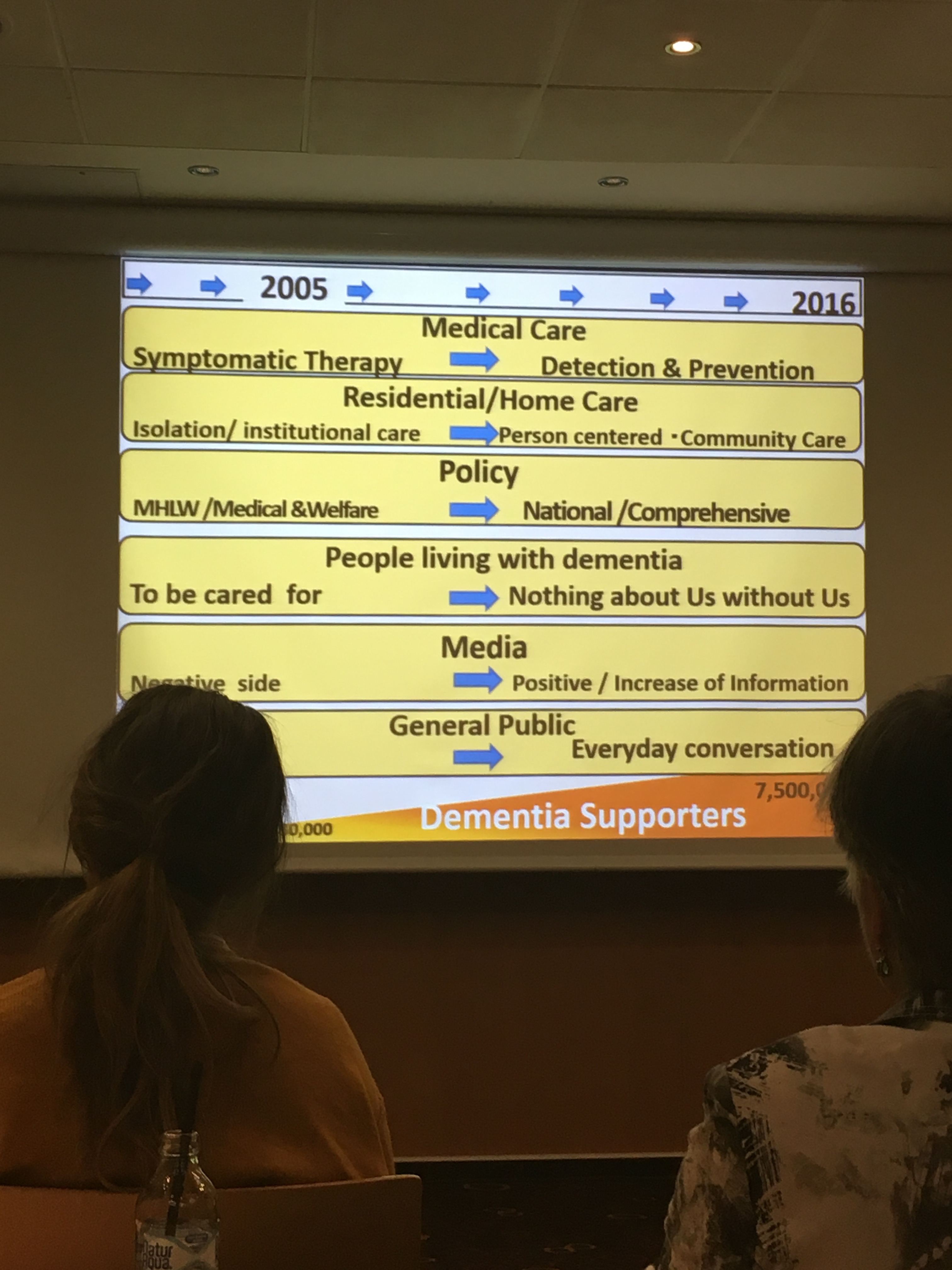
The talks from the other jurisdictions indeed touched upon what might have been reasonable outcomes.
Say, for example, in Japan.
And indeed there are a number of possible ways in which you could consider ‘Dementia Friends’ has been of benefit.
These might conceivably include:
reduction of stigma and prejudice in public perceptions
better knowledge of dementia and how dementia impacts on personal lives
uptake of ‘dementia friendly initiatives’ in quality of care, such as ‘dementia friendly hospital wards’
better ‘customer experience’ from high street businesses or corporates
better perceived ‘quality of life’ of people living with dementia and those closest to them
better awareness of possible symptoms of dementia thus promoting more timely diagnosis of dementia
increased confidence of people with dementia living independently (not in isolation) in the community.
It is not fair and appropriate to reduce this into two or three questions, say “how much more confident do you feel about dementia?”. People invariably don’t know the sample size, or any other thing about basic demographics of the sample.
I have noticed a huge drive in Dementia Friends, and in fairness other jurisdictions too, to play ‘the numbers game’. So, at first, you are seeking one million friends – and then you can make the website deliver more friends more easily – so the number increases for little further effort. But this is being accompanied by a marked shift in societal attitudes in dementia? It’s like my mass marketing of Mars Bars analogies.
A social movement for me also implies that the people delivering the information session have some intellectual investment in the process. This is not true of Dementia Friends, which specifically wants Dementia Friends Champions to deliver the same product as advertised – as indeed a Big Mac is the same whether you buy it in Doncaster or Dubai. The organisers of Dementia Friends clearly do not want Mars Bars accidentally turning into Snickers, by the addition of a few peanuts, by a few ‘rogue champions’.
One or two companies delivering a ‘better customer experience’ will be an expected outcome from those companies which have invested money in such a programme. The issue is whether this is replicable through means such as ‘secret shoppers’.
So, all in all, it is of vital importance how you actually measure the efficacy of the social movement. I indeed asked this as a general discussion point in the session chaired by Glenn Rees, the Chair of Alzheimer’s Disease International.
And of course there are a number of ways to tackle this question.
Jeremy Hughes mooted the idea of high quality survey data. I think this would be far superior to relying on a quantitative analysis of pledges from the pledge card. For a start, there is a problem with potentially low response rates for pledge cards. Secondly, whilst easy to codify, the information from the pledge cards are only as good as the quality of the pledges you can pick from in a multiple-choice fashion. For example, in my experience as a Dementia Friends Champion, I have learnt that many people want to ‘join dementia research’, as it gives them some agency and hope about dementia. And yet this is not a stated pledge. It does concern me how slow Dementia Friends has seen to be in working with NIHR in fostering links between the ‘Dementia Friends’ and ‘Join Dementia Research‘ initiatives?
Formal assessments do of course exist of the ‘success’ of social movements. But for the reasons I describe above actually identifying the outcome measures is itself tricky.
Take for example the ‘social value return on investment’ (SROI).
The key assumption of SROI analysis is that there is more to value creation than purely economic value, indeed the value creation process can be thought of as a continuum with purely economic value at one end, through to socio-economic somewhere in the middle, and social value at the other end. Economic value creation is the raison d’etre of most for-profit corporations (i.e. taking a product to service to market that has greater value than the original inputs and processes that were required to generate it), whereas social value is created when ‘resources, inputs, processes or policies are combined to generate improvements in the lives of individuals or society as a whole’.
Social value creation is a huge goal for the third sector in facilitating social inclusion and access for those that may be marginalised). However, unlike economic value, social value is difficult to quantify, varies according to the type of organisation involved in its creation and does not have a common unit of analysis (such as money) that enables it to be easily standardised and compared.
Social Movement Impact Theory (otherwise known as Outcome Theory) is a subcategory of social movement theory, and focuses on assessing the impacts that social movements have on society, as well as what factors might have led to those effects. It is relatively new, and was only introduced in 1975 with William Gamson’s book “The Strategy of Social Protest,” followed by Piven and Cloward’s book “Poor People’s Movements”.
Finding appropriate methods to use for studying the impacts of social movements is problematic in many ways, and is generally a large deterrent to scholars to study in the field. The first problem scholars ran into was defining “success” for social movements; the significance of this is that key stakeholders often have disagreements of what a movement’s goals are, and thus come to different conclusions about whether a movement has “succeeded.” Argos might have different outcomes in mind to Addenbrookes Hospital in Cambridge?
Other issues arise when one attempts to locate a movement’s impact in all arenas. Impacts are most often studied at the political level,and yet it has been proven that they have individual, cultural, institutional, and international effects as well. Is exporting an operational homogenous product the same as propagating a wider social movement?
The psychology of the individuals who participate in movements are normally profoundly affected. But do the 1.5 million ‘Dementia Friends’ feel any sense of connectedness to one another? One suspects not, especially if some have achieved ‘Dementia Friends’ status through a few minutes on a computer terminal in isolation.
Has Dementia Friends shifted quality of care or attitudes in care homes, for example? Has it shifted political attitudes to dementia which have historically been shaped by much political lobbying? One parsimoniously thinks not if the current Government wishes to shift emphasis now to diabetes, and has not even renewed post 2014 the English dementia strategy.
Inevitably within government there continues to be an interest in and application of techniques for program or project evaluation such as cost benefit analysis. And this from an utilitarian perspective makes complete sense – in terms of society’s assessment of ‘getting most bang for your buck’.
Lessons for Dementia Friends can also be usefully learnt from other arenas.
For example, an interesting example of an impact evaluation is provided in a report from a few years ago. This report was entitled “An evaluative framework for social, environmental and economic outcomes from community-based energy efficiency and renewable energy projects for Ashton Hayes, Cheshire March 2012″ , and was published from the nef (the new economics foundation).
Ashton Hayes is a rural village located just outside Chester. Their aim is to become the first carbon neutral village in England, through energy efficiency measures and carbon offsetting; by: ‘…encouraging everyone in their community to think about how their way of life affects their impact on climate change and to help people to understand how simple actions can make a big impact on carbon dioxide emissions to the atmosphere.”
The report helpfully discusses choice of indicators.
It was proposed that all stakeholders are often the best people to identify indicators, but a common mistake is to misinterpret what is meant by ‘measurable’. One should avoid the trap of using inappropriate indicators just because they are readily available; so, if the outcome is important, you will need to find a way to measure it.
Outcomes work also concedes that effect of some outcomes will last longer than others. Some outcomes depend on the activity continuing and some do not. For example, in helping someone to start a business, it is reasonable to expect the business to last for some time after your intervention. The difference between ‘benefits’ and ‘outcomes’ is therefore imperative in this context. The outcomes of a campaign such as ‘Dementia Friends’ will be valid as a snapshot in one particular time.
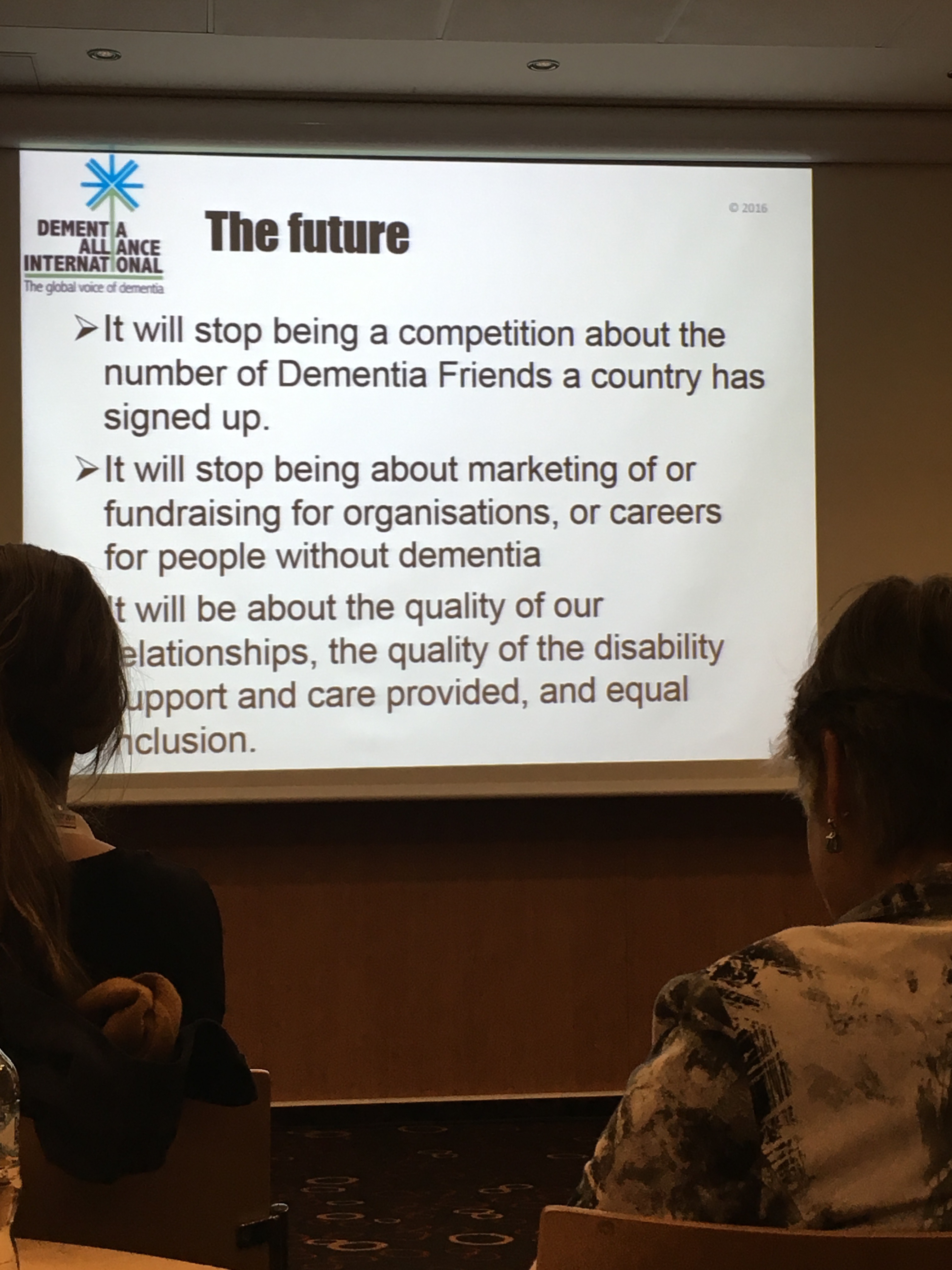
I feel things will change say when people with dementia are genuinely considered as ‘equal and reciprocal partners’ in any relationship. For example, it should be an automatic given that dementia friendly communities include people living with dementia as paid consultants, not tokenistically ‘involved’.
Kate Swaffer successfully conveyed the sentiments behind this for Australia yesterday, for example.
And I think that is the way things are heading now with the Alzheimer’s Disease International umbrella approach of inclusion and a strong ‘rights based approach’, which hopefully will now filter down to national agencies for implementation.
I feel that how ‘successful’ Dementia Friends has been, given the statement below when the initiative was first announced in November 2012, needs to be comprehensively examined.
And ultimately Dementia Friends has to be much more than a successful, easily exportable, marketing campaign – it needs to deliver results on the ground. This is no different for the Alzheimer’s Society and the Government as it is for small social enterprises. The rules of the game must be equally applicable to all, otherwise it’s an “unfair market”.
Dementia enabling communities primarily needs to be for the benefit of people living with dementia and their closest.
Chris Roberts, living with mixed vascular and Alzheimer’s dementia, stated clearly in a session run by Angela Rippon at the Alzheimer’s Show: “It’s not only awareness we need: it’s actual education”
He was of course referring to the mushrooming of ‘dementia awareness’.
At one level, “awareness” is very basic. It’s called “tier 1″ in the jargon, as the ‘entry level’ for how services for dementia could be organised.
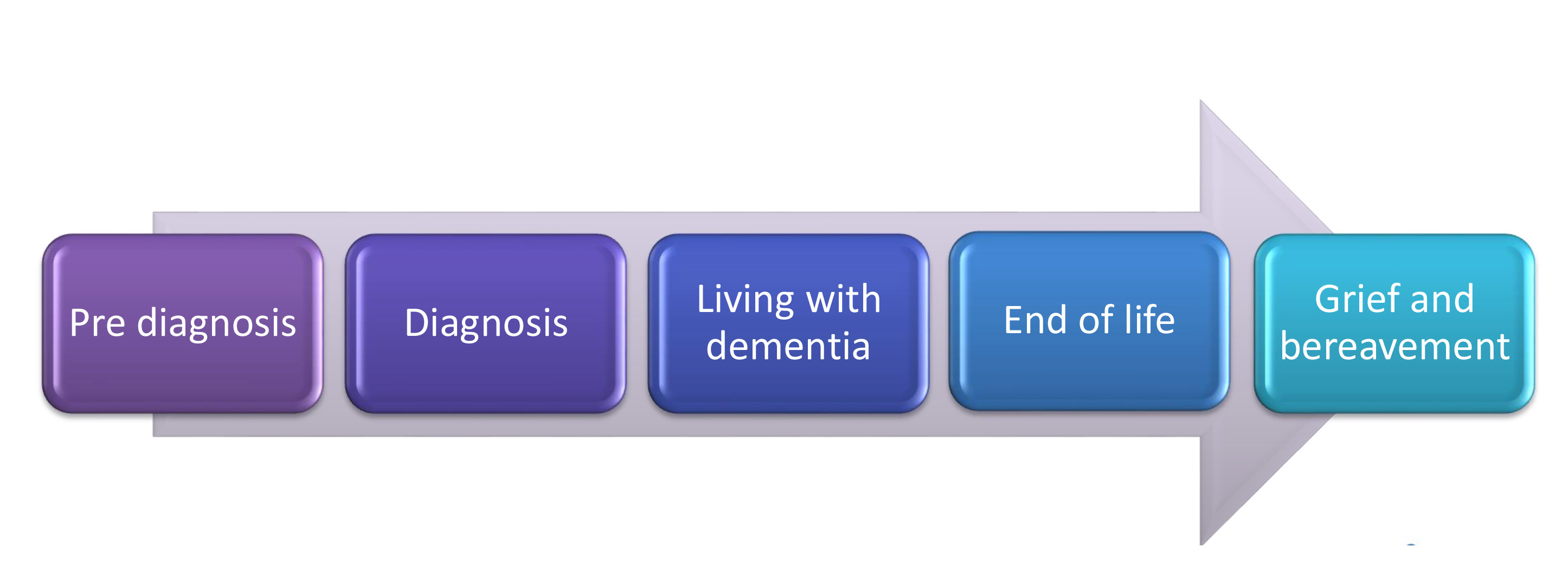
Ceri Hodgkison and Dr Karen Harrison Dening in a talk at the Royal College of Nursing explained how dementia care lies on a continuum at the Royal College of Nursing the other week.
A concerted effort must now be made into why many people find the actual disclosure process of the diagnosis of dementia very unsatisfactory. This must aim at looking at why the beliefs, concerns and expectations of the imparting of that information fell below standard, sometimes, and there must be mechanisms for acting on that at an individual basis.
The English nursing strategy provides for a diversity of nurses involved in care: ranging from “dementia aware” to “dementia knowledgeable” to “dementia specialist”.
There has been a drive to denegrate specialist knowledge, in a general drive towards ‘generalists’, but I feel strongly there is a place for all contributions. Simply, awareness is not enough.
The complexity of dementia service provision in part comes from the unique way in which the brain can be affected in the hundred or so different types of dementia. Dementia, however, I would humbly submit poses considerations of its own. It directly affects how the person communicates with the world, and this can potentially alter the dynamics and perception of that person.
It also poses clinical issues for the National Health Service and social services. A person living with dementia as such is unlikely to present to the NHS with ‘an acute exacerbation of dementia’, though in one sense might do such as repeated falls. A person living with dementia as the condition progresses is likely to accumulate an increasing number of other clinical diagnoses which need addressing; they may affect the decision for transition into a residential care setting.
A person living with dementia may enter an acute hospital setting from one of many other care settings; such as CMHTs, hospices, care homes, nursing homes, or even directly at home (if the emphasis has been on ‘self care’).
A member of the family will often find himself or herself as a pivotal person involved in the care and/or support of a person with dementia. He or she can know things other people will not know.
So when a person living with dementia enters a care setting, there is a fundamental change in dynamics which happens. Often a member of the family, thus far in a caring role, finds the care being transferred to relative strangers. But there, in fact, remains a ‘threesome’ – the person with dementia, carer, and member of staff (such as nurse, allied health professional, etc.)
In a paper published in Dementia journal in 2014 from the School of Nursing and Midwifery at Monash University, Australia, the authors looked systematically at the experience of family caregivers of people with dementia who were admitted to hospital.
People who are ‘family caregivers’ clearly have substantially more than an ‘awareness’ of dementia. They are in effect ‘experts’ of care, who take their responsibilities of care extremely seriously. They can have substantial care and support needs of themselves.
One sentence in this paper really caught my attention.
“Carers often have a negative experience with hospital care (Jurgens et al., 2012) and can feel overwhelmed and under-noticed by the system and the teams of clinicians who work within it (Haesler, Bauer, & Nay, 2007).”
And yet this the very opposite of the ‘triangle of care’ proposed in a strong contribution by the Carers Trust/Royal College of Nursing.
This is a massive deal: as people very close to a person living with dementia find themselves rapidly acquiring ‘visitor status’, in an institution, according to the authors.
And the emotions can be huge in being asked to respond to their experiences.
“One participant said that it was a relief to be able to talk confidentially about her feelings to someone external and that ‘Noone had asked her how she felt before ’. Another who was crying intermittently throughout the interview was asked by the researcher whether she would prefer to stop the discussion. She responded ‘No, it’s a relief to get this all off my chest ’.”
We need also high quality research, rather than marketing, into the ability of stories from caregivers and people with dementia who feel able to provide such narratives to shape local acute services in dementia.
Sometimes it feels as if ‘the world is not enough'; but, as start, awareness is not enough.