I remember once being told that an “alcoholic” is uomebody who drinks as much alcohol as you, but somebody you don’t particularly like.
Culture has an odd way of inflicting labels on people it doesn’t particularly respect. This can be done for entirely political reasons – a need to place a ‘them against us’ division, like the term ‘benefit scroungers’ for people who cannot find gainful employment.
I remember when I went to the Alzheimer’s Show last year, and a senior consultant in psychiatry gave a talk on ‘challenging behaviours and BPSD’. I challenged him at the end for whom did he deem the behaviour challenging – for the person with dementia distressed, or for the professional who wanted a quiet shift?
I then shortly afterwards went to an evening of a drug company sponsored CPD session on frailty. The GP presenting the case study kicked off with the line ’83 y.o. demented F’. I asked the presenter to justify the use of the word ‘demented’ in his case study. He informed me it was about as pejorative, and equally inoffensive, as saying ‘wheelchair user’.
I don’t want to enter into a discussion about normative morality. That is way beyond the scope of this blogpost. But there comes a time when you simply can’t cope with the deluge of cultural impropriety.
Two events happened back to back only yesterday. For example, a friend of mine, in an otherwise good article in a tabloid, was called ‘Dementia sufferer’ in the title. A press release about a forthcoming BBC programme on cures and dementia was littered with the word ‘sufferer’.
But I have recently been doing a lot of work in education of dementia, and it shocks me how entrenched the BPSD dogma is. I simply don’t want teaching I am involved in with to perpetuate knowingly this misfeasance.
‘Person-centred care’ is a much used and abused term. But dealing with failures in communication with a person who lives with dementia but who is distressed is a more ethical (and cheaper) way of behaving, other than pimping money out at Big Pharma.
An individual who’s received a diagnosis of dementia has a right to be angry, agitated, anxious or depressed at conscionable behaviour from a carer or professional, for example. An individual who’s received a diagnosis of dementia is therefore entitled to feel emotions if provoked.
What this situation does not give professionals a right to do is to drug innocent people with dementia always to prescribe antipsychotics inappropriately as a ‘chemical cosh‘.
In parallel to the human right to live with dignity, found in the European Convention of Human Rights which we can all petition over in England and Wales if we are a signatory, irrespective of the Human Rights Act (1999), there’s an expectation that patients of the NHS are not subject to assault and battery from inappropriate medications.
Whilst many of us are saddened by the lack of clarity in the current Government assaulting the legislation over human rights, we also take some comfort in devolution. Scotland is a clear example of an administrative style in one country. Manchester has been another. Maybe with the election of Sadiq Khan in London today we may have another example of a devolved infrastructure, which can distance itself from Westminster, and act as a nestbed for the integration of health and social care?
Be in no doubt – it takes a long time to alter the directions of supertankers. Dementia Alliance International has been campaigning hard on this for a few years now, and as the only influential international stakeholder group run by people with dementia, many of us wish them well.
It was a huge achievement for Prof Peter Mittler, human rights advisor to Dementia Alliance International, to get human rights firmly on the map last week. Dementia Alliance International is the main peak body for people with dementia, working closely, but autonomously, with the hugely influential Alzheimer’s Disease International.
We have to talk about the Dementia Alliance International. This is a group entirely of people who are ‘living beyond dementia’, in the phraseology of their leader Kate Swaffer, campaigning for the needs of people living with dementia.
This can mean that they are often highly sought after for their independent, yet massively influential, views. Prof Mittler CBE has a long and distinguished career in the intellectual disabilities, and now currently lives with dementia. Mittler was indeed one of the leaders who helped to establish the UN Convention on Rights for People with Disabilities.
Mittler’s voice is therefore an authentic and learned one. He has much experience in navigating through the maze that is the policy territory of international NGOs. It was therefore pretty predictable therefore that the resolution he worked on for Dementia Alliance International, with Neil Crowther, would be unanimously assumed by the Alzheimer’s Disease International. This means that rights-based advocacy has now been delegated to all the national dementia societies to implement at a local level.
I believe the way forward in ‘activism’ for human rights needs above all to have authenticity. People with dementia need to be leading from the front, taking charge of the campaign. This is a cardinal example of authentic leadership from the front being much more convincing than ’empowerment or engagement’.
This means that an approach based on slick presentations and booklets with relevant case studies, for the benefit for commissioners, will not be effective in embedding a rights-based consciousness for rights, akin to the racial civil rights movement of Martin Luther King or the democratic movement of Mahatma Gandi.
This means that glossy pitches, grants and Powerpoints in town halls will not be the defining factor for embedding a rights-based culture.
Where I think the town halls will be useful will be in building up a ‘guiding coalition’ of people with similar values, such as other groups which are at the forefront of equality and campaigning against discrimination – e.g. groups campaigning for race-related rights, or rights of people with intellectual disabilities.
But again, such a manner of campaigning solely through this formulaic approach would be highly naïve, bordering on disingenuous, here. Human rights are universal and inalienable – this means they can’t be easily siloed off according to which ‘protected characteristic’, e.g. sexual orientation, age, has been breached on any one particular occasion.
Take for example a right to health, or a right to independent living, under the current framework of global policy on sustainable communities. People with dementia often are not only living with dementia: ergo, policy and campaigning should not treat them as if they are only living with dementia, even if this is a useful corporate third sector construct.
We need to get away from the idea, running through English policy like letters in a stick of rock, that dementia is a condition to be gamed for the purposes of writing grants, for example in human rights.
Above all, people with dementia, not anyone else, must be leading the campaign on rights based advocacy.
Martin Luther King wasn’t white.
Mahatma Gandhi wasn’t from Slovenia.
A rights based advocacy approach for dementia in England can be achieved to a limited extent even if fronted by big charity and associated enterprises belatedly jumping on the bandwagon. But I don’t deny they also serve an important function in ‘playing the system’ – but this is not really what campaigning for rights is about. And they also have the big £££££.
Authentic organisations like Dementia Alliance International, going local, are the key.
The conundrum is quite literally this: Only people with dementia can do it, but they can’t do it alone?
There has been a disturbing tendency for the word ‘social movements’ to become bastardised for marketing a theme or even business product. I sympathise with people needing to pay their mortgages, but this approach has been to the detriment of real participation of those people whom Prof Edgar Cahn referred to as ‘no more throw away people’. Slick marketing, like pornography for the US Supreme Court, can indeed be spotted a mile off – you recognise it when you see it.
The word ‘co-production’ faces a similar setback. However, it is actually quite hard to escape what co-production really means, as defined below as an example.
“Co-production means delivering public services in an equal and reciprocal relationship between professionals, people using services, their families and their neighbours. Where activities are co-produced in this way, both services and neighbourhoods become far more effective agents of change.”
(Boyle et al., 2010).
Fake ‘involvement’ of patient groups I think does quite a lot of damage. This at one level is the notorious ‘zero sum gain’ – in that resources consumed A deprives resources for B. As an example, it would be dead easy for Big Charity to donate money to the Dementia Alliance International, a group run by and run for people living with dementia. But the fact this does not readily happen is an epiphenomenon entirely of the need of Big Charity to retain control as to who writes the script. Or put another way, who is in the room.
But secondly an illusion of control is deeply fraudulent in itself. The “illusion of control”, defined as various forms, is the tendency for people to overestimate their ability to control events; for example, it occurs when someone feels a sense of control over outcomes that they demonstrably do not influence.
You in an orchard, and you choose an apple which tastes delicious. You assume you are very skilled at choosing apples (when in fact the whole batch happens to be good today).
Another good example is that you enter the National Lottery and in fact you win millions. You assume that this is (partly) a result of how good your lucky numbers are. However, lotteries are totally random so you can’t influence them with the numbers you choose. Although most of us acknowledge this as a statement of fact rather than an opinion, we still harbour an inkling that maybe it does matter which numbers we choose).
Available evidence suggests that an important factor in development of this illusion is the personal involvement of participants who are trying to obtain the outcome (reviewed by Yarritu, Matute and Vadillo, 2014).
It is possible that pseudo involvement or pseudo engagement through regional working groups might be doing more damage than active democracy. I think a tell-tale sign of this is when in a double act of a person with dementia and a person without dementia the person without dementia does nearly 50% (or more) of the talking.
Another good example is where in ‘involving a person with dementia’, there is a “working group” chaired by, and the agenda set by, a person without a dementia. That person without dementia is in full control of the narrative.
This illusion of control has been discussed extensively elsewhere.
“Such involvement is frequently held up as empowering audiences and enhancing democracy. Indeed, the possibility of audiences creating their own content has led to the idea of reconceptualising traditional consumers as, in Jay Rosen’s now famous definition, ‘the people formerly known as the audience’. But what is being offered is a ‘simulacrum’ of engagement. The user is given the illusion of control – while all the time the underlying power relationships remain unchallenged. It has become commonplace to argue that policy-makers should act to ‘increase citizens’ participation in the commissioning and production of news in order to ensure that “the public interest” is no longer defined in private’ (for example Co-ordinating Committee for Media Reform 2012). How this might be achieved is less than clear and the belief that it will increase plurality may be ill-founded’.
(Scullion et al., 2013)
The traditional approach to the work on the “illusion of control” has been framed in motivational terms (e.g., Langer, 1975).
From this perspective, people’s judgments of control are influenced by subjective needs related with the maintenance and enhancement of the self-esteem (e.g., Heider, 1958). And as such it might be better to call involvement initiatives for what they also achieve – peer-support as well as boosting people’s self confidence in talking at public events.
It has been shown that the sense of having control has benefits for well-being (e.g., Bandura, 1989; Lefcourt, 1973).
As Bandura (1989) writes:
“They are full of impediments, failures, adversities, setbacks, frustrations, and inequities. People must have a robust sense of personal efficacy to sustain the perseverant effort needed to succeed. Self-doubts can set in quickly after some failures or reverses. The important matter is not that difficulties arouse self-doubt, which is a natural im- mediate reaction, but the speed of recovery of perceived self-efficacy from difficulties.”
This reflects a personal adage of mine – it’s not how you fall, it’s how you get up. And also makes complete sense – in that the invitation to go to events or conferences acts as a counterpoint to being given a diagnosis of dementia which has potentially a profound impact on identity.
Undeniably, one must set one’s sights way above “involvement”.
Promoted by the Scottish jurisdiction notably, a human “rights based approach” is about empowering people to know and claim their rights and increasing the ability and accountability of individuals and institutions who are responsible for respecting, protecting and fulfilling rights.
There are some underlying principles which are of fundamental importance in applying a human rights based approach in practice. These are the so-called PANEL principles.
participation
accountability
non-discrimination and equality
empowerment and
legality.
And these remain relevant too to the actual way care and support are approached.
“Everyone has the right to participate in decisions which affect their human rights. Participation must be active, free, meaningful and give attention to issues of accessibility, including access to information in a form and a language which can be understood.
In relation to the care of older people this means that individuals should participate in all decisions about the care and support they are receiving. This could range from participation in the commissioning and procurement of social care services by local authorities to participating in daily decisions about the care and support being received.”
Latterly, there has been such enormous arrogance that consistently people with dementia, if invited to conferences about dementia at all, are invited at the last minute giving all the semblance of an ‘after thought’ for marketing purposes.
One wonders why the named speakers in the programme are so reluctant to keep up a fuss, even those who have an involvement string to their bow.
Exclusion is no laughing matter parodies excepted.
But this sadly is not a joke. One year ago, Saudi Arabia hosted an all-male ‘women’s rights’ conference as reported here.
The article notes that:
“Saudi Arabia’s laughably prestigious University of Qassim played host to one of the biggest women’s rights conferences in the Arab world in 2012. Ironically, the institution managed to hold the event without the advice or attendance of a single woman.”
In the market which has developed in health and social care, it has been convenient to formalise the ‘invisible hand’ of Adam Smith into a broker. But questions about whether there is such a thing as a free broker, or whether fake involvement is seriously damaging to your genuine participation, must surely be asked. References
Bandura A. (1989). Human agency in social cognitive theory. American Psychologist, 44(9), 1175–1184. doi: 10.1037/0003-066X.44.9.1175.
Boyle, D, Coote, A, Sherwood, C, Slay, J. (2009) Right here, right now: Taking co-production into the mainstream. NEF/NESTA/The Lab.
Heider F. (1958). The psychology of interpersonal relation. New York, NY: Wiley.
Langer E. J. (1975). The illusion of control. Journal of Personality and Social Psychology, 32, 311–328. doi: 10.1037/0022-3514.32.2.311
Lefcourt H. M. (1973). The function of the illusions of control and freedom. American Psychologist, 28, 417–425. doi: 10.1037/h0034639.
Scullion, R, Gerodimos, R, Jackson, D, Lilleker, D. (2013) The Media, Political Participation and Empowerment. Routledge Publishers.
Yarritu I, Matute H, Vadillo MA. Illusion of control: the role of personal involvement. Exp Psychol. 2014 Jan 1;61(1):38-47. doi: 10.1027/1618-3169/a000225.
Late on Wednesday it was announced that the decision has been taken to admit Kate Swaffer to the World Dementia Council.
Kate Swaffer is Chair of Dementia Alliance International (“DAI”), which is a leading non-profit group of people with dementia from all around the world that seek to represent, support, and educate others living with the disease. DAI is an organisation that will provide a unified voice of strength, advocacy and support in the fight for individual autonomy and improved quality of life.
Kate, from Adelaide in South Australia, was diagnosed with semantic dementia – a form of fronto-temporal dementia – in 2008 at the age of 49.
Since getting her diagnosis Kate has become a campaigner, speaker and accomplished writer on dementia issues. In January 2016, her book ‘What the hell happened to my brain?” was published, and has rapidly become a landmark contribution of a detailed account of a lived experience with dementia.
Subsequent to my being diagnosed with younger onset dementia at the age of 49, health care professionals and service providers all told me the same thing: “to give up work, give up study and go home and live for the time I had left.” On the way, it was also suggested I put my end-of-life affairs in order – even though at no time was I told dementia is a terminal illness. I was also told to get acquainted with aged care, including selecting a respite day care and residential care facility, sooner rather than later, so I could become used to it. My husband was told he would soon have to give up work to become a full-time family carer.
Very quickly I termed this Prescribed Disengagement™, and thankfully I eventually chose to ignore it. Because Prescribed Disengagement™’ is a term I came up with, I was advised to trademark it before someone else did, and hence have done so.
Kate last year was awarded a distinction in her Master of Science in dementia care from the University of Wollongong.
The statement from the Dementia Alliance International reads as follows.
“Dementia Alliance International (DAI) Chair Kate Swaffer from Australia has today officially become a member of the World Dementia Council, the second person with dementia to join this council. This is an important and significant appointment for DAI, and for people with dementia globally. She joins another DAI member, who is also Vice Chair of the European Dementia Working Group, Hilary Doxford from the UK.”
Established by the last UK government, the World Dementia Council has the stated mission to champion dementia research and development and unlock investment around the world.
Kate’s admission to the World Dementia Council is a highly significant event.
DAI has been working towards full access for people with dementia to the United Nations Convention on the Rights of Persons with Disabilities (CRPD), which is a global tool for achieving social change, this second appointment is particularly significant. Article 19 of the Convention is the right to live independently and to be included in the community. Indeed, Prof Peter Mittler is due to be presenting on this, on behalf of DAI, at the Alzheimer’s International Conference in Hungary in April 2016.
Article 29 on “participation in public and political life” enshrines an obligation for State Parties “to persons with disabilities political rights and the opportunity to enjoy them on an equal basis with others, and shall undertake to ensure that persons with disabilities can effectively and fully participate in political and public life on an equal basis with others.”
The four major prongs of the World Dementia Council’s work currently are integrated development, “optimising the path of medicines from research through to market by reducing barriers & encouraging regulatory flexibility”; finance and incentives – “looking at ways to increase the relatively low investment in funding dementia innovation by exploring new types of funding product”; open science – “unleashing the potential of open science for sharing information and knowledge to accelerate progress in developing new treatments and care approaches”; and public health/prevention – “The Council is also beginning an evidence review into existing research on how risk factors such as diabetes and heart disease relate to dementia, as well as looking into public health messaging on lifestyle and prevention.”
Even with the development of new drugs to delay the progression of the dementias, the leading cause of which is Alzheimer’s disease in the world, the need for prevention of progression of diseases through both cognitive and non-cognitive therapies will be essential. Kate’s input as a person living with dementia and as an accomplished student of dementia herself will be unique.
Err… since this photo was taken in the Hotel Adina, opposite the conference centre hosting the Alzheimer’s Disease International (ADI) conference for 2014, I have lost a lot of weight (I wish.)
But actually literally seconds before this snap was taken, Kate had said ‘you goose!’ in utter surprise when I suggested to Kate she should turn her roaming charges off. We were, of course, both in Australia, and the country of habitual residence of Kate is also Australia.
I have many happy memories of that conference, though overall I tend to be antagonistic of conferences. Most of the plenary speakers tend to be overwhelmingly underwhelming.
There are of course some exceptional speakers. I always enjoy the updates on Prof Martin Prince on epidemiology of dementia, with a focus on low and middle income countries. I know this is a complicated area, as I am sure Prof Carol Brayne from my alma mater will demonstrate in Budapest for this year’s ADI conference.
Many of the pervasive issues internationally about living with dementia also relate very much to domestic jurisdictions: including research, drug therapies, timely diagnosis, care and support, enhancing health, and dying well.
Sometimes it can be all too easy to become an innocent pawn in massive corporate agendas, which sometimes tragically reveal themselves in slick ads from ‘big charity’, raising money, but pushing stigma of dementia to do so.
I first spoke with Kate over a rather greasy lamb moussaka. Beth was there. Beth and Kate took a mutual interest in what the restaurant had to offer.
I showed Kate the manuscript of my first book expecting her to be wholly uninterested in it: actually, the opposite was the case.
Kate’s background is not straightforward. A devoted mother and wife, haute cuisine chef (trained with the best people in this field), a distinction in dementia care from a world famous University, nurse specialist in operating theatres, volunteer in bereavement counselling, and, of course, keen international speaker on dementia.
I think Kate manages to update her blog every day, and has introduced an unique term called ‘living beyond dementia‘, which sums up a positive and flourishing approach – novel and original – setting aside the negative aspects of the impact of the medical profession in imparting a diagnosis.
Kate was the first person in the world to coin the term ‘prescribed disengagement‘ which was a huge impact in the field of dementia.
As Kate says, “This Prescribed Dis-engagement(TM) sets up a chain reaction of defeat and fear, which negatively impacts a person’s ability to be positive, resilient and proactive.”
“Dementia is the only disease or condition and the only terminal illness that I know of where patients are told to go home and give up their pre-diagnosis lives, rather than to ‘fight for their lives’.”
It is all too easy to become ageist about dementia, but it is the case that dementia encompasses conditions of the age which can affect people below the age of 65. Particular considerations for the so-called ‘young onset dementia’ might include how the diagnosis is arrived at, as well as subsequent impact on real lives such as family or employment.
I personally don’t think that academics can have the moral integrity to present the full picture, when what is truly valuable and a scarce commodity is the expertise and lived experience of people living with dementia.
I think it goes further than ‘working with not for’ in fact: it is more of a question of ‘who’s in the room’ at all. I think of the co-production imperative as ensuring there are ‘no more throw away people’ as per Prof Edgar Cahn. This, as Prof Peter Mittler reminded me recently, has a parallel in the inclusivity literature as ‘No one left behind’.
And above all – it is clear people having had a diagnosis of dementia feel great comfort from the experiences of other people in similar circumstances who have reconfigured their lives accordingly. Indeed this should be the analogous to how people with physical disability are given ‘reasonable adjustments’. Whilst reasonable adjustments is a rather legalistic clunky term, it is an aspect which has been seriously lacking in the drug-focused medical model of dementia.
Kate Swaffer, not just living with a dementia, has an important narrative to tell, which is continually evolving. It is totally unsurprising that her being Chair of Dementia Alliance International (DAI), an international stakeholder group for people with dementia, has been welcomed as a huge success by Alzheimer’s Disease International.
It always seems like a marathon not a sprint, and a long one at that. I thought it was unbelievably clumsy that the World Dementia Council, a steering group on world dementia work, did not have a single representative living with dementia currently.
I indeed wrote an open letter on October 13 2014, which is on the DAI website here. I was of course ecstatic when Hilary Doxford, a mutual friend and colleague, was appointed onto the WDC, as documented here.
Kate is a world-class advocate for people with dementia, and, take it from me, a force to be reckoned with.
I received this morning my copy of “What the hell happened to my brain?” written by leading international advocate in dementia, Kate Swaffer. This book is due to be released by Jessica Kingsley Publishers on January 21st 2016. I received an advance copy as I wrote one of the Forewords. The other Forewords have been written by Dr Richard Taylor Ph.D. and Glenn Rees AM Chair of Alzheimer’s Disease International.
Kate is Chair of Dementia Alliance International, the international stakeholder group run by people living with dementia. I feel this book will be incredibly useful for a diverse audience, including doctors – especially those completing specialist training in medicine (general medicine, neurology, psychiatry, surgery especially) – as well as members of the public newly diagnosed with dementia.
I know Kate Swaffer held Dr Richard Taylor Ph.D. in very high esteem. I found the chapter dedicated to him, and his Foreword, very moving.
This book is all about living ‘beyond a diagnosis of dementia” – Kate’s phraseology TM. Kate was the first to articulate and explain the phenomenon of ‘prescribed disengagement’ how people at the point of diagnosis are often put into a process of managed decline when they could be given opportunities for an enriched life. This of course goes together with essential practical help, such as things you can do such as driving. It also explodes myths out of the water – and ignites a provocative debate on the ‘big money’ in dementia, disability discrimination, an urgent need to rework the medical label of ‘challenging behaviours’, early vs late diagnosis, stigma, loneliness, inclusion, and guilt.
It’s not hyperbolic, nor puffery, to claim that you won’t be able to put this book down. It’s an outstanding book, and I strongly commend it to you.
Assessing risk is a critical part of English dementia policy at all levels. I again found myself talking about risk as I saw responses to World Alzheimer’s Day which was yesterday on September 22nd 2015.
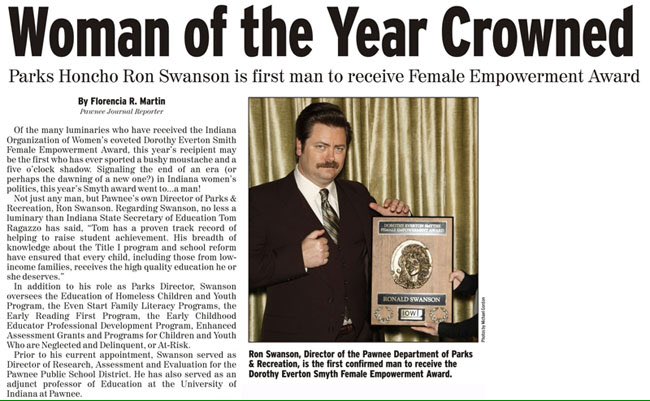
I don’t especially like the term ‘wandering’ for people with dementia. This term, like ‘challenging behaviours’ has become seemingly legitimised through the hundreds of papers on it in the scientific press, and the grants no doubt equivalent to hundreds of thousands of dollars probably. I think the term, intentionally or not, attributes blame. And as I moot in the tweet below, this is potentially a problem, especially one considers that a dementia charity should not ideally be fundraising out of sheer fear.
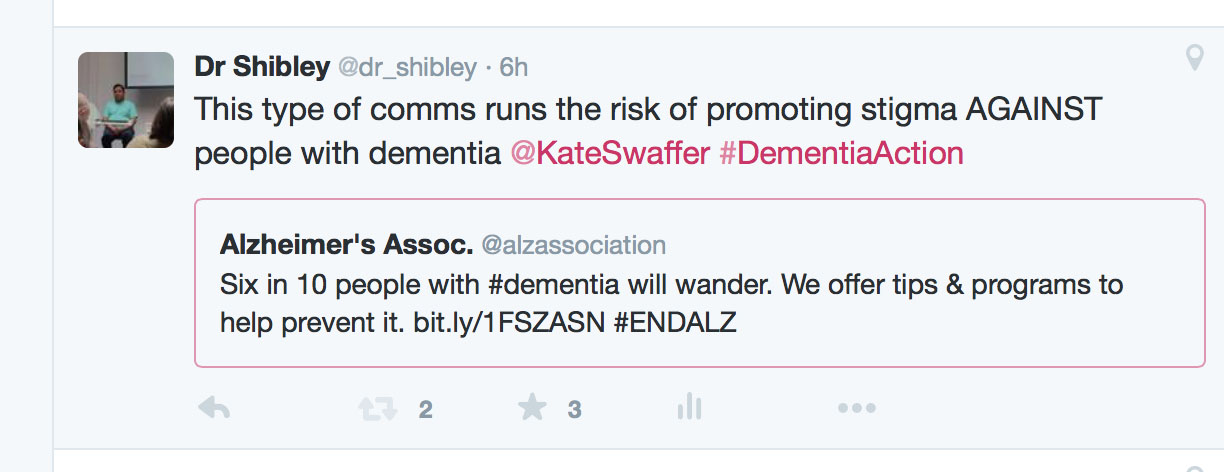
Don’t get me wrong. I think charities have an incredibly important part to play, and they do, in educating people about dementia; and generally ‘raising awareness’ howeverso defined. Take for example this helpful tweet from the Alzheimer’s Disease International containing a relevant infographic about the scale of the dementia epidemiology.
I had a hunch that something was very awry about yesterday when my colleague Simon Denegri tweeted something which caught my eye. Let me introduce you to Simon. He’s Chair, INVOLVE, NIHR National Director for Patients and the Public in Research, and, importantly, a nice guy.
The tweet, and the main subject of the research, is pretty self explanatory in fact.
The point Simon raises is worth thinking about, I feel. Is updating the epidemiology of dementia every year, nay every month, or even every week, an effective way of genuinely raising public awareness – or is it rather a lazy way to campaign on it? Obviously, playing devil’s advocate, one should argue that this main issue should be raised until something happens, but with a cure for dementia a long way distant it seems that this option is not likely.
So how about offering some solution instead? In other words, having scoped the problem, why not offer hope instead of fear through the huge volume of research in improving quality of life for people living with dementia and carers. Here’s the thing: there are 850,000 people living with dementia at the moment currently, and there’s got to be something in it for them with all this coverage.
I call fixating on the ‘tsunami’, ‘time bomb’ or ‘tidal wave’ “the shock doctrine” to make you want to dig into your deep pockets, to make you donate to a dementia charity. BUT – with social care funding on its knees, having not been ringfenced since 2010 – is this actually a luxurious response to a rather serious immediate problem? Long before #DementiaWords ‘got sexy’, I presented my poster (PO124) on the hyperbolic language used in the G8dementia proceedings, in the Alzheimer Europe 2014 conference.
Here’s the rub.
Jeremy Hughes and the Alzheimer’s Society have been hugely successful with the ‘Dementia Friends’ campaign, which has seen a roll-out of information sessions on the basics of dementia for the whole country. Yesterday was a good opportunity to talk about that.
But meanwhile Alzheimer’s Research UK, which indeed does formidable work for the research infrastructure on dementias in the UK, rolled out this in a blogpost yesterday. The phraseology of the remark, “At Alzheimer’s Research UK, our hope is for a different kind of future, one where future generations will be free of this life-shattering condition”, is the opposite to one of the central messages of Dementia Friends, that ‘it is possible to live well with dementia’.
I don’t, of course, want to downplay the huge significance of the disclosure of the diagnosis of dementia as a life event for all those involved, not least the direct recipient of that diagnosis.
All of this leads to me wonder who exactly is protecting whom? I wouldn’t go so far as to say that the public needs protecting from large dementia charities, but the sway they hold on policy is not inconsiderable; whether this is on the cure v care resource allocation in dementia, or whether there should be specialist nurses as well as dementia advisors (as I argued this year both in the ADI and Alzheimer Europe conferences).
There’s no doubt, as regards safeguarding issues, that people with dementia need to protected from risk where it is proportionate to do so. As I have long argued, you need to embrace risk to live well with dementia. But it is worth thinking about on whose part we are negotiating risk? Damian Murphy’s excellent blogpost yesterday emphasises how we cannot necessarily assume that carers and persons with dementia have the same (or even similar) viewpoints: this is directly relevant, say, on whether a person with dementia with a carer gets a GPS tracking device? (I duly anticipate and expect Damian’s contribution here, by the way, to be seminal one, by the way.)
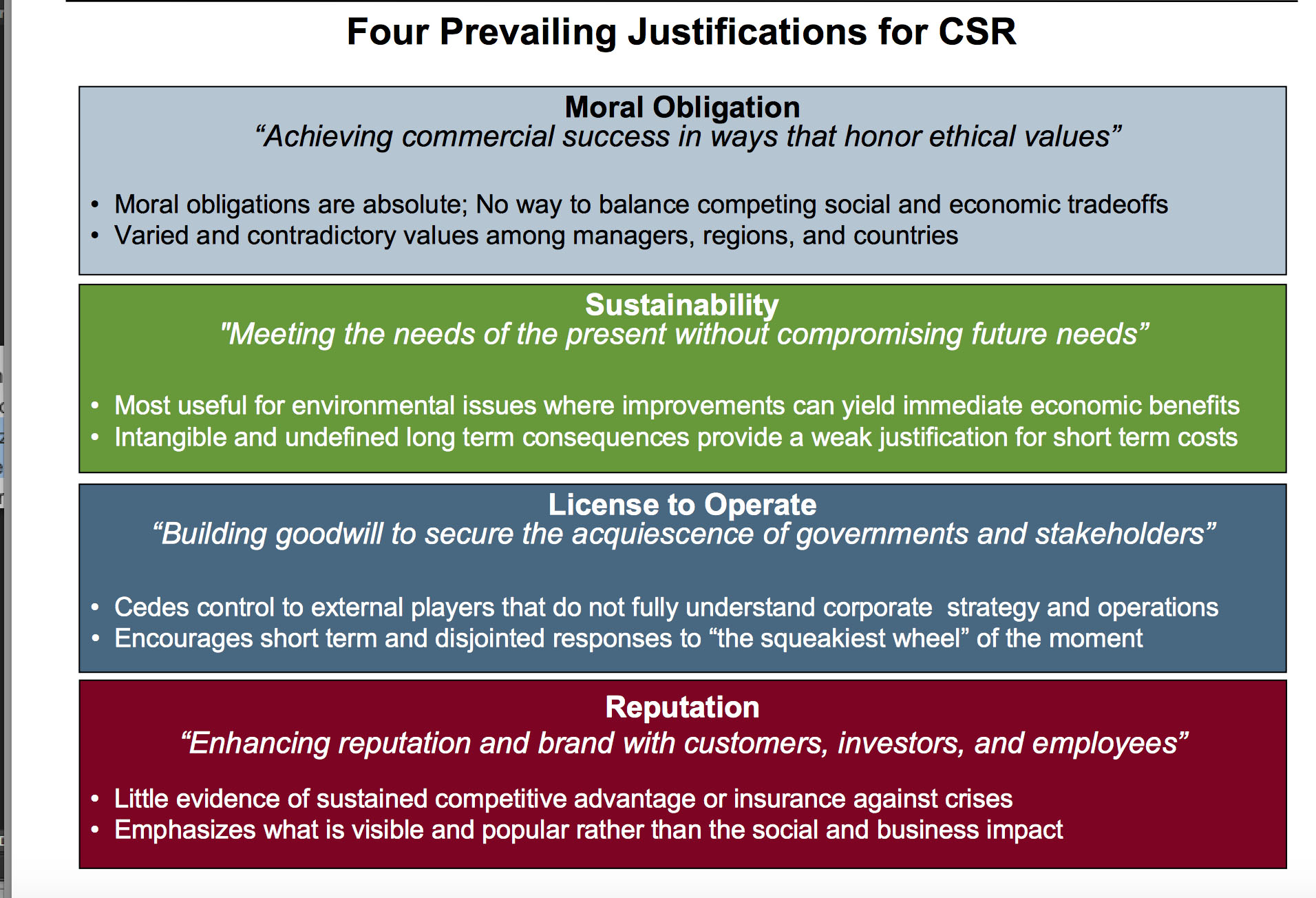
A long time ago when I was reading some of the management literature, I was really impressed by a paper to which Prof Michael Porter contributed on strategy and society (co-author Mark Kramer) in the Harvard Business Review.
Mark in a slide once summarised four crucial tenets of observing this re-articulated corporate social responsibility thus.
I, for one, would like to see all campaigning done by the dementia charities seen through this prism; and also bearing in mind the clinical, if not societal, question cui bono?
There is no doubt the ‘World Dementia Council’ (WDC) is a very good thing. It contains some very strong people in global dementia policy, and will be a real ‘force for change’, I feel. But recently the Dementia Alliance International (DAI) have voiced concerns about lack of representation of people with dementia on the WDC itself. You can follow progress of this here. I totally support the DAI over their concerns for the reasons given below.
“Change” can be a very politically sensitive issue. I remember going to a meeting recently where Prof. Terence Stephenson, later to become the Chair of the General Medical Council, urged the audience that it was better to change things from within rather than to try to effect change by hectoring from the outside.
Benjamin Franklin is widely quoted as saying that the only certainties are death and taxes. I am looking forward to seeing ‘The Cherry Orchard” which will run at the Young Vic from 10 October 2014. Of course, I did six months of studying it like all good diligent students for my own MBA.
I really sympathise with the talented leaders on the World Dementia Council, but I strongly feel that global policy in dementia needs to acknowledge people living with dementia as equals. This can be lost even in the well meant phrase ‘dementia friendly communities’.
Change can be intimidating, as it challenges “vested interests”. Both the left and right abhor vested interests, but they also have a strong dislike for abuse of power.
I don’t mean simply ‘involving’ people with dementia in some namby pamby way, say circulating a report from people with dementia, at meetings, or enveloping them in flowery language of them being part of ‘networks’. Incredibly, there is no leader from a group of caregivers in dementia; there are probably about one million unpaid caregivers in dementia in the UK alone, and the current direction of travel for the UK is ultimately to involve caregivers in the development of personalised care plans. It might be mooted that no one person living with dementia can ever be a ‘representative’ of people living with dementia; but none of the people currently on the panel are individually sole representatives either.
Roger was keen to emphasise to me that you must listen to the views of people with dementia in developing innovations. He has written at length about the implementation of ‘user groups’ in the development of designs for assistive technologies. Here’s one of his papers.
My Twitter timeline is full of missives about or from ‘patient leaders’. I feel one can split hairs about what a ‘person’ is and what a ‘patient’ is, and ‘person-centred care’ is fundamentally different to ‘patient-centred care’. I am hoping to meet Helga Rohra next week at the Alzheimer’s Europe conference in Glasgow; Helga is someone I’ve respected for ages, not least in her rôle at the Chair of the European Persons with Dementia group.
I really do wish the World Dementia Council well. But, likewise, I strongly feel that not having a leader from the community of people living with dementia or from a large body of caregivers for dementia on that World Dementia Council is a basic failure of democratic representation, sending out a dire signal about inclusivity, equality and diversity; but it is also not in the interests of development of good innovations from either research or commercial application perspectives. And we know, as well, it is a massive PR fail on the part of the people promoting the World Dementia Council.
I have written an open letter to the World Dementia Council which you can view here: Open letter to WDC.
I am hopeful that the World Dementia Council will respond constructively to our concerns in due course. And I strongly recommend you read the recent blogposts on the Dementia Alliance International website here.
Sue Stephen, one of the founding members of the Dementia Alliance International (DAI), spoke about how she came to be diagnosed with PCA.
This is one of the latest additions on their blog, which I strongly recommend. The DAI is an unique group of individuals with a strong sense of solidarity, who live with one of the various types of dementia.
“I had been noticing myself for the last few years that I was having visual issues… very bad glaring.. when I tried to read..”
She put it down to stress, but she still went ‘to get [my] eyes tested.’
And this went on for a few years. Interestingly, she reports this delay in diagnosisas rather typical for many people finding a diagnosis of PCA.
Tests for dementia of the Alzheimer type, typically initially shown up by problems in short term learning and memory, were negative.
When she was eventually given a diagnosis, she was told, “That’s it. There’s nothing I can do. Here’s a prescription for Aricept. See you in six months.”
But she described being shocked, and she had no idea what PCA is/was.
“I lost all certainty in my life. How do I make decisions in my life?”
She then sat on her month doing ‘research’, but reported ‘three wonderful things’ which came out of her research.
She found a list of symptoms which matched what she had been experiencing. “That was really good”. This enabled her to see her GP who then went referred her onto more suitable specific tests, confirming the diagnosis.
That’s one of the slight paradoxes about the way we approach a fellow citizen of ours living with a dementia. Nobody wants to be defined by any medical conditions they live with. They do not wish (rightly) to consider themselves as a collection of diagnoses.
But it is often reported by people living with conditions how it can be both a blessing to know what might happen but also a burden to know something might happen, with this information resulting from a clinical diagnosis.
She then reported discovering the work of Sir Terry Pratchett, who is living well with PCA, still writing books.
A third thing which she reports is finding a group of people on Facebook of people with posterior cortical atrophy. It’s a closed group where people can share in private “scenarios”.
“I could see in the future what symptoms might be. I look at symptoms, and I think if this happened to me, what could I do now to help?”
Stephen reports sharing these stories really helped.
Terry Pratchett went to see other people living with posterior cortical atrophy in 2010, a form of dementia.
Pratchett is an example of an individual who has shown that it is possible to live well with dementia.
Pratchett admitted he was apprehensive about the meeting, as he said it was like ‘seeing into the future’.
One person in the meeting, “Anything coming through the postbox, I can’t read. Susan has to do everything from cutting my nails to putting my shoes on. This disease.. or whatever you call it, changes your perspective.”
“It didn’t happen – it evolved.”
Pratchett though admitted despite his fears he enjoyed the meeting.
“I can see why people enjoy meeting up”
He had dinner with Graham Doggett, who is an 70 year-old author, and academic who has written books about quantum chemistry, and his wife.
“Susan is the gardener. If I help her, I can never find the wretched branches in the air to prune. They disappear.”
“I was doing computing since 1959. That’s gone.”
“I used to play piano up to grade 7. Gone.”
“Reading, writing, gone gone”.
When the term ‘living well with dementia’, one of the main disclaimers on that is that the person living with one of the dementias will have their life before to compare their experience to.
And this is bound to impact upon one’s own personal perception of living with dementia. Unless you bother to find out about the past of a person, in relation to his environment, you will not be able to understand his or her world.
The symptoms of PCA can vary from one person to the next and can change as the condition progresses.
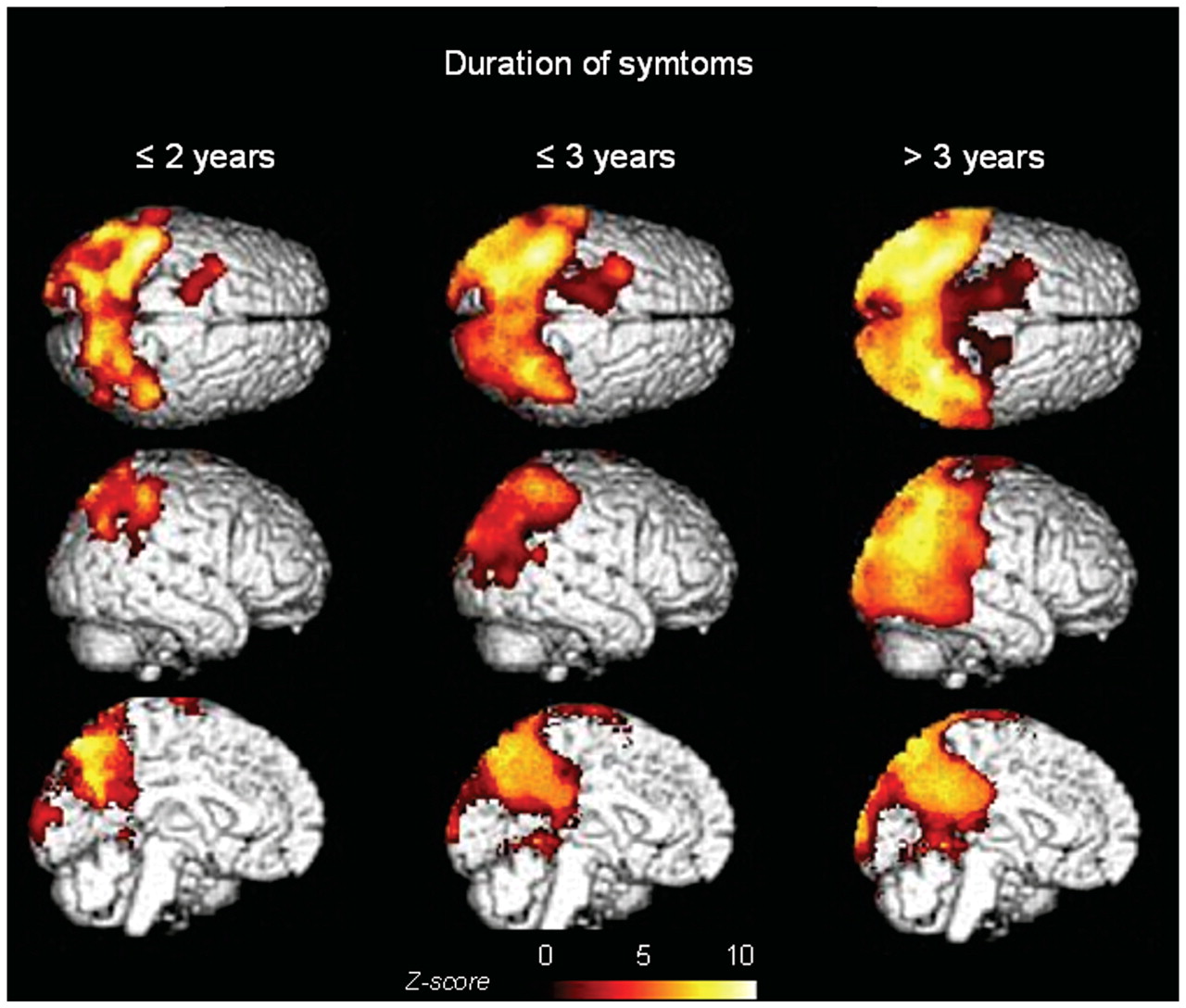
The most common symptoms are consistent with damage to the part of the brain at the back of the head, an area responsible for processing visual information.
Consistent with this process are slowly developing difficulties illustrating its slow and progressive nature due to a disease of the brain.
Now you’re even able to follow it using sophisticated ‘imaging’ of the brain.
These difficulties include visual tasks such as reading a line of text, judging distances, and distinguishing between moving objects and stationary objects.
Other symptoms include an inability to perceive more than one object at a time, disorientation, and difficulty maoneuvering, identifying, and using tools or common objects.
Some people can experience hallucinations.
Yet further symptoms can include difficulty performing mathematical calculations or spelling, and many people with PCA experience anxiety, possibly because they know something is wrong.
In the early stages of PCA, most people do not have markedly reduced memory, but memory can be affected in later stages.
This illustrates how this particular dementia is not just about memory.
Both Stephen and Pratchett demonstrate by a country mile while there are more to people than their dementias.
If you’d like to find more about dementia, you can do a short 45 minute session close to where you live in England (and now in other parts of the UK). The initiative is run by the Alzheimer’s Society, but is a Public Health England initiative. To find out more about this initiative called “Dementia Friends”, please go to their website.
There’s more to this initiative than the badge you’ll receive in the process, but this initiative is all about improving understanding in the general population about the dementias. I hope you will wish to learn more.
People with PCA are are at risk of being let down by ‘traditional dementia support groups’.
That is partly because they are younger and face different challenges, and partly because the activities offered in day centres puzzles, large-font books—are visual and thus actively unhelpful for people with PCA.
PCA is not new to the research community.
Already in 1902, the Czech psychiatrist Arnold Pick mentioned a woman’s inability to see and grab a lit candle held in front of her face in his essay “Ueber eine eigenthuemliche sehstoerung senile dementer,” Jahrbuecher f. Psychiatrie u. Neurol., see excerpt.
Several attempts at defining criteria for diagnosis exist.
The neurologist Frank Benson at the University of California, Los Angeles, coined the term while describing the pattern of symptoms in five patients (Benson et al., 1988).
Later, Mario Mendez, also of University of California and San Francisco proposed clinical diagnostic criteria arguing that PCA is its own syndrome, not simply Alzheimer’s disease with visual symptoms (Mendez et al., 2002).
The English dementia strategy is mindful of the needs to develop communities supportive of the needs of people living with PCA, of the need for high quality research research into PCA, and to think how people living with PCA can be best supported professionally and personally.
It’s not only people with posterior cortical atrophy who experience problems with vision, however. This is very important to be aware of.
“Or when we shouldn’t be put in a freezer, when we our caregivers go on holiday. We too should take a vacation from our caregivers.. enjoy the company of other people with dementia and enjoy their company.”
Dr Taylor had explained how there is a feeling of camaraderie when people living with dementia meet in the room. This is somewhat different from an approach of people without dementia being ‘friendly’ to people with dementia, assuming of course that you can identify reliably who the people with dementia are.
We are now more than half way though ‘Dementia Awareness Week’, from May 18 – 24 2014. Stigma, why society treats people with dementia as somehow ‘inferior’ and not worth mixing with, was a core part of Dr Taylor’s speech recently at the Alzheimer’s Disease International conference held this year in Puerto Rico.
He has ‘been going around for the last ten years, … talking to people living with dementia, and listening to them.”
That’s a common ‘complaint’ of people living with dementia: other people hear them, but they don’t listen.
“Stigma defines who we are.. not confined to the misinformed media, or the ‘dementia bigots’. Stigma is within all of us. When I heard my diagnosis, I cried for weeks… I’d never heard of dementia or Alzheimer’s disease, but it was the stigma inside me.”
Commenting a new vogue in dementia care, which indeed I have written about in my first book on living well with dementia, Taylor remarks: “We’ve now shifted to ‘person-centred care’. I think that’s a good idea. I always ask the caregiver who that person was centred was on previously. But I do that because I know I can a bit of a smart-arse”
“The stigma is in the very minds of people who treat us.”
“But you actually believe we are fading away… and we are not all there… it is not to our benefit.”
“The use of stigmas to raise awareness must stop right now.”
” Very little attention is paid to humanity of people living with dementia.. The use of stigma to raise awareness and political support must stop. We must stop commercials with old people.. which end with an appeal for funds. That reinforces the stigma. That comes out of focus groups with a bunch of people they want to focus on.”
“What would make you give money to our organisation? An older person or a younger person… We had a contest in the United States of who should represent “dementia”. The lady who won was 87-year old man staring into the abyss with a caregiver with a hand on her shoulder…”
“Telling everybody with dementia that they’re going to die is a half-truth. The other half without dementia are going to die too. Making it sounds as if people are going to die tomorrow scares the life out of people… scares the money out of people.”
But it seems even the facts about dying appear to have got mixed up in this jurisdiction. Take for example one representation of the Alzheimer’s Society successful Dementia Awareness Week ‘1 in 3 campaign’.
Neither “Dementia Friends” nor “Dementia Awareness Week” can be accused, by any stretch of the imagination, of ‘capitalising on people’s fears”.
And the discomfort by some felt by speaking with some sectors of the population is a theme worthy of debate by the main charities.
Take this for example contemporaneous campaign by Scope.
But back to Richard Taylor.
“How are you going to spend the rest of your lives? Worrying about how you’re going to die, or dying how you’re going to live?”
“I believe there is an ulterior motive.. to appeal to our fear of dying.”
“Stop using the fear of us dying to motivate people to donate to your organisations. It makes us mad and complicates our lives more than it needs to be.”
“The corruption of words to describe people who live with dementia and who live with us must stop.”
Dr Richard Taylor argues that the charities which have worked out how best to use manipulative language are the dementia charities.
“The very people who should be stopping corruption in language are the very ones involved in… “We’re going to cure dementia” What does that mean? Or will it be a vaccine where none of you get it and we all die, and so there’s no dementia any more?”
Taylor then argues you will not find ‘psychosocial research’, on how to improve the life of people with dementia.
“We are heading for more cures.. we’ve set the date for it wthout defining it. If we’re going to cure it by 2025, what will I see in 2018 to know we’re on track? .. It’s corrupt language.. None of the politicians will be around.. But people with dementia will be around to be disappointed.”
Taylor notes that every article rounds off with: “And now with further investigation, there’s a hope this might do this and this might do that.”
Except the politicians and charities have learnt how to play the system. These days, in the mission of raising awareness’, a Public Health and Alzheimer’s Society project, many articles focus on ‘Dementia Friends’, and people can decide at some later date whether they want to support the Alzheimer’s Society.
They could as a long shot decide to support Alzheimer’s BRACE, or Dementia UK. Dementia UK have been trying desperately hard to raise awareness of their specialist nursing scheme, called “Admiral Nurses“.
It all begs the question is the focus of the current Government to promote dementia, or to promote the Alzheimer’s Society?
Take this tweeting missive from Jeremy Hunt, the current Secretary of State for Health in the UK:
According to Taylor, “We need to start helping for the present.”
He is certainly not alone in his views. Here’s Janet Pitts, Co-Chair of the Dementia Alliance International, who has been diagnosed with frontotemporal dementia. Janet is also keen on ‘person centred services’, ‘is very proud of the work [we] have been doing since [our] inception in June 2013′, and is an advocate.
“I am an example of where life is taken away, but where life is given back… [I want us to] live well with dementia, advocate for people with dementia, reduce stigma in dementia.”