Previously, there had been a nihilistic view that ‘nothing can be done’ once a diagnosis of dementia is imparted. It is now clear that dementia rightly deserves a place alongside other long term conditions; and where it is appropriate to consider it under a ‘social model of disability’ so that full rehabilitation can be approached.
There have been various versions of this concept including “dementia capable”. At first blush, such an approach might seem too simplistic, given the vast cultural and ethnic variations. However, there is now an accreditation scheme which establishes a specification, and the elements you would expect, i.e. community-based sustainable solutions to combat stigma, are all there. This builds on a long line of work in England, and can be nicely compared with approaches in other jurisdictions such as Australia and Japan.
There have been a number of staging posts in English policy which have given this policy a firm footing, not least the Prime Minister’s Dementia Challenge. It is clear, however, that such initiatives only have substainability and moral integrity if they have the full backing of stakeholder groups for people with dementia, such as the Dementia Alliance International or the European Working Group for People with Dementia. Such groups are been pivotal themselves in combatting stigma, for example in the scrutiny of language. Other international groups, such as WHO and the Alzheimer’s Disease International, have also been massively influential.
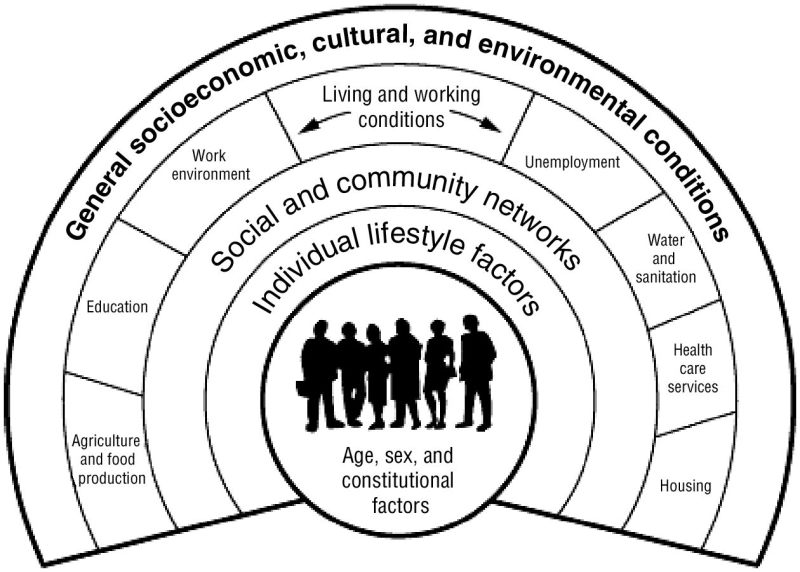
In England, “Dementia Friends” is an example of a social movement which was intended to provide a basic level of education about dementia. And this acts as a useful background to other ‘elements’ of the “dementia friendly jigsaw”, such as dementia friendly cities, dementia friendly design, or dementia friendly hospitals. “Dementia friendliness”, nonetheless can be considered at a number of different levels, such as securing a better customer experience in shops for people with dementia, or greater consciousness over legal ‘rights’ such as employment or human rights. The wider social determinants of health are clearly important in providing the theoretical underpinning of promoting wellbeing, such as housing, education, transport and leisure; and are, unsurprisingly, key components of any proposed system for promoting living better with dementia.
Whilst the exact term ‘dementia friendly’ may not be right, and many agree on that, a sense of accessibility and inclusivity is deeply desirable. Progress on this policy has to go beyond marketing, and research funds must not neglect this area of policy or service provision. This talk will, however, emphasise that a huge amount has been achieved in a relatively short space of time.
Chris Roberts, who was diagnosed with mixed vascular and Alzheimer’s dementia in his late 40s, made a very focused comment yesterday in conversation with Angela Rippon at the annual Alzheimer’s Show in London.
Chris argued that we can all ‘be aware’, but “awareness is very different from education”.
Coincidentally, I had been privately been discussing with Angela Rippon before the session how struck I am that people around the world found the Dementia Friends programme groundbreaking.
I am extremely proud to be a ‘Dementia Friends Champion’ in England. I run ‘Dementia Friends’ sessions for the general public to the best of my ability, and the programme, an initiative from the Alzheimer’s Society and Public Health England, is good fun to be involved with, for me.
There’ve been various attempts at raising awareness about dementia, some with varying degrees of success. I remember judging one abstract for the Alzheimer’s Disease International conference we’ve just had in April 2015, where one group had released some purple balloons in a town scale.
This reminds me of the famous Lynton Crosby strategy of the “dead cat”.
As Boris Johnson MP describes about this strategy, “”The key point, says my Australian friend, is that everyone will shout ‘Jeez, mate, there’s a dead cat on the table!'; in other words they will be talking about the dead cat, the thing you want them to talk about, and they will not be talking about the issue that has been causing you so much grief.”
According to Health Minister Rona Ambrose said the goal is to reduce stigma, “so that when (people with dementia) go to the bank or the corner store, people understand to be a little more patient.”
Watch the promotional video for yourself.
Charities have a long track record of being engaging professional advertising agencies to get their message across. Here in England, it was reported that, “PHE will invest up to £4 million a year until 2014/15 and expects significant additional funding from partnership marketing. “The scale of the challenge demands far greater ubiquity than we alone can fund,” a PHE spokeswoman said.”
The allocation of scarce resources in itself is an important policy question, in the light of cuts in social care, and accusations of a relatively impoverished infrastructure of dementia advisors, dementia support workers and clinical specialist nurses including Admiral nurses.
The presenter of the Canadian video walks into a darkly lit theatre, in keeping with the usual ‘shock doctrine’ tactics which are quite common in such pitches.
The presenter then says, “It’s repeating the same word or phrase. It’s repeating the same word or phrase. It’s repeating the same…”
But this is problematic territory, as the lines are presented as if to be ‘mildly amusing’. When this approach was last used at the Sunday Night at the Palladium, in a more extreme version, it went down like a lead balloon.
A comic there said: “I think I am losing my memory. Do you ever think you have Alzheimer’s? Do you do that thing when you walk into a room and go ‘what did I come into this room for?’ Open up a fridge, and go into soft focus. And close the fridge and go ‘what did I open the fridge for?’ Driving my car and thinking where am I going. I was looking for something in the fridge.”
And, after a few minutes, the comic added: “Have I done the Alzheimer’s joke?”
Two of the symptoms he presents are symptoms which could be reasonably expected in people with Alzheimer’s disease, the most common form of dementia globally, presenting in the majority with problems with learning and memory. These symptoms are word finding difficulties, or not knowing where you are.
But other symptoms include “not being dressed for the weather”, “pacing up and down”, or “even using expletives such as “shit”, according to the presenter”. These symptoms are certainly not common at all for people living with any type of dementia early on.
I have had many thousands of conversations with people living with dementia, and use of profanity by either party has been negligible.
Sometimes some persons with the behavioural variant of frontotemporal dementia can be disinhibited; so in cognitive testing you would occasionally get the reply ‘sun, sea, sex, sangria, suspenders’ when asking someone to name as many words as possible beginning with S. This has been reported elsewhere.
But the interesting aspect of this for me is how certain people with dementia can perform very well on this test known as “verbal fluency”, often at a superior level to people without dementia.
Helga Rohra, pioneer advocate as Chair of the European Persons with Dementia, herself living with dementia, refers specifically to the “faces of dementia”, rather than the ‘stages’ of dementia.
But this episode with the Canadian video shows that there can be a wrong type of education. The presenter then remarks on the need to know about dementia, hence the campaign of ‘Dementia Friends’ in Canada from the Alzheimer Society of Canada.
I am not particularly ‘angry’ that this has happened. It’s obvious to me that this initiative from Canada must be strongly supported by people wishing to break down stigma and discrimination towards our fellow citizens with dementia around the world.
I am a bit disappointed that all of this could have been easily avoided simply by involving a ‘focus group’ of people living with dementia at all stages of development of this project; and possibly this film is a result of a vague instruction to a marketing agency.
But I feel that it would be worth thinking about tweaking the video in subsequent revisions of the promotion of this programme, to provide a more accurate representation of dementia.
Rather than fostering mutualism, Liz Kendall is at risk of producing a policy void through nihilism. Just like pets are not just for christmas, entitlements are not just for employees. A look at the reform of public services, as Liz has done brilliantly, is especially to the English dementia policy debate, and as such it’s hard to argue against ‘quality, flexibility and choice’ per se.
But take the example of people sitting in chairs with the TV blairing out and a noisy hoover on in a care home. These residents of the care home probably can’t be said to have choice over their local environment, and this is clearly not ‘good care’ whoever provides it. If the same situation were on an acute hospital ward in the NHS, it wouldn’t be great either.
Perhaps the dichotomy between ‘left’ and ‘right’ is a false one in politics, in that both private businesses and state services would possibly agree it’s hard to provide the best services on an inadequate budget. But this is important for personal-held budgets too. And choice is somewhat illusory, if the service is essentially the same, for example treatment of a leg ulcer using evidence-based antibiotics on a NHS hospital ward or private nursing home.
I would like to feel that ‘self help’ is a political shorthand. Overall, the policy ambition that people can know about their own health and wellbeing through appropriate information, have some control or choice over their management, might be able to avoid hospital admission through anticipatory personal care planning, all makes intuitive sense to many.
The reality does deserve thinking about anyway. Many are essentially pumping the line still that there is no alternative, and indeed there might not be an alternative if an English government advocates reading lips and no more taxes until 2020. Labour deputy hopeful Rushanara Ali MP managed somehow to ramrod the word ‘competition’ in an answer on devolution on BBC Any Questions on Friday, but competition has not always necessarily helped.
What we really wanted, and we are finally getting from the care regulators, led by the Care Quality Commission, is the sharing of good practice. Too often any good practice has found itself isolated and not publicised. Sharing of information is essential not only for breaking down silos in care, such as health, mental or social, but also from a practical point of view in effecting safeguarding, for example.
But a race to the bottom as to who can offer lowest taxes is clearly not the solution if it translates into who can offer the worst public services. Something’s gotta give. And, even if you do subscribe to some identity of the left, it must be a concern if the left does not encourage peer support networks, or enable professional relationships, whether that may be a dementia advisor, dementia support worker, or clinical specialist nurse such as an Admiral nurse.
Self help is not necessarily THE solution if expertise is required to anticipate low bone density due to a mélange of risk factors which might predispose someone to a fall at home, such as poor diet or low sunlight. It cannot be the solution if people with dementia, and closest ones including family caregivers, aren’t given guidance on coping strategies. The demands of carers are huge. Many of us would not wish to call these cumulating in a ‘burden’, somewhat detracting from the value of carers, but the health and wellbeing of the carer can directly impact upon the health and wellbeing of a person with dementia.
If we have problems in assessing ‘quality’ in public services (and we do), we are likely to have problems in assessing quality in self-care. No doubt there can be clever algorithms in ‘activation’ of self care, but many still feel themselves relatively undertrained in self-carer. Many unpaid family carers do not indeed think themselves as ‘carers’, despite knowing full well their enormous care commitments, and feel that they have been plunged into the deep end into a rôle they didn’t particularly anticipate at their time of life.
One of the most potent criticisms of the ‘Big Society’ was that in fact it was a cover ‘for cutting the State’ – and we can see how this might have arisen as the timing of the Big Society was virtually simultaneous as the Cameron-push for austerity in light of the global financial crash. But likewise, there’s a lot to commend in self-care, which is at risk of being toxified by continued cuts in public services.
Public services, even if outsourced, tend to be reluctant in assessment of ‘continued performance’, and yet this takes time and resources. Giving a person with dementia or a proxy a budget, and expecting him/her just ‘to get on with it’, cannot be the solution. But relationships-centred care is where much thrust rightly is being placed in English dementia policy, showcasing integrated person-centred approaches (and we can argue for a long time on the exact meaning of this).
But I feel that ‘self help’, while a well intended shorthand, is perhaps missing a big problem identified by Phillip Blond. That individualism can be promoted by converting a contract with a large provider (be it public or private, e.g. one of the private oligopolies) into lots of social contracts with other stakeholders. Not all “positive” choice is exerted through a budget or market economics, and the sooner politicians of all purported shades realise this, the better?
Thanks to Nigel Ward for organising this year’s programme, and to my co-presenters Marion and Maggie who presented their books on personal life experiences of caring in dementia. I strongly commend these books to you; “Have you seen my daughter?” and “The Gift of Alzheimer’s“.
A recording of my talk is provided here. Thanks to Gary Marsh (@mistersquash) for recording it on an iPad; please note that the concourse of the exhibition is very noisy, so there is inenvitably a lot of background noise despite the excellent sound system.
I greatly admire Angela Rippon for promoting policy issues in dementia, but especially in inter-generational education of living with dementia.
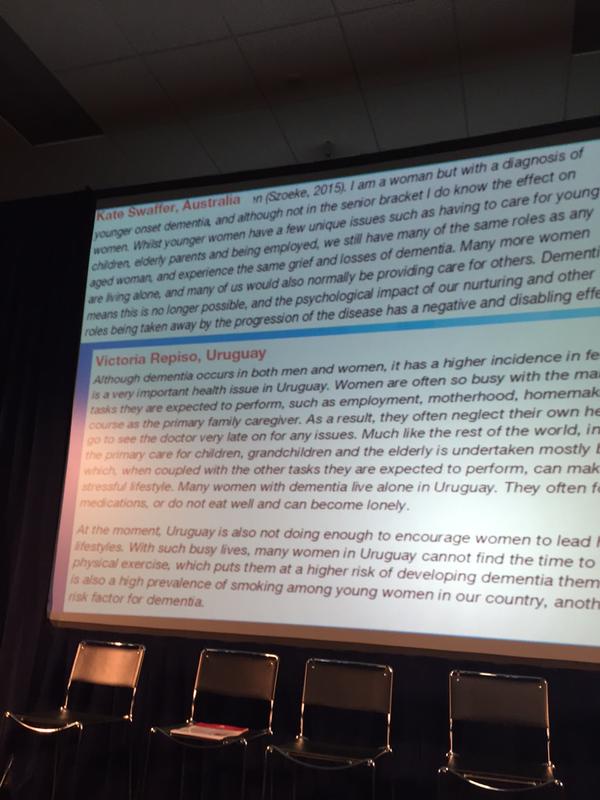
This of course is a key policy plank in England and around the world; like ‘women and dementia’ (the 2015 report on this from Alzheimer’s Disease International was launched at the Alzheimer’s Show yesterday.)
Prelude
Any individual’s wellbeing is more than their interaction with health and care systems. Wellbeing is not simply an absence of ill being, and many factors are known to determine one’s health in the social strata such as housing and transport.
Many phenomena are not just physical buildings, such as hospices or care homes, and it is now being increasingly recognised that they act as community hubs in the wider community. It’s become ‘acceptable’ to celebrate very good care, and is in fact now being strongly encouraged in national policy to promote good practice. All too often boundaries can get established, creating distinct silos; sharing is “king”, but secrecy can be fatal. Even regulators are taking on the mantle of trying to advance promote good care, as well as identifying when things have gone wrong.
It’s easy to unappreciate the potency of a number of different separate strands which have converged on the potential of ‘living better with dementia’. These include, for example, developments in the law, such as safeguarding under the Care Act to mitigate against neglect and abuse, initiatives to encourage ‘integrated care’ such as the ‘Better Care Fund’, the recent public health initiatives to increase knowledge about dementia in the public (“Dementia Friends“). Also, instruments in international law, such as the United Nationals Convention for People with Disability, have set the weather, in the way that, say, the Human Rights Act, possibly about to be repealed, might not.
But troublesome faultlines remain. For example, NHS spending is notionally being ringfenced, despite increasing ‘demand’ , but social care funding has not. The budget for Health Education England is substantially more than for Skills for Care, for example, reflecting different institutional priorities between professionals and practitioners perhaps.
When somebody receives a diagnosis, it’s invariably their friends and/or family who also deal with the diagnosis as a “team effort”. While the actual disclosure of dementia can be suboptimal, and here we need to be particularly mindful of success of people from different cultural backgrounds and with learning difficulties in obtaining a diagnosis, sometimes post-diagnostic support can be diabolical.
It might be a question of knocking on various doors, such as hospital services, or social care, but without proper care coordination, the system may present itself as a higgledy piggledy mess. Whilst research into better treatments is clearly for the benefit of society, we have to be realistic about we can achieve; we are unlikely to achieve ‘a cure for dementia’, in the same way that progress for the cancers, in treatments producing virtual remission, has been piecemeal across the years.
Progress is nonetheless being made, not least in identification of key issues. For example, people presenting with younger onset dementia often are testament to the notion that dementia’s not only about memories; some persons with ‘posterior cortical atrophy’ get driven round the houses seeing opticians for their complex visual problems, before seeing a cognitive specialist.
Above all in policy, we do need to learn from each other, and top of this must be the living experience of people living with dementia and those who find themselves in a caring rôle, often relatively underreported with little formal introduction from training. There’s been a lightbulb moment in policy, where it’s been OK to acknowledge that there’s space for all of us; for example, dementia advisers do different things to dementia support workers, or clinical specialist nurses. Not everything is clinical (indeed the policy drive has been to rely less on drugs where drugs are inappropriate). Different parties have different expectations, such as in the education and training of others, ability to enable and protect carers and people with dementia with coping strategies, or attention in specialist areas such as end of life.
A system oriented at wellbeing necessarily expects you should look at what people can do, rather than punish them for what they cannot do. I myself am now physically disabled, so the idea of reablement and rehabilitation is one I philosophically enrol to. And such an approach has to be joined up; and personalised. We all prefer have own clothing tastes, reflecting our experiences in the present and future. You’d never embark on making people all dress the same; so therefore an approach which totally disregards personhood is now totally unacceptable.
We’ve come a long way, but I can’t emphasise enough how I feel ‘experts by experience’ must be in the driving seat in service design, even including ‘new models of care’ and research priorities. These issues are not easy, often controversial, but I feel strongly we should not “shy away” of confronting them.
Remarks about this title
‘I congratulate Shibley on writing a book that brings together so many of the challenges facing people who are living with dementia, their families, and professionals from many different disciplines, and takes them forward in a critically thoughtful way. This is a book that truly points the way to a future where living better is a reality for everyone affected by dementia.’
– Beth Britton, Freelance Campaigner, Consultant, Writer and Blogger
‘This new book is an immaculately researched guide to living with dementia in England in the 21st century, covering the subject from policy to lived experience, but always with consideration and compassion. There is no better introduction to the challenges and complexities that dementia brings to individuals, families and society.’
– Geoff Huggins, Director of Health and Social Care Integration, Scottish Government
‘This book is informative and challenging in equal measure. It not only provides a thorough analysis of the issues currently facing dementia care, but it also offers a refreshing and thoughtful critique of the many challenges. Each chapter carefully combines research evidence, practice issues and policy influences, and contextualises these within the experience of those living with dementia, including their carers. Whilst this book is complex and thought-provoking – I believe it is a highly welcome counterbalance to current thinking on how to improve the lives of all those who are affected by dementia. It will force the reader to challenge their own thinking about dementia, not just as an illness but as a social construct, and as such I would highly recommend it.’
– Rachel Thompson, Professional & Practice Development Lead for Admiral Nursing, Dementia UK
‘Shibley Rahman follows his first brilliant book on dementia with this fascinating publication, containing insight and empathy in equal measure. This book will help readers – health professionals and the public alike – to understand people in their lives with dementia, guiding you through everything you ever wanted to know about dementia and could possibly want to ask. Shibley guides you through the challenges of caring for people and living with dementia. He doesn’t shy away from the topics that are uncomfortable, but he also gives space to examples of good living and practice that leave the reader with hope and positivity.’
‘I commend Shibley for this valuable addition to the current thinking and discussion on what it is to live with dementia. This text builds quite significantly on his original work and continues to challenge professionals on issues of importance for families affected by dementia. I find his frank and open style refreshing, unreserved in his willingness to question both the semantics used in practice and assumptions that are too easily made on what it might be like to live with dementia.’
– Karen Harrison-Dening, Senior Fellow at Institute of Mental Health, University of Nottingham
Other information
Living Better with Dementia: Good Practice and Innovation for the Future
Shibley Rahman (forewords by Kate Swaffer, Chris Roberts and Beth Britton)
The Amazon page (yet to be fully updated) is here.
What do national dementia strategies, constantly evolving policy and ongoing funding difficulties mean for people living well with dementia?
Adopting a broad and inclusive approach, Dr Shibley Rahman evaluates critically existing dementia policy. He tackles head-on current and controversial challenges at the forefront of public and political discourse, such as leadership, access to services for marginalised groups, stigma and discrimination, integrated care, care and support networks, rights and budgets, personalised medicine and the use of GPS tracking. Drawing on a wealth of diverse research, with voices from around the world, he also identifies positive avenues for living better with dementia, such as creativity, and highlights pockets of innovation and good practice to inform practical solutions for the future.
Shibley Rahman graduated in neuroscience and medicine from Cambridge University. There he also completed his PhD in frontotemporal dementia, commencing a lifelong interest in the timely diagnosis of dementia. He also trained to postgraduate level in medicine, law and business. Shibley speaks regularly about dementia diagnosis and post-diagnostic care, researches wellbeing and advocates rights-based approaches.
Dementia’s about real people, and for me, whatever the minutiae of policy aims in cure, care, research and dementia inclusive communities, I feel it’s all about hope.
As I was in a cab going from North London to West London, the radio happened to be on. And up popped Jayne Goodrick for National Carers’ Week for the Jeremy Vine show on BBC Radio 2. http://www.bbc.co.uk/programmes/p02sxhl5/player There’s no escaping from Jayne sometimes for me, in a completely good way.
I can honestly say I had a koala of a time when we all trekked off to the Western Australia for this year’s Alzheimer’s Disease International conference in April. Here’s Jayne with the ceramic koala I later gifted Kate Swaffer.
Jayne and Chris made it from Rhudlan, Wales, setting off at 4 am. Despite that Jayne looked very spritely and incredibly excited about the event. And actually yes – we are still buzzing about this event, as it’s got a great atmosphere. It hasn’t got the stuffiness that you can sometimes get – it just has people who want to spend time with each other.
The first thing you can be reassured about is the fact you’re at the right venue; not least as it’s a bit of a ‘who’s who’ in dementia care who turn up (very famous people from Twitter who all share a common interest in living with dementia and caring). My only complaint about the ‘dementia friendly’ nature of the venue is that the numbering around the stalls was not at all systematic, very disorienting, and should be rationalised in future.
The first thing to say is that the programme for anyone with a passing interest in the lived experience of individuals following a dementia diagnosis, issues relevant to carers, domestic or international policy, will love this conference. The talks in a diverse and detailed programme were invariably packed, and delivered to an exceptionally high standard. It is remarkable that this event is so inexpensive compared to normal conferences on dementia; this is because the emphasis is not on selling products to commissioners who can get paid to go to such events from local budgets, to grease the cogs between commissioners talking to other commissioners, or journalists oiling whom they perceive to be ‘key stakeholders’.
The emphasis instead is completely on the people who matter: people with dementia, carers and especially family and friends who become vicariously engulfed into this world. I’m not a huge fan of West London, to be blunt. But everytime I’ve even to London Olympia, it’s been incredibly well organised, and people there very helpful.
The first person who greeted me at the Alzheimer’s Show was Marc Wortmann, CEO of Alzheimer’s Disease International (ADI). And of course the first thing that Marc told me me about was the groundbreaking report from the ADI on “Women and Dementia” and that Dawn Brooker would be presenting the findings at lunchtime. I did in fact go as advised; it was a fascinating talk; and made me conclude (like I did for Prof Martin Prince’s talk that we must have these seminal findings seeming their way into the national plans for dementia).
The policy plank that is ‘women and dementia’ is incredibly important for a number of reasons. I should let you read the reports for yourself. And it’s not just the ADI who’ve had a crack at this. I had a long chat with Nada Savitch whom I think is brilliant. Involved in ‘Innovations in dementia’, Nada is really not interested in any of the stuffiness which can accompany working in the dementia field. Her primary interest in learning off people who’ve been given a clinical diagnosis, and carers, often family members, what makes them tick and what they want; and likewise has contributed much herself on understanding women and dementia.
Likewise, Beth Britton, who last week was at a Macintyre Charity event (this charity has a particular interest in intellectual difficulties), is also very interested in promoting issues to do with women and dementia, anyway.
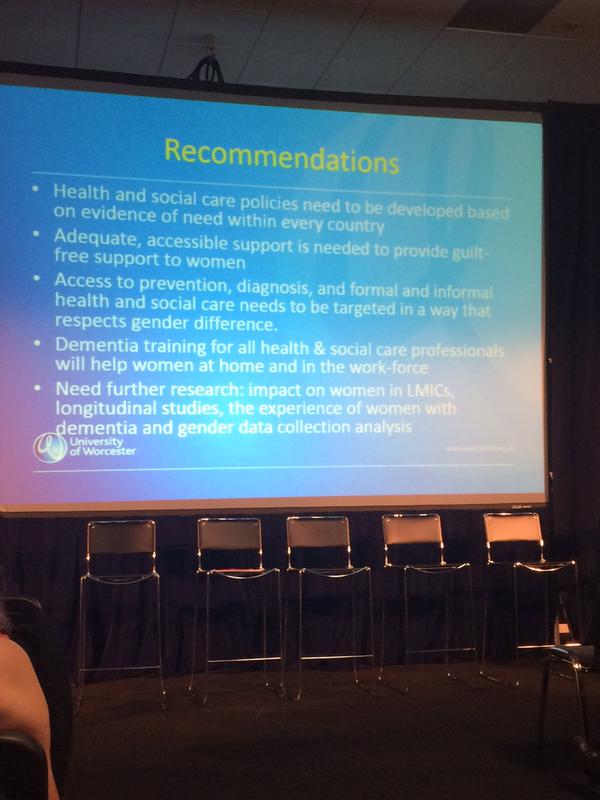
Here were yesterday’s recommendations from the ADI:
I’ve got a habit of turning at events in England and around the world where @KateSwaffer will suddenly spring up on a slide or overhead. And yesterday was no exception. Here’s Kate being mentioned by Prof Dawn Brooker.
And here is Kate again on the @AlzDisInttwitter feed.
The findings of the report are truly remarkable, and I do commend them to you. Across all regions of the world, dementia disproportionately affects women. It turns out more women live with dementia than men. The prevalence is higher for women than for men; women are more at risk of developing dementia and the symptoms they live with are more severe. Women provide a substantial proportion of informal care to people with dementia, with around two thirds of primary caregivers overall being women; and this figure is significantly higher in LMICs, areas which will account for 71% of the global prevalence of dementia by 2050. There were numerous hard copies of the report made available on the “Red and Yellow Care” stall.
Earlier this week, in the NHS Confederation, Duncan Selbie of Public Health England discussed why public health was an unique policy offering, but how it was essential to make it integrated as a concern of whole policy. This indeed is especially true in dementia. I agree entirely with Jeremy Hughes that, parallel to developments in symptomatic treatments, a major line of avenue must be prevention. I find the prevention area difficult, as it is well known that there have been very learned people who’ve developed dementia (such as Iris Murdoch), but the policy discussion needing to be had is an important one, as prevention of illness, health and wellbeing is part of the national narrative, and comes up in an analysis of non-modifiable risk factors.
Inevitably, it’s hard to sit through talks feeling very hypoglycaemic. It is however extremely helpful to have tweets which display conveniently sweets dotted around the event, together with bay numbers.
Here was what I spent ages hunting for, from Four Seasons; I would have got there sooner had it not been for the clumsy numbering of the booths.
I don’t “do” competitions, but there were tote bags dotted around the place. And it would be churlish not to get a free stress ball, when apparently stalls had “loads of them – please take one!”
Joanne Agnelli gave a brilliant talk which touched on a number of key policy issues. I caught Joanne, Gary Mitchell and Jessie McGreevy in the morning who were all buzzing with sheer joy. Here’s Joanne.
And here’s Jessie.
Here’s a ‘cheesy shot’ of me and Gary.
Jeremy introduced the whole event. I really liked what he said during the whole day, including “we can all make a difference not only to those living with dementia now but for many years to come “. Jeremy underlined the need to share good practice, which is of fundamental importance to research and service provision
.
Ironically, the second person to find me was Chris Roberts. We’d effectively travelled all around the world to re-convene again in the Mini-Australia, that is West London.
Chris in Western Australia had been speaking about his lived experience of dementia, having been diagnosed in his late 40s with mixed vascular and Alzheimer’s dementia. But he also speak of the importance of research in dementia (both in national and global policy), how it had inspired him to campaign on better research. Chris is one of those people who believes that high quality into care is important, like treatments for better symptom control; and that research is pivotal for this. I was on Prof Martin Rossor’s firm once upon a time at the National Hospital for Neurology and Neurosurgery; and of course Prof Rossor is now national clinical director for research in dementia for NIHR DeNDRoN.
And I loved dropping by the Sweet Tree stand who are seeking to coproduce sustainable services with Admiral nurses, which I think is a very good thing for an extended care ecosystem involving care homes.
This was a theme that Jeremy Hughes, the Alzheimer’s Society Chief Executive who has had a remarkably successful time in putting dementia ‘on the map’ for both national and international policy. The Care Quality Commission (CQC) has reviewed the experience of people living with dementia as they move between care homes and hospitals.
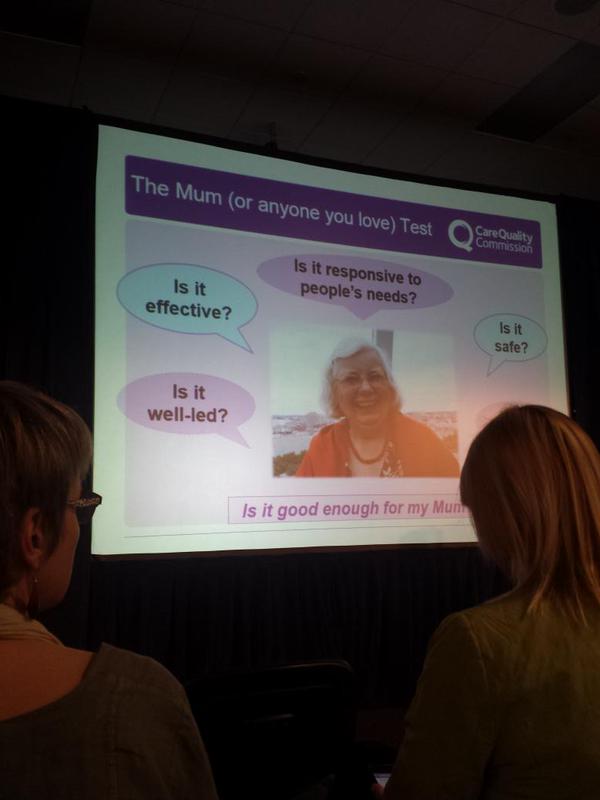
Andrea Sutcliffe, CQC’s, Chief Inspector of Adult Social Care, highlighted the findings from the seminal ‘Cracks in the Pathway’ report from October 2014, and explained how regulation can inspire improvement in services.
In my experience, it is all too easy for the clinical regulators to get deeply engrossed with ‘process’ losing an ability to see the “wood from the trees”. That’s why I feel that going back to what the public want off the regulator is essential. Andrea described a simple ‘Mum test’, which broadly speaking is that if the services are good enough for your Mum they should by and large be good enough for most reasonable members of the public. The CQC are in the unenviable position of rating care facilities across the whole range of performance, and there was a real sense that the CQC were not simply a ‘hit and run’ organisation that would produce damning criticism of providers, but also sought to signpost how care could be improved.
In a question and answer session, I asked what the panel thought were the greatest ‘barriers for care’. Dr James Warner, lead for old age psychiatry at the Royal College of Psychiatrists, was definitely ‘singing my tune’ when he referred to care being like 24 separate doors that you knock on but with no central coherence. Jeremy Hughes later said that for him it seemed that it was like knocking but not knowing for certain they were even front doors. Andrea Sutcliffe, a key person in a critical clinical regulator, said there were three major barriers in her experience: silos, stigma and secrecy (but then gave excellent explanations as to how to mitigate against all of them).
Anyway, the panel at the #AlzShow had much better success in achieving what the #Confed2015 (NHS Confederation) earlier in the week had not been able to achieve: diversity in the panel (but not yet ticking the disability or BAME “boxes”).
Jeremy emphasised that different charities would do different things for different people at different times of their dementia. Helga Rohra, chair of the European People With Dementia group, often refers to ‘faces of dementia’. Like Al Power, she rejects the ‘stages’ of dementia approach, not least because it is an inaccurate overly medical perspective. Likewise, it’s fair to say dementia advisors do different things to Admiral nurses, a type of clinical specialist nurse provision by @DementiaUK. Hilda Hayo CEO @DementiaUK and chief Admiral Nurse, further emphasised the need for ‘collaboration’.
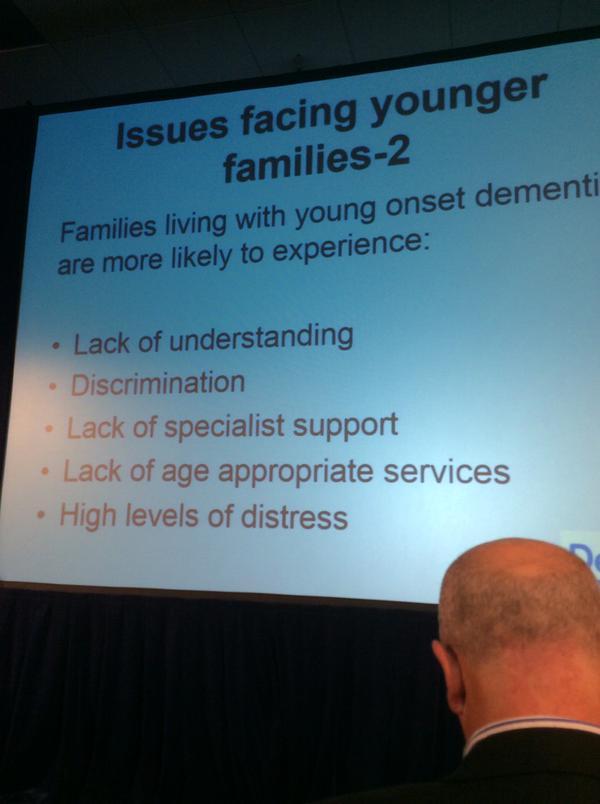
Hilda Hayo was especially good on the unmet needs of younger families where there is someone who’s received a diagnosis of dementia. Hilda’s conclusions are broadly similar as mine, not that surprising as Hilda is finishing off her doctorate thesis on behavioural variant of the frontotemporal dementia. That indeed was the subject of mine, supervised by Prof John Hodges at Cambridge, so I inevitably spent some time evangelising about my own research with Hilda.
Later today (Saturday), at 10.45 am, I will be speaking about my work under the guise of ‘Meet the authors’. This probably won’t be as interesting at Nick Higham’s version on the BBC but I will explain what I have tried to do in explaining domestic and integration in living well with dementia suitable for the general public; with of course has an emphasis on high quality research of key stakeholders, inclusive communities, “integrated” and “whole person care”, and the views of people living with dementia. As such, my books continue to be read and discussed by people living with dementia, and I hope the second one further contributes to a national debate (description here).
I’ve loved the Alzheimer’s Show – all 50% of it so far. Thanks hugely to Nigel Ward and staff for bringing it together. It’s a really special event to the many of us who are really devoted to English dementia policy. This year I, like Gary Rycroft, got a real feeling that there was more interest than ever, which I supposed to be expected as a ‘lag effect’ after the Prime Minister’s Dementia Challenge. As Jeremy Hughes argued, one advantage of having the same Prime Minister is that the Prime Minister will be forced to assess the efficacy of his own policy promises.
The political accusation, in case you have not heard it, is that structures of the main government can insufficiently promote prosperity and not pull people out of poverty. This may be couched in terms of a ‘civic conservatism’ analysis, but provokes rightly for me a need not to shy away from certain difficult issues. It would never be a stated outcome of English dementia policy to promote a ‘dependency culture’, and such accusations are fraught with political and financial overtones.
Change is not necessarily progress, but there was much to be cheerful about in Phillip Blond’s analysis of the potential beneficial outcome of devolution, from the NHS Confederation yesterday. Simon Stevens quoted David Bowie in his speech, but, especially since the media were pump primed with the £22 of ‘efficiency savings; but I wonder whether William Gibson would’ve been more appropriate – “The future is already here. It’s not evenly distributed yet.” There is no doubt that generalism is a highly valued specialism in itself, but I think this is the one area in policy where we must not denigrate diversity in talent. Controlling one’s destiny, control or agency, in living better with dementia must be an outcome many of us should wish to embrace?
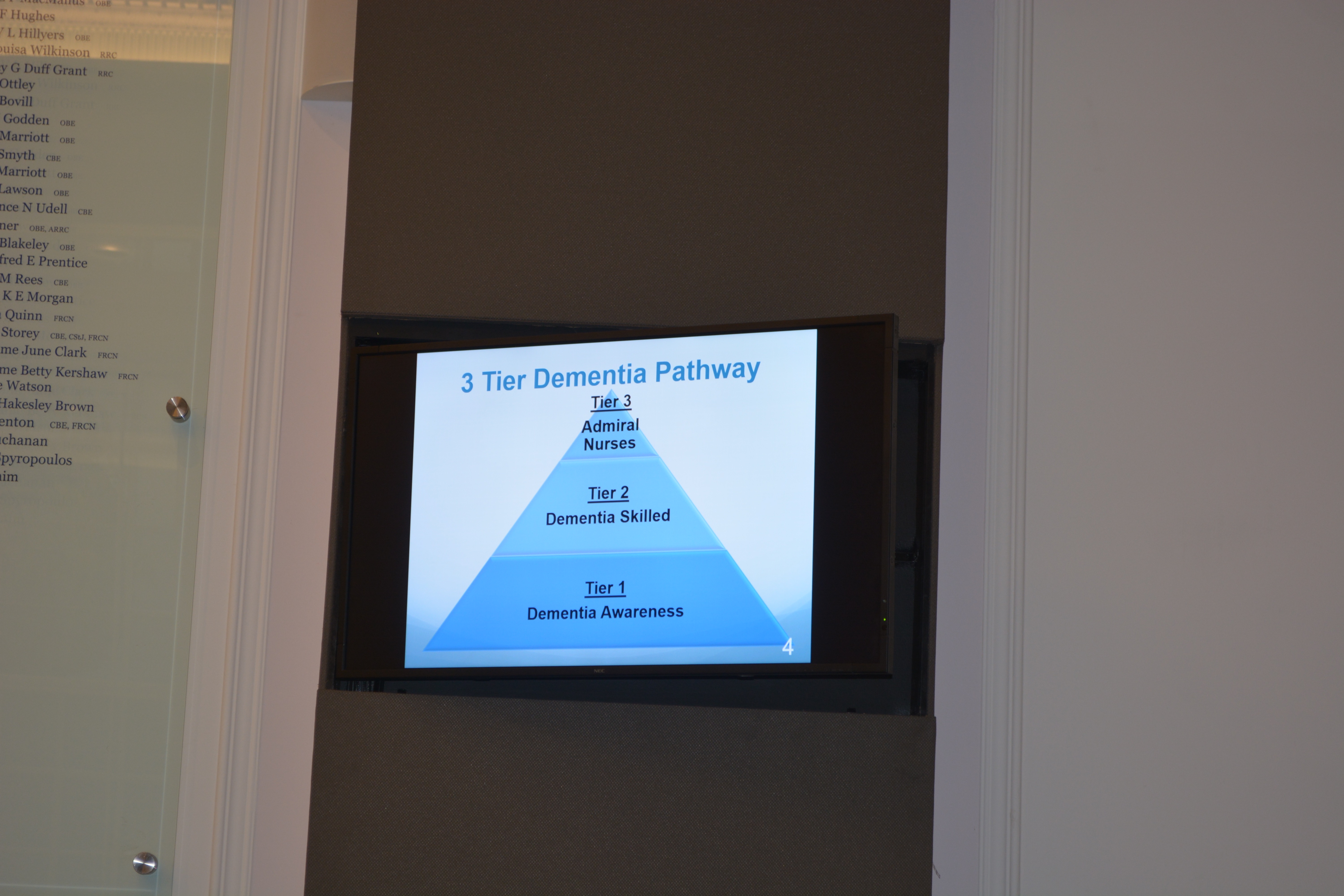
Whilst ‘awareness’ of dementia for example is important, it’s also great that we can have specialist Admiral dementia clinical nurses who can do the ‘heavy lifting’ in dementia-specific issues, such as care and support of the needs of carers, initial diagnosis, end of life care, clinical issues (such as eating, incontinence, mobility). Such an approach might be illustrated in this policy ‘pyramid’.
And it must be a concern that certain institutions exert a new monopolistic power, it seems, on health and care. Even a small number of entities can collude together (oligopolies) to produce monopolistic effect. We have the exactly the same parallel in providing of health and care, if hospital services collude amongst themselves to drown out the wonderful pro-active work that could be done in primary care to encourage health and wellbeing.
This of course is highly desirable in changing a ‘fragmented illness service’ into a ‘national health service’. Before mobilising a social movement into actions, one is obliged I feel to articulate the narrative carefully to begin with. Such a movement may be at best ‘leading from the edge’, but certainly involves working with other people, not being seen as a ‘pain in the arse’, and not merely heckling from the sidelines. I think all mainstream political parties have been keen to promote ‘choice’, and we see this particularly in the policy strand that is personal budgets. But I think often we ignore of who is actually in control; patients may not necessarily know they’re pawns in a global power game when they’re prescribed a statin not engaged in a dialogue about healthy diet. A healthy diet may help with your obesity as well as your headline figure of cholesterol?
Also, it may be possible to construct a microcosm of members of society working with each other in collective action, rather than all having individual monopolistic relationships with the State, in a devolved environment. Clinical specialist nurses should not viewed as an outpost of the State, I feel, but part of this same conversation that people with dementia and carers want. They should be the power brokers between parties, as they already are between statutory and non-statutory services, but also as knowledge brokers in communities of practice exerting much education and training power.
But the bottom line is that you can’t have control sadly unless things are properly funded. We need a commitment that these cash injections will start now not in five years time, for example. I asked Dr Peter Carter, RCN general secretary and Chief Executive, earlier this week whether there is a rôle for specialist nurses in the new English dementia strategy. Peter said ‘very much so’, then strongly explained how investing in the nursing workforce was better than short-sighted measures. I had previously had this conversation with Prof David Croisdale-Applebly, Chair of Skills for Care, after one of the sessions in the ‘Admiral nursing conference’ earlier this week at the Royal College of Nursing. David explained that it was also important to make the commissioning case carefully, as well as the clinical one, and that power would come through evidence. David of course was influential in establishing the authority of NICE, and indeed I went on my policy high horse about the need for such regulatory capture to command social prescribing. David emphasised that the case could be made for clinical nursing specialists could be made out at a national not just local level, with levers such as QUIP for example.
A distributed authentic leadership, with the voices of people with dementia and carers easily heard above the ‘noise’ is King. It’s all too easy to be entrenched in an impenetrable haze of jargon and terminology such as ‘new models of care’, but the idea that people with dementia and carers have more control over the management of their wellbeing and medical needs is for me a very attractive one. And one should not pull away support, as traditionally described, for medical including psychological needs. This should not be absolving responsibility from the NHS, particularly if viewed as the NHS ‘not being able to afford it’. Self management, however activated, with the right information is not just the domain of ‘the right’. But this is an acknowledgment that a person’s wellbeing needs might be much greater than those provided from the health and care services only.
Sources of inequality, such as housing or transport, have to be put into the mixer, but this will be possible at a level where people in society and communities can indeed communicate effectively with one another. The problem with the traditional alternative is that it can vastly restrict what is the policy offer, which I feel is detrimental to promotion of living better with dementia. Care homes, where there are over 400,000 residents, many of whom are living with dementia, are not to be viewed in isolated, but part of the wider health and care system, which should be funded much better than it is currently.
Personal control over wellbeing needs to be a focus in future English dementia policy, and should be a policy aim rightly in itself. It can never be presented simply in terms of ‘saving money’. This will not engage the hearts and minds of the public. And whilst the phrase ‘there is no such thing as society’ has been widely discussed, it is clear to me that people with dementia and carers do need to be given the tools to speak to one another, and not just been in contract with a limited number of ‘providers’, to bring about an organic progress in English dementia policy.
If you have a passing interest in organisational learning and development, you have to be necessarily interested to some extent in organisational structures. There is remarkable ‘complexity’ in the landscape of the dementia strategy for England potentially, not least because there are so many factors which are inherently uncertain: such as political, social, cultural, environmental, legal and technological factors. The issue of “bounded rationality” though obliges us to think about what factors are within our control and within our field of vision in forming strategy, and this ‘creative strategising’ as Marshall Ganz calls it is not without its perils.
When one thinks about ‘communication’ being turned into action, there are quite a few directions we can pull in. It turns out that pair of cancer drugs can shrink tumours in nearly 60% of people with advanced melanoma, a new trial has suggested. An international trial on 945 patients found treatment with ipilimumab and nivolumab stopped the cancer advancing for nearly a year in 58% of cases. Now, these drugs are examples of ‘monoclonal antibodies’, and I once sat next to the person who invented this (disruptive) technology at dinner in Cambridge. A man called César Milstein; a very modest man, but he certainly had nothing to be modest about. Delightfully humble, he won the Nobel Prize for Physiology, despite Cambridge to my knowledge not offering him a professorship. And indeed the same technology in a different guise was ultimately responsible for saving somebody’s life from Ebola at my local hospital, the Royal Free in North London.
In December 2013, leading nations committed to developing a cure or treatment for dementia by 2025 at the global dementia summit. I personally find such a simple message at one level problematic, but at another it conveys a perfectly laudable message which conveys hope not fear. The BBC website ran a similar message today based on the melanoma development.
In the past, I have been one to raise eyebrows at the statement that dementia is where cancer used to be at twenty years ago, in that the veil of stigma surrounding dementia is comparable to that which surrounded the ‘C word’. But in the past treatments or cures (however so defined, possibly near perfect remission) for cancer would’ve been unheard of.
But it ‘frames a narrative’ in a straightforward way. In other words, the cure for dementia may in fact be a cure for Alzheimer’s disease. This in itself does matter if you look behind the details of the immunotherapy way of dealing with melanomas this way; instead of attacking the growth of cells itself, you end removing the protection of the human body protecting these abnormal cells. This is of course not a million miles from the build up of tau or amyloid substances in Alzheimer’s disease (although their precise rôles in disease production is still far from certain); nor is it a million miles from the build up of other noxious substances in other types of dementia (such as tau in the frontotemporal dementias).
Paralysis of analysis can lead us potentially to not get past ‘go’. That’s why I also find the ‘I statements’ helpful in dementia policy, and it’s been a big success of Dementia Action Alliance and the Alzheimer’s Society to plug away at this.
I was diagnosed in a timely way
I know what I can do to help myself and who else can help me
Those around me are well supported and are in good health
I get the treatment and support, which are best for my dementia, and my life
I feel included as part of society
I understand so I make good decisions and provide for future
I am treated with dignity and respect
I am confident my end of life wishes will be respected. I can expect a good death.
I know how to participate in research
But my concern about ‘physics’ is that it is held from the laws of entropy that systems degenerate into chaos. When you look at the concourse of Victoria Station here in London, it looks like a complete dog’s dinner, and yet when you look at individuals people are heading away from and towards their platforms in some sort of order. Likewise, the messaging of narratives will be done by individuals and parts of organisations in various ways; but ultimately better drug treatments (whether ‘cures’ or symptomatic therapies), if used appropriately, might be able to complement care and improve the wellbeing of people living with dementia.
This is where I genuinely feel turning ‘communication into action’ gets potentially complicated, as long as we can pull together despite our differences. People react to circumstances in different ways, and when I ask people how they wish to contribute to ‘dementia friendly communities’ answers show a remarkable diversity, including ‘helping mum’ or ‘promoting research’. So, whether it’s a ‘call for action’ in reducing inappropriate prescriptions for antipsychotics, or for promoting support of family caregivers for dementia through a new dynamic network (such as through the previous #DAACC2A), or whether it’s a mission to promote a #ARUKfightback to ‘get behind research‘ I’m actually all for it. One point of disagreement I have with the social scientists investigating social movements is that I feel the rôle of emotions in guiding cognitions has been hugely understated in the ‘communication for action’ construct. We know that emotions play a massive role in shortcuts in guiding decision making, ultimately this is important for system leadership and ultimately whole systems regulation. Differences do matter, and ultimately many of us are striving for a whole person-centred integrated service, but what must be a common driver of transformational change in dementia, I feel, is hope overcoming perceived dissent. Acknowledging we all have something ‘to bring to the table’, diversity, is going to be essential whatever actions we ultimately decide to adopt for English dementia policy.