English film director Alfred Hitchcock (“Hitch”) made cameo appearances in 39 of his 52 surviving major films.
For the films in which he appeared, he would be seen for a brief moment boarding a bus, crossing in front of a building, standing in an apartment across the courtyard, or even appearing in a newspaper photograph.
This playful gesture became one of Hitchcock’s signatures; and fans would make sport of trying to spot his cameos.
As a recurring theme, he would carry a musical instrument — especially memorable was the double bass case that he wrestles onto the train at the beginning of “Strangers on a Train”.
In “The Birds”, as Melanie Daniels (Tippi Hedren) enters the pet shop, Hitch is leaving with two white Sealyham terriers.
This is a film of every single ‘Hitchcock cameo’.
Here are some recent cameos.
Full details about my book are on the Radcliffe website here.
Here are further ‘tweets of support’.
@legalaware Thanks for the RT! You seem to be having huge success with your book. Delighted to see the wonderful tweets about it. Well done!
This is the programme for today which I’m looking to enormously today.
I will be promoting heavily the cause of living well with dementia, to swing the pendulum away from pumping all the money into clinical trials into drug trials for medications which thus far have had nasty side effects.
In keeping with this, I have been given kind permission to give out my G8 Dementia Summit questionnaire to look at delegates’ perception of what this conference was actually about.
We need also not to lose sight of the current persons with dementia, to ensure that they have good outcomes in the wellbeing.
This can be achieved through proper design of care environments, access to innovations including assistive technology, meaningful communities and networks for people with dementia to be part of and to lead in, and proper access to advocacy support services and information which empower choice and control.
There’s a lot to do here – and we need to have high quality research into all of this arm of research too.
Coming back home to Scotland is like travelling back in time for me.
I was born in Glasgow on June 18th 1974, and my lasting memory of leaving Glasgow for London 37 years ago was how relatively unfriendly Londoners were in comparison.
Of course the train journey through the beautiful England-Scottish border countryside brought it back to me. There’s a lot to be said for getting out of London. It’s an honour to be here back in Scotland.
I had absolutely no idea I would have such a warm welcome here in Scotland. Still feeling incredibly emotional I’m here at all in Glasgow.
Dedication • Acknowledgements • Foreword by Professor John Hodges • Foreword by Sally Ann Marciano • Foreword by Professor Facundo Manes • Introduction • What is ‘living well with dementia’? • Measuring living well with dementia • Socio-economic arguments for promoting living well with dementia • A public health perspective on living well in dementia, and the debate over screening • The relevance of the person for living well with dementia • Leisure activities and living well with dementia • Maintaining wellbeing in end-of-life care for living well with dementia • Living well with specific types of dementia: a cognitive neurology perspective • General activities which encourage wellbeing • Decision-making, capacity and advocacy in living well with dementia • Communication and living well with dementia • Home and ward design to promote living well with dementia • Assistive technology and living well with dementia • Ambient-assisted living well with dementia • The importance of built environments for living well with dementia • Dementia-friendly communities and living well with dementia • Conclusion
Reviews
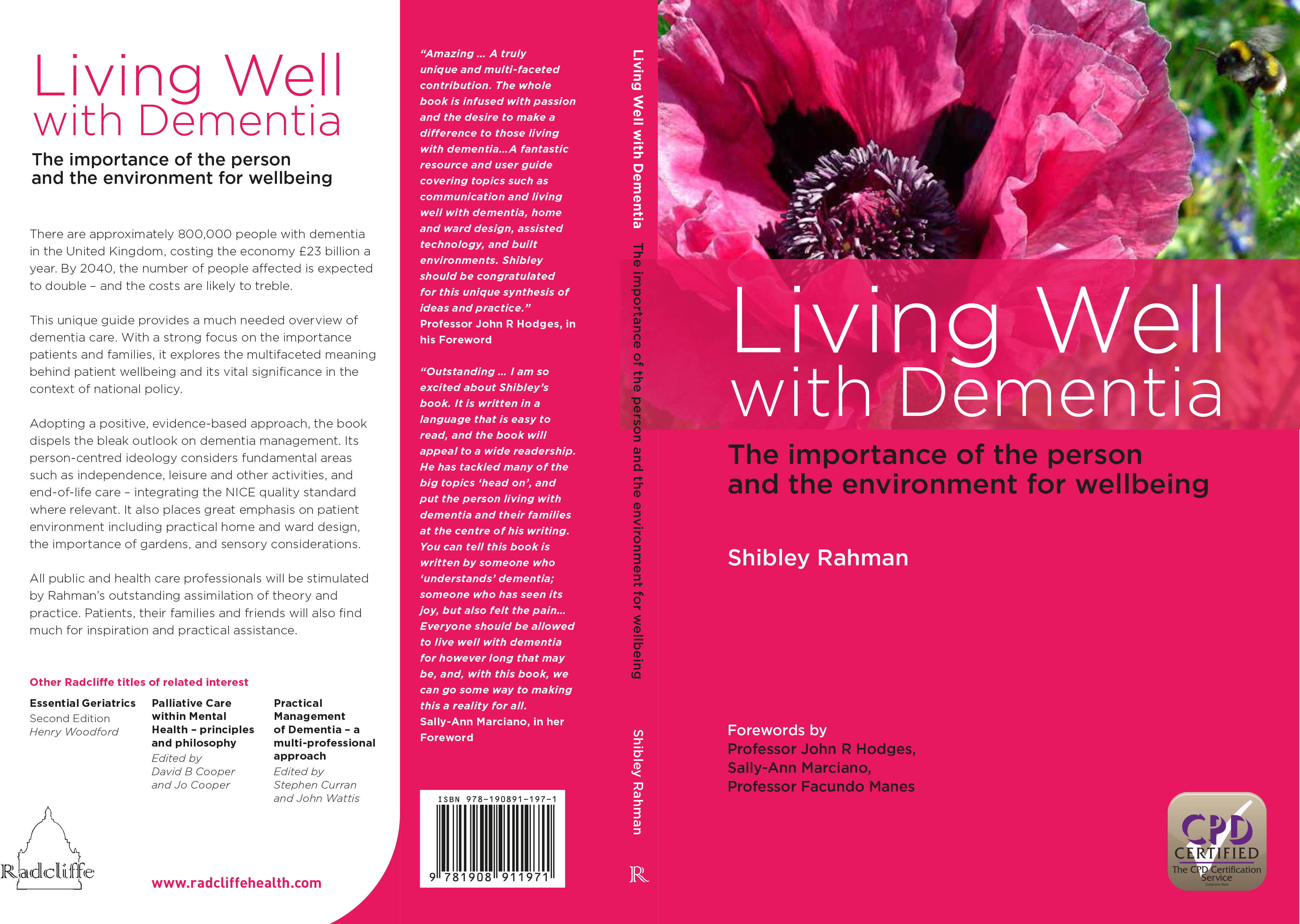
Amazing … A truly unique and multi-faceted contribution. The whole book is infused with passion and the desire to make a difference to those living with dementia…A fantastic resource and user guide covering topics such as communication and living well with dementia, home and ward design, assisted technology, and built environments. Shibley should be congratulated for this unique synthesis of ideas and practice.’ Professor John R Hodges, in his Foreword
‘Outstanding…I am so excited about Shibley’s book. It is written in a language that is easy to read, and the book will appeal to a wide readership. He has tackled many of the big topics ‘head on’, and put the person living with dementia and their families at the centre of his writing. You can tell this book is written by someone who ‘understands’ dementia; someone who has seen its joy, but also felt the pain…Everyone should be allowed to live well with dementia for however long that may be, and, with this book, we can go some way to making this a reality for all.’ –Sally-Ann Marciano, in her Foreword
I don’t go to “trade fairs” where people display their latest ‘products’ for dementia. I am an outsider, and very happy to be so so.
But I do feel my book is having an impact slowly with the right people.
For example:
@a_carers_voice sitting in sunshine London garden reading @legalaware living well with dementia – what a read … Brilliant Shibley …
These are just some of the messages in the ‘little black book’ I was given at my book launch for ‘Living well with dementia’ (details here). Ones not shown have not been excluded out of any malice. I am hugely proud of people who kindly made it to Camden to celebrate my book on February 15th 2014. I am of course hugely indebted to Gill Phillips (@WhoseShoes) for presenting me with this ‘little black book’, which I promise to cherish forever. #KoalaHugs
I felt very happy to give a copy of my book to Prof Sube Banerjee, newly appointed Chair of Dementia at Brighton and Sussex Medical School. Sube has in fact been the lead for England for dementia – his work is quoted in my book, and I think he’s made an enormous contribution to the living well with dementia literature.
And what does the future hold for ‘living well with dementia’?
Here is a sample chapter from my book ‘What is living well?’
‘Living well’ is not some bogus mantra for the hell of it. It is an ideological standpoint which serves to promote the dignity of our fellow citizens who happen to also have a clinical diagnosis of dementia.
And here are the “beautiful people” who came to my book launch at the Arlington Centre, Camden, one afternoon in February. I can’t believe that this wasn’t even a month ago now!
One of the happiest days, as well, was giving Joseph a copy of my book as a gift.
Joseph was in fact my carer when I could hardly walk or talk, when I was in physical recovery from meningitis on ITU (where I was unconscious in 2007).
And those were the days…
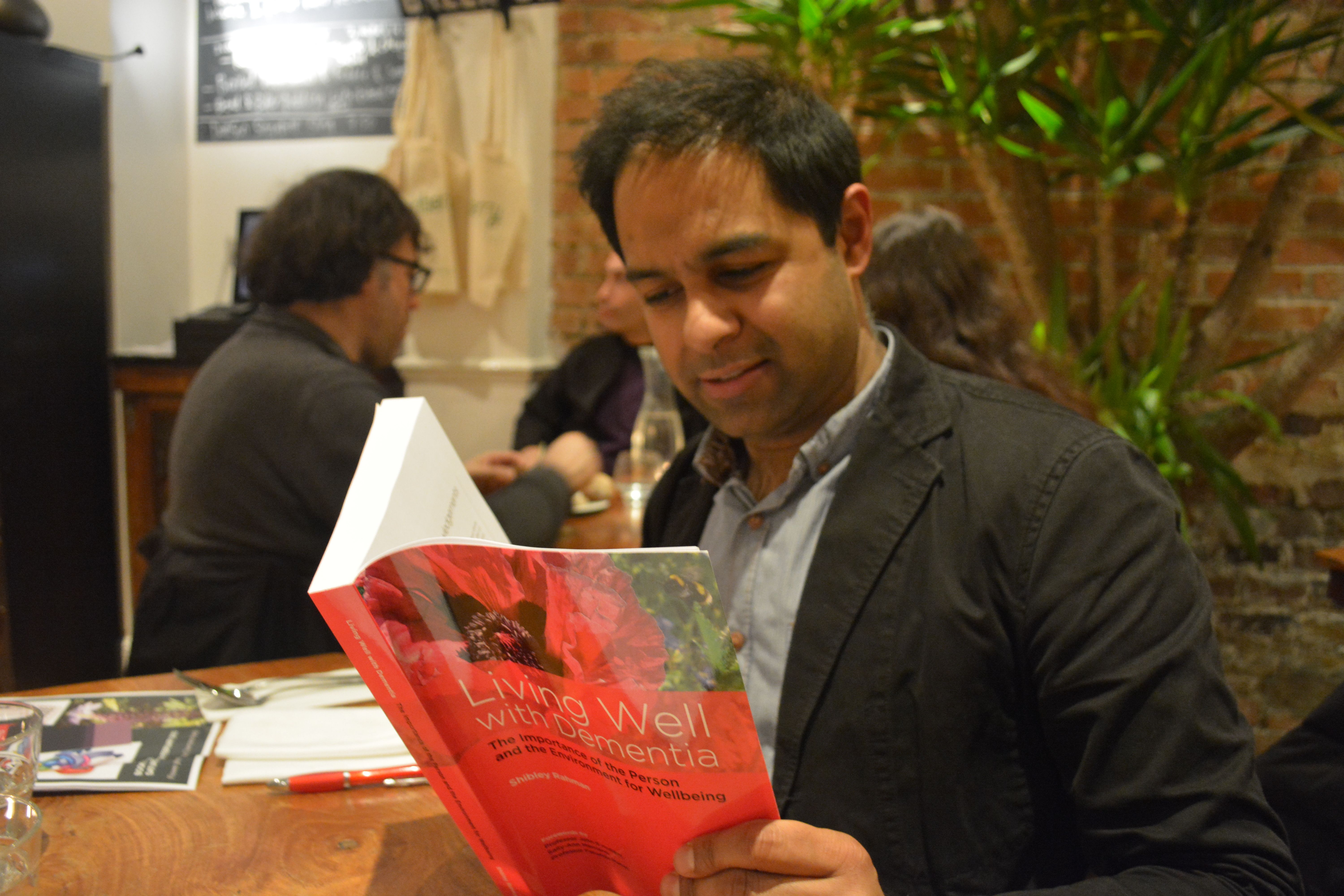
And THIS is the famous poppy.
This picture was taken by Twitter pal, @charbhardy, first amongst equals in the #dementiachallengers.
After I said I was buying my own copies, @KateSwaffer asked:
But Kate has read a copy of my book from cover to cover:
And as @Norrms says – how can ‘living well with dementia’ fail?
These structural problems are, not least, to what extent will the NHS be paid for out of general taxation in the long term. The issue is not fudged altogether, in that Oldham calls for a future government to look into this as a priority.
Nonetheless, the Oldham Commission does fudge the issue of how much integrated and social care systems can rely on private not state provision. This is a strange ‘elephant in the room’, given the emphasis of the report on individualised budgets (call them what you will, personal budgets or personal care budgets).
Oldham does however concede helpfully that ‘financial arrangements in the adult social care system are equally fragmented, with complex and overlapping funding and provision arrangements between private and public funding sources, and private and public providers of care. The multitude of private care providers adds to this complexity.’
The need to repeal section 75 Health and Social Care Act is pivotal to all this. In fact, a repeal of the whole Act, as Labour (as Andy Burnham and Ed Miliband have indeed promised), would be helpful. This is, quite simply, because legally integration might offend the competition legal infrastructure established by section 75 and its associated Regulations, and of course sit uneasily with EU competition law.
At the moment, the NHS and social care services are geared up to ‘reacting to events’. And this is reflected in the payment by results mechanism (a reincarnation of ‘activity based costing’).
“Public funding has increasingly focused on those with greatest needs – particularly as rationing of care has become more severe – driven by a reactive, crises oriented approach rather than a focus on early intervention and wellbeing.”
Wellbeing is of course not just the opposite of illbeing, though lessons can be learnt from poor hydration and nutrition, for example, in individuals with advanced dementia.
The Oldham Commission view health and wellbeing boards as a vehicle for collective system leadership for whole person care,” involving the leaders of existing organisations working together to coordinate care and align incentives across their geography.” And therefore it is critically important that they are fluent in what wellbeing is, and how to promote it. This is especially important for dementia, but I would say that wouldn’t I.
Information is obviously vital in decision-making along a path to wellbeing however defined. I, in fact, devote a whole chapter to decision-making in my book ‘Living well with dementia’.
The exact mechanism of integration of voluntary organisations and health and care services to provide a combination of medical and non-medical support as part of the care pathway for older people living with multiple long term conditions needs of course to be put under greater scrutiny.
The ‘deal‘ between the Department of Health and the Alzheimer’s Society in promoting ‘Dementia Friends’ is of course welcome in promoting awareness of dementia. But we do need to be careful that, firstly, other dementia charities do not suffer in a ‘zero sum gain’ manner. Secondly, we need to be doubly sure that charities are not expected to pick up any shortfall in state provided services. Already there’s valid criticism of the way in which private companies can legitimately ‘cherry pick’ services to maximise their shareholder dividend.
Oldham’s group is right to refer to “a strong evidence base now exists to target key risks to health independence and wellbeing in old age.” Clearly there’s a balance to be struck between independence through assistive technologies perhaps of persons living with dementia in their own homes, and social inclusion with other persons face-to-face. Online communities offer great value for persons with dementia nonetheless.
Oldham’s team also helpfully reviews how Preventive aspects of whole person care must therefore pay attention to environmental factors. The emphasis in the Report is on diet, but this is valid too for dementias in the context of vascular dementias. Vascular dementias are common in older age groups, and certainly medical professionals, dieticians and others are keen at considering cholesterol and diet, and their interaction with other factor such as smoking.
Therefore, one of the conclusions is that, “Whole person care should not only include joining up services …”
It is inescapable that whole person care should include ‘joined up services’. Data sharing different disciplines, despite the concerns about #caredata, needs to involve a more effective dialogue with the general public, one expects.
The report also picks up on a number of other important issues.
One is the possible interaction with benefits. People with disabilities, for example, are right to wonder if benefits might be taken away if the system drives towards ‘whole person care’. On the other hand, it does not perhaps make intuitive sense for the care and benefits situation to work in isolation?
This is of course an intense political quagmire, given ATOS’ role in both the GP extraction scheme and the implementation of the much criticised disability and employment benefits.
Also, it turns out that 70% of people over 75 live with a major long term condition and a quarter live with two or more. Many persons living with dementia also live with otherconditions.
Furthermore, the Report notes that, “in all groups in society, housing has a large impact on people’s health and wellbeing.” As perhaps care embraces personhood in the true meaning of Kitwood or otherwise, the influences of other people in society, such as housing or the criminal justice system to name but a few, may become apparent.
But what the State is by that stage is anyone’s guess. In the meantime, the Oldham Report is fully consistent with my book ‘Living well with dementia’.
I had expected this to be the case. In fact, there’s a paragraph on whole person care in my book.
I held a private book launch for guests of mine, who are interested in dementia at the grassroots level.
The talk was dedicated to Charmaine Hardy (@CharBHardy), whose husband has a very rare type of dementia known as primary progressive non-fluent aphasia. The publishers picked her poppy to be the cover of my book.
This for me, as was later suggested, as the book itself is dedicated to the memory of my late father (who did not have dementia but had a severe back pain which severely limited his quality of life in his final years.)
A special mention to Thomas Whitelaw (@tommyNTour) – a true gentleman and a Scot (!)
It was wonderful to meet Darren (@MrDarrenGormley) for the first time. Darren’s clearly someone who sees the person; with superb empathy skills, Darren and colleagues will need to be the change catalysts to break down obstructive silos.
It was a massive honour Beth Britton (@BethyB1886) could make it. Beth, like many in the room, of course knows this subject inside-and-out, and I am personally grateful to Beth for campaigning for the use and validation of more effective assessment of wellbeing approaches.
Here are some happy photos of my book launch.
I really couldn’t have been happier.
I am strongly against promoting my thesis about wellbeing with involvement of people as marketing ‘window dressing’
On the other hand, it gives me enormous pride to present to you the video presentations recorded by Norman McNamara, Kate Swaffer and Dr Peter Gordon which I played to my guests at the Arlington Centre in Camden on Saturday.
Friends of mine, who happen to be currently living with dementia, are also reading the book.
I mention during my presentations the ‘Purple Angels’, including Lynette Richards, Julie Line, Kim Pennock, Jane Moore, and of course Norman McNamara.
And no I am not a retainer from Ostrich Care! x
I feel it would have been it would have been “defeating the object”, if the book could not be read by people living lives with dementia.
Dr Peter Gordon is the only one of the three who does not have a dementia. He is a Consultant Psychiatrist working in this field. It was incredibly nice of him to put together his film for me, shown below.
Dedication • Acknowledgements • Foreword by Professor John Hodges • Foreword by Sally Ann Marciano • Foreword by Professor Facundo Manes • Introduction • What is ‘living well with dementia’? • Measuring living well with dementia • Socio-economic arguments for promoting living well with dementia • A public health perspective on living well in dementia, and the debate over screening • The relevance of the person for living well with dementia • Leisure activities and living well with dementia • Maintaining wellbeing in end-of-life care for living well with dementia • Living well with specific types of dementia: a cognitive neurology perspective • General activities which encourage wellbeing • Decision-making, capacity and advocacy in living well with dementia • Communication and living well with dementia • Home and ward design to promote living well with dementia • Assistive technology and living well with dementia • Ambient-assisted living well with dementia • The importance of built environments for living well with dementia • Dementia-friendly communities and living well with dementia • Conclusion
Amazing … A truly unique and multi-faceted contribution. The whole book is infused with passion and the desire to make a difference to those living with dementia…A fantastic resource and user guide covering topics such as communication and living well with dementia, home and ward design, assisted technology, and built environments. Shibley should be congratulated for this unique synthesis of ideas and practice.’ Professor John R Hodges, in his Foreword
‘Outstanding…I am so excited about Shibley’s book. It is written in a language that is easy to read, and the book will appeal to a wide readership. He has tackled many of the big topics ‘head on’, and put the person living with dementia and their families at the centre of his writing. You can tell this book is written by someone who ‘understands’ dementia; someone who has seen its joy, but also felt the pain…Everyone should be allowed to live well with dementia for however long that may be, and, with this book, we can go some way to making this a reality for all.’ –Sally-Ann Marciano, in her Foreword
Extracts from my talks
This talk was given by me (Dr Shibley Rahman) on Saturday 15th February 2014 to a group of personally invited guests. Guests included persons with dementia, carers (past and present), campaigners, academics in social care, innovation and service provision, dementia club coordinators, and dementia nursing specialists.
1. This is the first segment of the first talk.
Particular things to look out for include:
James Murray-White (@sky_larking) 6 mins
Beth Britton (@BethyB1886) 7 mins
and their @AlzheimersBRACE work
Norman McNamara’s message at 15 mins
@mason4233 (Chris Roberts)’s tweet at 19 mins
2. I start off by thanking Prof John Hodges for his kind Foreword (0) and a clear description from Sally Marciano (@nursemaiden) why she, kindly, felt the book might be helpful. I am honoured at Sally’s personal contribution to my book.
I introduce the topic of personhood, using Tom Kitwood’s seminal work as a brief introduction only, but clearly the topic is huge. I then touch upon the practical difficulties academics and practitioners have had for their definitions of ‘living well’, and the implications therefore for its measurement.
There’s a clearly a debate to be had about why diagnosis might have been so problematic, using @edanaming’s research (Edana Minghella) as a springboard. At around 9’55”, I then use the problems in giving a potential diagnosis of dementia to a person is LGB or T as an illustration.
Gill Phillips (11′ 30″) kindly gives a brief description of the background and philosophy behind ‘Whose Shoes’, a modern application of personalisation which allows service users, including persons and patients with dementia, a say on what they wish to achieve from their person-centred care.
At around 16’30” Lucy Jane Masters (@lucyjmasters), a specialist nurse in dementia, explains the remarkably successful ‘Dementia is my business’ initiative, innovative badges which have acted as an ‘ice breaker’ for bringing about a cultural change in dementia care even amongst health professionals.
This next segment concludes with a brief discussion of the ethical issues of diagnosis, through Dr Peter Gordon’s contribution (@PeterDLROW). I use Peter’s letter to the BMJ as an introduction to the seminal four ethical principles of Beauchamp and Childress (1979), i.e. autonomy, beneficence, non-maleficence and justice. I also include Peter’s video which I will also separately upload elsewhere.
3. I then give an overview of some essential topics germane to this academic debate.
The contributions by the medics have not been a complete farce.
There’s been a lot of scrutiny about the ethical framework regarding dementia from people who are medically qualified, such as Dr Peter Gordon (@peterDLROW), Consultant in dementia. This was been necessary to neutralise some of the potent fraudulent memes in the media from elsewhere.
There’s been wonderful work too by @nchadborn on including service users’ views and opinions into the design of health services, from an applied perspective, as part of Nottingham University.
And the cognitive neurologists have been important in delineating the diverse cognitive presentations of dementia. Prof Facundo Manes’ group in Buenos Aires (@manesf) have been identifying how social cognition in the behavioural variant of frontotemporal dementia can be heavily dependent on context. As an example of this, I explain the Ebbinghaus Illusion and Titchener circles. Prof Manes is a colleague of ours in cognitive neurology, and wrote one of the Forewords to my book.
4. Particular things to look out for now include:
12″ Personal dedication to Charmaine Hardy [@CharBHardy] from England for the poppy on the front cover of my book, and being a key member of the #dementiachallengers
15″ The “Purple Angels” in raising dementia awareness and dementia friendly communities worldwide narrative. Jane Moore and Norman McNamara jointly designed this motif.
21″ beginning of the message by Kate Swaffer (@KateSwaffer), based in Adelaide, Australia, to my guests. (this is the beginning of the pre-recorded message; the second half of the message is in a different video.)
5. This last segment of my recordings contains the second part of Kate Swaffer’s message to my guests, and my film ‘Love is a wonderful thing’ for my community of delegates for the book launch.
The book
The book’s Amazon page, with some testimonials, is here.
The publishers’ page (Radcliffe Publishers) is here.
Independent blogposts by Gill Phillips (one of my guests) about my book launch at the Arlington Centre
These blogposts capture for me what was an extremely happy occasion for me.
One of the biggest illusions, and this is not a ‘complaint’ about this jurisdiction only, is that large dementia charities represent the views of persons with dementia.
They have a myriad of different influences, and certainly it has become dangerous that they legitimise policy directions from which many persons with dementia and caregivers can become totally disenfranchised.
This leaves persons with dementia two options.
The first option is that they can hope to influence large dementia charities better, but this is an impossible task. They act in organised corporate ways, with much marketing and branding power, so if they decide not to adopt the agenda of persons with dementia and carers it would not be altogether surprising.
The second option is to form strategic alliances with general patient groups, but not all persons with a long term condition are ‘users’ of healthcare services which thus far have typically concentrated on illness rather than health.
The third way, and this is in my opinion the most realistic option is to organise better a national and international network of groups focused on the needs of, and run by, persons with dementia.
There are, however, very impressive carers organisations, and many of their competences and aims align with the person-driven agenda for wellbeing.
The uphill task for those of us pursuing a living well with dementia agenda is truly formidable. Cholinesterase inhibitors, the frontline drugs for treating memory problems in Alzheimer’s disease, have annual sales in the billions, but have very modest effects in the vast majority of patients. They do not reverse or markedly slow down the disease either.
I feel that getting in lost in a definition of wellbeing, and how we measure it, is not the way to win the argument, although clearly relevant to how commissioning for integrated care might happen in future, say through value-based commissioning.
I feel arguments based on cause and effect will be more compelling (and easily supported by supporting evidence). That is, memory reminiscence techniques, improving the design of homes and wards, and introduction of innovations such as the ‘Dementia Dog’, which clearly have had a beneficial outcome for many, are options worth pursuing.
The ’cause’ of attracting monies for high quality research, acting as a foundation for pharmacological interventions, is a very worthy one. As someone who has published in this arena in international journals, I certainly don’t have any weird ideological objection to such work.
But we have to acknowledge, albeit reluctantly, that the world is changing, and whether some of us like it or not becoming more “consumer-driven”.
Citizens have become consumers with status proportional to purchasing power, and there’s now a fine line between data gathering of your personal lifestyle preferences through the ‘recreational’ social media and direct targetted marketing of things to improve your health or prevent illness.
The ultimate prize for industry is to determine government policy, but smaller organisations cannot compete against the large corporations, many of which contribute generously to political organisations too.
Where wellbeing campaigners lobbying may not succeed on economic power, their organising ability might succeed on the basis of facts and logic, in seeking out a constructive alternative to the existing policy, practice, or product.
It is often said that the basic rule of pressuring targets is that politicians react to publicity that reflects on their character, bureaucrats react to disrupting their provision of services and programmes, and corporations react to loss of their product’s reputation.
Wellbeing is an agenda for which politicians could have, and have had, much affinity.
If regulations are to be implemented, it’s often possible, hijack or “capture” the regulatory process. This can become easy if the regulatory process is biased towards a medical model of dementia, e.g. the General Medical Council and NICE, rather than social care institutions which are tacitly not given parity.
A committed opponent, who for the most part we’re not interested in reaching because debate with this individual tends to harden his or her position. Big Pharma, the General Medical Council, NICE and large dementia charities are clearly not targets to promote the wellbeing agenda.
The focus in parliament, through the All Party Parliamentary Group, and to some extent helped by powerful allies in the charity and corporate sector, has been relentlessly medical too.
Prof Felicia Huppert, to which my book is dedicated, ran a Royal Society meeting on wellbeing. There is no doubt that this was very succcessful, but we have never had a corollary in parliament.
A legislative hearing, however, gives the lawmakers the opportunity to hear all sides of an issue and to ask questions and challenge witnesses in a relatively brief span of time.
In 1991, the author Michael Frayn wrote a book, A Landing on the Sun, about a British prime minister who tasked his advisers with looking into happiness and what the government could do to promote it. The prize proved elusive, the adviser went mad and died.
Even in November 2010, speaking at the Google Zeitgeist Europe conference, David Cameron suggested, “Wellbeing can’t be measured by money or traded in markets.”
“It’s about the beauty of our surroundings, the quality of our culture and, above all, the strength of our relationships. Improving our society’s sense of wellbeing is, I believe, the central political challenge of our times.”
And this agenda has not sprung out of nowhere.
Aristotle talked about “eudaimonia” – happiness as human flourishing and purpose to life – rather than the modern hedonistic concept. John Maynard Keynes talked about the “art of life” in 1930, and in 1968 Bobby Kennedy told a student audience in Kansas: “We cannot measure national spirit by the Dow Jones average, nor national achievement by the gross domestic product.”
Tacrine was the prototypical cholinesterase inhibitor for the treatment of Alzheimer’s disease. William K Summers received a patent for this use (US Patent No. 4,816,456). Studies found that it may have a small beneficial effect on cognition and other clinical measures, though study data was limited. and the clinical relevance of these findings was unclear.
Tacrine was ultimately discontinued in the US. Unfortunately, it is associated with transaminase elevation in up to 50% of patients. The mechanism of tacrine-induced liver damage is not fully understood, but earlier studies have suggested that genetic factors may play a role.
And now leading Big Pharma companies are involved in an ‘arms race’ to get their drugs to market, and they have powerful allies in large dementia charities worldwide.
Both the AstraZeneca and Merck medicines work by blocking an enzyme called beta secretase that is involved in production of beta-amyloid, a protein that creates brain plaques considered a major cause of Alzheimer’s disease.
Such oral drugs are known as BACE inhibitors and are viewed as a promising new approach to fighting the memory-robbing condition.
BACE inhibitor drugs have taken centre stage after an injectable class of medicines targeting beta-amyloid plaque failed or fell short in trials conducted by Pfizer and Eli Lilly.
Not all experts accept that reducing beta-amyloid is the key to defeating Alzheimer’s, however, and the safety of the new BACE drugs has also been a subject of concern after Lilly pulled the plug on its product due to liver toxicity.
Unlike heart disease and cancer, no major advancements have been seen in Alzheimer’s drug research since the first treatment was approved in 1993 by U.S. regulators.
Of course, the push away from the relative failure of the drug industry should not be the only reason to pursue living well with dementia.
Being disciplined and organising specialist groups to represent only the needs of persons with dementia, both nationally and internationally, will be the only way to promote living well with dementia in the current environment.
They need to ‘capture’ research grant processes, such that we know what psychological interventions work too. They need to ‘capture’ service provision design.
A problem has been the cosiness between the large charities and the Pharma agenda. It is virtually impossible now to detect and act upon material conflicts of interest.
It’s not impossible that the sheer numbers of interested people can act as one large external radical for change. A new organisation, Dementia Alliance International, holds already substantial promise for advocacy for people living with dementia. There is also monumental size of influence of ‘the Carers’ Call to Action’ from the Dementia Action Alliance in this jurisdiction. And size is power.
But I don’t really feel that it should be a competition. The risk, nonetheless, of totally ignoring persons with dementia, their friends, family, or carers, is that the more you ignore them, they more they’ll come back.
Or as Labi Saffre said, “”The higher you build your barriers, the taller I become.”
The numbers are very tight because of the venue in Camden.
Do you remember when you used to prepare Cocoa Pops cakes for kids’ birthday parties? Yes, it’s at least that level of excitement and more.
But I am now extremely excited about our private get-together to talk about issues raised in my book ‘Living well with dementia‘. Thanks to Amazon (at last), this book for the time-being is available to order for next-day delivery.
Not being invited to my private book launch, however, has absolutely no significance.
The venue is very small, and it’s been very difficult co-ordinating it thus far.
The guests are: Beth Britton, Charmaine Hardy (and sons), Darren Gormley, Edana Minghella, Gill Phillips (‘Whose Shoes’), Rachel Niblock, James Murray-White, Jo Moriarty, Lee, Lucy Jane Marsters, Margaret Kilby, Marian Naidoo, Mike Clark, Neil Chadborn, Dr Peter Gordon, Shaun Naidoo, Simona Florio, Thomas Whitelaw, Vidal Andreas, Amanda Ramsay, Gillian Nineham, Shirley Ayres, Zoe Harris, Ken Howard, Sally Marciano, Jane Samuels and Tony Jameson-Allen.
I’ve never met some of my guests, but I know them all well through Facebook or Twitter.
It has the feeling of a wedding reception in fact.
I wonder if I should get some special badges for what is effectively a #tweetup?
Indeed, I am looking forward to thanking Charmaine in person for permission to use the photography of her poppy – which was chosen by my publishers out of the ones proposed to them.
I’m also hoping Dr Mitul Mehta and family will be able to ‘drop in’. Despite being a Senior Lecturer at the world-famous Institute of Psychiatry, in their neuroimaging division, Mitul found my discussion of the problems in early cognitive diagnosis of dementia helpful. I also made him read my book recently!
I am excited that Tommy Whitelaw has accepted an invitation to come from Scotland. The distance is perhaps prohibitively long, but in any case I will be massively singing Tommy’s praises. Tommy is genuine. And he’s also a Glaswegian! An amazing contributor, who’s made a massive paradigm shift through his groundbreaking work with Alliance Scotland.
Norman McNamara, in the spirit of all good awards ceremonies, ‘can’t be there’ (the distance from Torbay is prohibitively long.) Nonetheless, Norman is recording a message on YouTube which I hope to be playing in our book launch. It’s impossible to give an account for Norman’s unique accomplishments in this area.
Not only has Norman got a huge amount of organic goodwill and love for his ‘Purple Angel Ambassadors’, but Norman has brought about a discussion on the potential merits of GPS trackers to mitigate against wandering. Whatever one’s precise views, which tend to be always sophisticated and deeply felt, this debate is much needed in my view. I am trying to make suitable arrangements for Purple Angels themselves to be represented in person.
It would be very early for Kate Swaffer to ‘Skype’-in, for Sunday morning her time in Adelaide. I am thinking of recording message by Kate especially for my guests. Kate, living with a dementia, is one of the most well liked and respected advocates for dementia internationally.
Predicting the future on the basis of your past is of course the ultimate goal of the shopping industry.
It also seems to be the goal of healthcare, as consumer behaviour and patient care appear to converge in ever-marketised healthcare.
When you ‘sign up’ for a health subscription somewhere, one day, it’s possible you’ll be offered “packages” most suitable for you. Consider them like targetted adverts on Facebook. Of course, with disease registries compiled on your behalf by public health through data sharing, tomorrow’s world is getting ever closer.
So how much of dementia is in your ‘control’, if you haven’t yet developed it?
Is prevention of dementia a pipe dream? There are, after all, many factors which we’re born with which can have a huge influence. These are known as generic factors.
Amazon, the world’s largest online retailer, is already testing unmanned drones to deliver goods to customers. The drones, called Octocopters, could deliver packages weighing up to 2.3kg to customers within 30 minutes of them placing the order. Amazon has filed a patent that will allow it to ship a package to you before you even know you’ve bought it.
To give you another example, I know someone who was being given sponsored ads for hotels in Bilboa after Facebook had picked up her location by GPS.
Now back to the past.
Back to Black in fact.
The Black report was a 1980 document published by the Department of Health and Social Security (now the Department of Health) in the United Kingdom, which was the report of the expert committee into health inequality chaired by Sir Douglas Black. It was demonstrated that although overall health had improved since the introduction of the welfare state, there were widespread health inequalities.
Modulating the environment might have some sort of impact on prevention of dementia, even if we don’t yet know how big or small this impact is.
The study of exceptionally long-living individuals can inform us about the determinants of successful aging. There have been few population-based studies of centenarians and near-centenarians internationally. But a recent study involving individuals 95 years and older were recruited from seven electoral districts in Sydney provided evidence that dementia is not “inevitable” at this age and independent living is common.
Low socioeconomic status in early life is well known to affect growth and development, including that of the brain; and it has also been shown to affect the risks of other chronic diseases.
Over a decade ago, a real attempt was made to relate early socioeconomic status to later dementia. We found results consistent with the hypothesis that a healthier socioeconomic environment in childhood and adolescence leads to more “brain reserve” (the brain’s ability to cope with increasing age- and disease-related changes while still functioning) and less risk of late-life dementia, including Alzheimer’s disease, later on.
Results from two major cohort studies, led by the University of Cambridge and supported by the Medical Research Council, have reveal that the number of people with dementia in the UK is substantially lower than expected because overall prevalence in the 65 and over age group has dropped.
Three geographical areas in Newcastle, Nottingham and Cambridgeshire from the initial MRC Cognitive Function and Ageing Study (CFAS) examined levels of dementia in the population. The latest figures from the follow up study, CFAS II, show that there is variation in the proportion of people with dementia across differing areas of deprivation, suggesting that health inequalities during life may influence a person’s likelihood of developing dementia.
The prevalence of dementia in the general population might be subject to change.
Factors that might increase prevalence include: rising prevalence of risk factors, such as physical inactivity, obesity, and diabetes; increasing numbers of individuals living beyond 80 years with a shift in distribution of age at death; persistent inequalities in health across the lifecourse; and increased survival after stroke and with heart disease.
By contrast, factors that might decrease prevalence include successful primary prevention of heart disease, accounting for half the substantial decrease in vascular mortality, and increased early life education, which is associated with reduced risk of dementia.
The study was led by Professor Carol Brayne from the Cambridge Institute of Public Health at Cambridge University. She opined that whether or not these gains for the current older population will be borne out in later generations might depend on whether further improvements in primary prevention and effective health care for conditions which increase dementia risk can be achieved, including addressing inequalities.
In fact, it has been recently appreciated that cardio-metabolic risk factors have been associated with poor physical and mental health.
An association of low education with an increased risk of dementia including Alzheimer’s Disease, the most common cause of dementia globally, has been reported in numerous cross-sectional and longitudinal studies. Education and socioeconomic status are highly correlated, it turns out.
The reserve hypothesis has been proposed to interpret this association such that education could enhance neural and cognitive reserve that may provide compensatory mechanisms to cope with degenerative pathological changes in the brain, and therefore delay onset of the dementia syndrome.
The complexity of people’s occupations also positively influences cognitive vitality, and this relationship becomes increasingly marked with age.
Further evidence from studies suggests that a poor social network or social disengagement is associated with cognitive decline and dementia.
The risk for dementia including Alzheimer’s Disease was also increased in older people with increasing social isolation and less frequent and unsatisfactory contacts with relatives and friends. Rich social networks and high social engagement imply better social support, leading to better access to resources and material goods.
Previous studies have also shown that social determinants not directly involved in the disease process may be implicated in the timing of dementia diagnosis. Possibly the living situation is related to the severity of dementia at diagnosis. If so, primary care providers should have a low threshold for case-finding in older adults who live with family or friends?
Regular physical exercise was reported to be associated with a delay in onset of dementia including Alzheimer’s Disease among cognitively healthy elderly.
In the Kungsholmen Project, the component of physical activity presenting in various leisure activities, rather than sports and any specific physical exercise, was related to a decreased dementia risk. It is generally thought that physical activity is important not only in promoting general and vascular health, but also in promoting some form of brain rewiring.
Various types of mentally demanding activities have been examined in relation to dementia in general, including knitting, gardening, dancing, playing board games and musical instruments, reading, social and cultural activities, and watching specific television programs, which often showed a protective effect.
So it really might not all the doom and gloom, and certainly we are much further forward than we were 33 years ago with the publication of “The Black Report”.
For the record, this Report doesn’t even mention dementia.
Prof Alistair Burns in New Scientist writing “Dementia: A silver lining but no room for complacency” summarised elegantly the situation as follows, on 10 January 2014:
“While it is true that there is no cure, the findings suggest that prevention is at least possible. This must surely explain any reduction in prevalence, so what might be behind it? Improved cardiovascular health, better diet and higher educational achievement are all plausible explanations. This opens up the possibility that people who are able to take control of their lives can reduce their individual risk of dementia.”
So, to answer the actual question.
There is a realistic possibility that we might be able to identify certain people who are most at risk of developing a dementia, and modifying the known risk factors constitutes ‘low hanging fruit’ for policy. If you park aside the corporate capture potential of making new markets through development of health promotion packages, this is indeed an example, shock horror, of where data sharing across the whole population might be helpful and direct the health of the nation in future.
I have been quite a good mood recently, getting ready for my book launch in Camden on the afternoon of February 15th, 2014. We’re all going out for dinner in Pizza Xpress later that evening, somewhere in Central London.
I bought my own book ‘Living well with dementia’ from Primrose Hill Books for the very much discounted price of £16.99.
This is not because it was a soiled copy, or because I was the buyer.
It was because they had ordered it in especially from the wholesalers, and managed to sell it onto me a very much reduced price.
Of course I am very grateful, as I think it’s important to support local independent booksellers in the community.
Here are the full details of ‘Primrose Hill Books’. They’re on the main road which passes through Primrose Hill. This book is called Regents Park Road.
Nonetheless, I appreciate that some people will prefer to use the bigger well known book retailers, especially if they do not time to browse or travel to such bookstores.
After a bit of haggling, we got Amazon this afternoon to reduce their delivery time from 9-11 days to fewer than 24 hours. This is of course a huge result for me. Their page on my book is here.
The Blackwells Bookstore is normally a good place to find the book for immediate delivery, but not at the time of writing this blogpost. The book is currently out of stock, but I do know reliably they had a good stock once upon a time. Here is their page.
But Primrose Hill Books will always have a special place in my heart. I’ve bought books there I’d never have ordered on Amazon, for example, through browsing.
It’s run by Jessica and Marek (and Kelly is often there too). All three have an enclopaedic knowledge of current books, some well known, some not so well known.
Of course, it was a source of great pride to see my book there. I’ve published specialist textbooks, but not the type which would look in place in the bookshop above or any other high street bookseller.
Here’s Jess looking at the book.
She said it was a good book, and we had a discussion of how long it had taken me to write (a year), how this had become a real passion of mine to share this information and to dispel all the scientific misinformation about dementia, and how it was written in the style of a long blogpost but it actually contained a lot of interesting contemporaneous evidence and discussion.
You can buy the book from the publishers’ website too.
Their is their official flier. You get 20% off if you use the promotional code ‘AUTHOR20′. You enter this code apparently just when you are completing the ‘checkout’ in this e-bookstore.
And finally, one of the people I genuinely admire the most is Tommy Whitelaw (please support Tommy at “@tommyNTour“).
You can read about Tommy’s campaign for giving carers ‘a voice’ on my blog here. His story continues to motivate me very much – and not just because he’s a Glaswegian like me!