Late on Wednesday it was announced that the decision has been taken to admit Kate Swaffer to the World Dementia Council.
Kate Swaffer is Chair of Dementia Alliance International (“DAI”), which is a leading non-profit group of people with dementia from all around the world that seek to represent, support, and educate others living with the disease. DAI is an organisation that will provide a unified voice of strength, advocacy and support in the fight for individual autonomy and improved quality of life.
Kate, from Adelaide in South Australia, was diagnosed with semantic dementia – a form of fronto-temporal dementia – in 2008 at the age of 49.
Since getting her diagnosis Kate has become a campaigner, speaker and accomplished writer on dementia issues. In January 2016, her book ‘What the hell happened to my brain?” was published, and has rapidly become a landmark contribution of a detailed account of a lived experience with dementia.
Subsequent to my being diagnosed with younger onset dementia at the age of 49, health care professionals and service providers all told me the same thing: “to give up work, give up study and go home and live for the time I had left.” On the way, it was also suggested I put my end-of-life affairs in order – even though at no time was I told dementia is a terminal illness. I was also told to get acquainted with aged care, including selecting a respite day care and residential care facility, sooner rather than later, so I could become used to it. My husband was told he would soon have to give up work to become a full-time family carer.
Very quickly I termed this Prescribed Disengagement™, and thankfully I eventually chose to ignore it. Because Prescribed Disengagement™’ is a term I came up with, I was advised to trademark it before someone else did, and hence have done so.
Kate last year was awarded a distinction in her Master of Science in dementia care from the University of Wollongong.
The statement from the Dementia Alliance International reads as follows.
“Dementia Alliance International (DAI) Chair Kate Swaffer from Australia has today officially become a member of the World Dementia Council, the second person with dementia to join this council. This is an important and significant appointment for DAI, and for people with dementia globally. She joins another DAI member, who is also Vice Chair of the European Dementia Working Group, Hilary Doxford from the UK.”
Established by the last UK government, the World Dementia Council has the stated mission to champion dementia research and development and unlock investment around the world.
Kate’s admission to the World Dementia Council is a highly significant event.
DAI has been working towards full access for people with dementia to the United Nations Convention on the Rights of Persons with Disabilities (CRPD), which is a global tool for achieving social change, this second appointment is particularly significant. Article 19 of the Convention is the right to live independently and to be included in the community. Indeed, Prof Peter Mittler is due to be presenting on this, on behalf of DAI, at the Alzheimer’s International Conference in Hungary in April 2016.
Article 29 on “participation in public and political life” enshrines an obligation for State Parties “to persons with disabilities political rights and the opportunity to enjoy them on an equal basis with others, and shall undertake to ensure that persons with disabilities can effectively and fully participate in political and public life on an equal basis with others.”
The four major prongs of the World Dementia Council’s work currently are integrated development, “optimising the path of medicines from research through to market by reducing barriers & encouraging regulatory flexibility”; finance and incentives – “looking at ways to increase the relatively low investment in funding dementia innovation by exploring new types of funding product”; open science – “unleashing the potential of open science for sharing information and knowledge to accelerate progress in developing new treatments and care approaches”; and public health/prevention – “The Council is also beginning an evidence review into existing research on how risk factors such as diabetes and heart disease relate to dementia, as well as looking into public health messaging on lifestyle and prevention.”
Even with the development of new drugs to delay the progression of the dementias, the leading cause of which is Alzheimer’s disease in the world, the need for prevention of progression of diseases through both cognitive and non-cognitive therapies will be essential. Kate’s input as a person living with dementia and as an accomplished student of dementia herself will be unique.
Err… since this photo was taken in the Hotel Adina, opposite the conference centre hosting the Alzheimer’s Disease International (ADI) conference for 2014, I have lost a lot of weight (I wish.)
But actually literally seconds before this snap was taken, Kate had said ‘you goose!’ in utter surprise when I suggested to Kate she should turn her roaming charges off. We were, of course, both in Australia, and the country of habitual residence of Kate is also Australia.
I have many happy memories of that conference, though overall I tend to be antagonistic of conferences. Most of the plenary speakers tend to be overwhelmingly underwhelming.
There are of course some exceptional speakers. I always enjoy the updates on Prof Martin Prince on epidemiology of dementia, with a focus on low and middle income countries. I know this is a complicated area, as I am sure Prof Carol Brayne from my alma mater will demonstrate in Budapest for this year’s ADI conference.
Many of the pervasive issues internationally about living with dementia also relate very much to domestic jurisdictions: including research, drug therapies, timely diagnosis, care and support, enhancing health, and dying well.
Sometimes it can be all too easy to become an innocent pawn in massive corporate agendas, which sometimes tragically reveal themselves in slick ads from ‘big charity’, raising money, but pushing stigma of dementia to do so.
I first spoke with Kate over a rather greasy lamb moussaka. Beth was there. Beth and Kate took a mutual interest in what the restaurant had to offer.
I showed Kate the manuscript of my first book expecting her to be wholly uninterested in it: actually, the opposite was the case.
Kate’s background is not straightforward. A devoted mother and wife, haute cuisine chef (trained with the best people in this field), a distinction in dementia care from a world famous University, nurse specialist in operating theatres, volunteer in bereavement counselling, and, of course, keen international speaker on dementia.
I think Kate manages to update her blog every day, and has introduced an unique term called ‘living beyond dementia‘, which sums up a positive and flourishing approach – novel and original – setting aside the negative aspects of the impact of the medical profession in imparting a diagnosis.
Kate was the first person in the world to coin the term ‘prescribed disengagement‘ which was a huge impact in the field of dementia.
As Kate says, “This Prescribed Dis-engagement(TM) sets up a chain reaction of defeat and fear, which negatively impacts a person’s ability to be positive, resilient and proactive.”
“Dementia is the only disease or condition and the only terminal illness that I know of where patients are told to go home and give up their pre-diagnosis lives, rather than to ‘fight for their lives’.”
It is all too easy to become ageist about dementia, but it is the case that dementia encompasses conditions of the age which can affect people below the age of 65. Particular considerations for the so-called ‘young onset dementia’ might include how the diagnosis is arrived at, as well as subsequent impact on real lives such as family or employment.
I personally don’t think that academics can have the moral integrity to present the full picture, when what is truly valuable and a scarce commodity is the expertise and lived experience of people living with dementia.
I think it goes further than ‘working with not for’ in fact: it is more of a question of ‘who’s in the room’ at all. I think of the co-production imperative as ensuring there are ‘no more throw away people’ as per Prof Edgar Cahn. This, as Prof Peter Mittler reminded me recently, has a parallel in the inclusivity literature as ‘No one left behind’.
And above all – it is clear people having had a diagnosis of dementia feel great comfort from the experiences of other people in similar circumstances who have reconfigured their lives accordingly. Indeed this should be the analogous to how people with physical disability are given ‘reasonable adjustments’. Whilst reasonable adjustments is a rather legalistic clunky term, it is an aspect which has been seriously lacking in the drug-focused medical model of dementia.
Kate Swaffer, not just living with a dementia, has an important narrative to tell, which is continually evolving. It is totally unsurprising that her being Chair of Dementia Alliance International (DAI), an international stakeholder group for people with dementia, has been welcomed as a huge success by Alzheimer’s Disease International.
It always seems like a marathon not a sprint, and a long one at that. I thought it was unbelievably clumsy that the World Dementia Council, a steering group on world dementia work, did not have a single representative living with dementia currently.
I indeed wrote an open letter on October 13 2014, which is on the DAI website here. I was of course ecstatic when Hilary Doxford, a mutual friend and colleague, was appointed onto the WDC, as documented here.
Kate is a world-class advocate for people with dementia, and, take it from me, a force to be reckoned with.
I received this morning my copy of “What the hell happened to my brain?” written by leading international advocate in dementia, Kate Swaffer. This book is due to be released by Jessica Kingsley Publishers on January 21st 2016. I received an advance copy as I wrote one of the Forewords. The other Forewords have been written by Dr Richard Taylor Ph.D. and Glenn Rees AM Chair of Alzheimer’s Disease International.
Kate is Chair of Dementia Alliance International, the international stakeholder group run by people living with dementia. I feel this book will be incredibly useful for a diverse audience, including doctors – especially those completing specialist training in medicine (general medicine, neurology, psychiatry, surgery especially) – as well as members of the public newly diagnosed with dementia.
I know Kate Swaffer held Dr Richard Taylor Ph.D. in very high esteem. I found the chapter dedicated to him, and his Foreword, very moving.
This book is all about living ‘beyond a diagnosis of dementia” – Kate’s phraseology TM. Kate was the first to articulate and explain the phenomenon of ‘prescribed disengagement’ how people at the point of diagnosis are often put into a process of managed decline when they could be given opportunities for an enriched life. This of course goes together with essential practical help, such as things you can do such as driving. It also explodes myths out of the water – and ignites a provocative debate on the ‘big money’ in dementia, disability discrimination, an urgent need to rework the medical label of ‘challenging behaviours’, early vs late diagnosis, stigma, loneliness, inclusion, and guilt.
It’s not hyperbolic, nor puffery, to claim that you won’t be able to put this book down. It’s an outstanding book, and I strongly commend it to you.
Many thanks to Fenella Lemonsky (@organiclemon) for this helpful review of my book in “Mental Health Today) [here is the link to the original article.]
I find reviews like this a useful steer on future work. Academics can be notorious in misjudging the ‘mood music’ of the main drivers behind the service: people who use the services, which in my case are people living with dementia, their friends and family and other carers. I am in a privileged position in having access to thousands of peer-reviewed papers, but also feel that I have learnt a lot about the dementias from people living after a diagnosis. My knowledge of dementia has vastly improved since I took myself away from the medical lens, and adopted a viewpoint of other professionals and practitioners and people living with disability.
Shibley Rahman, 2014, CRC Press, ISBN 978-1908911971, £29.99
There has been much written and spoken about dementia in the media recently as a result of the government’s Dementia Strategy, which aims to help those with dementia, their families, professionals and carers be more responsive to needs.
In this context, Living Better with Dementia, by Dr Shibley Rahman, a dementia expert who is qualified in medicine, neuroscience and law, is highly relevant.
Initially, Rahman talks about the stigma of dementia and how this has remained through the past century, despite dementia becoming better understood and having a more positive outlook in recent years. While dementia and the whole management perspective can appear a challenge as the older population survives longer, this book is encouraging and positive. Specific medication that delays the onset of dementia symptoms and other medication like antipsychotics are discussed at length, including their use in nursing and care homes and how specific practices that have no evidence base can be challenged.
Two chapters that for me stuck out as very important were on young onset dementia and on antipsychotics and innovation. Young onset dementia was first explained to me at the author’s book launch, where nurse lecturer Kate Swaffer from Australia, who has young onset dementia, gave a moving talk. The impact is huge for the individual, their family and peer network as well as professionals. It affects employment, career opportunities and has a huge stigma attached to it as it is still often misunderstood. This is all discussed in the book.
The use of antipsychotics and care homes is also discussed at length. This is an important chapter, especially for those who look after those going into residential care, and it can enable them be on alert to good practice and how to spot where medication is used inappropriately. Antipsychotics use in care homes is a complex issue. In many cases careful use can ease distress and agitation, but there seems to be concerning evidence that there is over-prescribing of antipsychotics where behavioural treatments are more appropriate. Using extensive research, Rahman explains why using antipsychotics needs careful thought.
Other chapters focus on deprivation of liberty, sporting memories, global view and leadership strategies.
This is a well-written, extensively researched, easy to read and important book for anyone interested or working with dementia.
Rating: Highly recommended.
Review by Fenella Lemonsky, mental health service user researcher
Assessing risk is a critical part of English dementia policy at all levels. I again found myself talking about risk as I saw responses to World Alzheimer’s Day which was yesterday on September 22nd 2015.
I don’t especially like the term ‘wandering’ for people with dementia. This term, like ‘challenging behaviours’ has become seemingly legitimised through the hundreds of papers on it in the scientific press, and the grants no doubt equivalent to hundreds of thousands of dollars probably. I think the term, intentionally or not, attributes blame. And as I moot in the tweet below, this is potentially a problem, especially one considers that a dementia charity should not ideally be fundraising out of sheer fear.
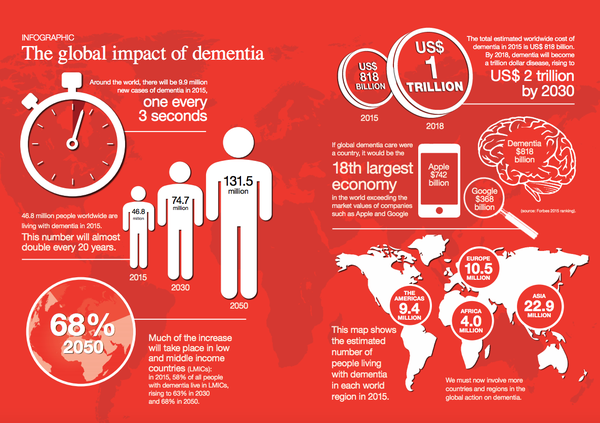
Don’t get me wrong. I think charities have an incredibly important part to play, and they do, in educating people about dementia; and generally ‘raising awareness’ howeverso defined. Take for example this helpful tweet from the Alzheimer’s Disease International containing a relevant infographic about the scale of the dementia epidemiology.
I had a hunch that something was very awry about yesterday when my colleague Simon Denegri tweeted something which caught my eye. Let me introduce you to Simon. He’s Chair, INVOLVE, NIHR National Director for Patients and the Public in Research, and, importantly, a nice guy.
The tweet, and the main subject of the research, is pretty self explanatory in fact.
The point Simon raises is worth thinking about, I feel. Is updating the epidemiology of dementia every year, nay every month, or even every week, an effective way of genuinely raising public awareness – or is it rather a lazy way to campaign on it? Obviously, playing devil’s advocate, one should argue that this main issue should be raised until something happens, but with a cure for dementia a long way distant it seems that this option is not likely.
So how about offering some solution instead? In other words, having scoped the problem, why not offer hope instead of fear through the huge volume of research in improving quality of life for people living with dementia and carers. Here’s the thing: there are 850,000 people living with dementia at the moment currently, and there’s got to be something in it for them with all this coverage.
I call fixating on the ‘tsunami’, ‘time bomb’ or ‘tidal wave’ “the shock doctrine” to make you want to dig into your deep pockets, to make you donate to a dementia charity. BUT – with social care funding on its knees, having not been ringfenced since 2010 – is this actually a luxurious response to a rather serious immediate problem? Long before #DementiaWords ‘got sexy’, I presented my poster (PO124) on the hyperbolic language used in the G8dementia proceedings, in the Alzheimer Europe 2014 conference.
Here’s the rub.
Jeremy Hughes and the Alzheimer’s Society have been hugely successful with the ‘Dementia Friends’ campaign, which has seen a roll-out of information sessions on the basics of dementia for the whole country. Yesterday was a good opportunity to talk about that.
But meanwhile Alzheimer’s Research UK, which indeed does formidable work for the research infrastructure on dementias in the UK, rolled out this in a blogpost yesterday. The phraseology of the remark, “At Alzheimer’s Research UK, our hope is for a different kind of future, one where future generations will be free of this life-shattering condition”, is the opposite to one of the central messages of Dementia Friends, that ‘it is possible to live well with dementia’.
I don’t, of course, want to downplay the huge significance of the disclosure of the diagnosis of dementia as a life event for all those involved, not least the direct recipient of that diagnosis.
All of this leads to me wonder who exactly is protecting whom? I wouldn’t go so far as to say that the public needs protecting from large dementia charities, but the sway they hold on policy is not inconsiderable; whether this is on the cure v care resource allocation in dementia, or whether there should be specialist nurses as well as dementia advisors (as I argued this year both in the ADI and Alzheimer Europe conferences).
There’s no doubt, as regards safeguarding issues, that people with dementia need to protected from risk where it is proportionate to do so. As I have long argued, you need to embrace risk to live well with dementia. But it is worth thinking about on whose part we are negotiating risk? Damian Murphy’s excellent blogpost yesterday emphasises how we cannot necessarily assume that carers and persons with dementia have the same (or even similar) viewpoints: this is directly relevant, say, on whether a person with dementia with a carer gets a GPS tracking device? (I duly anticipate and expect Damian’s contribution here, by the way, to be seminal one, by the way.)
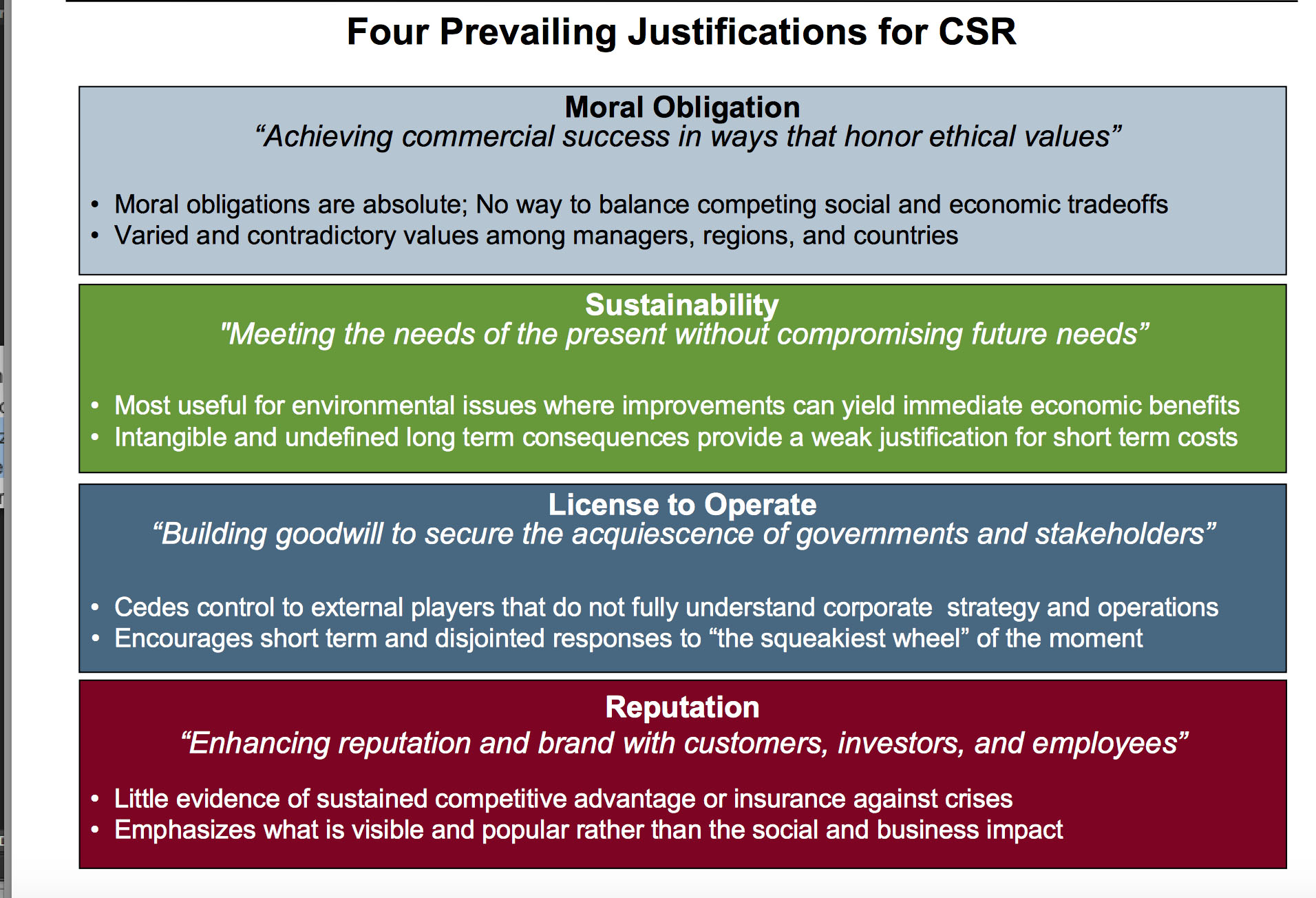
A long time ago when I was reading some of the management literature, I was really impressed by a paper to which Prof Michael Porter contributed on strategy and society (co-author Mark Kramer) in the Harvard Business Review.
Mark in a slide once summarised four crucial tenets of observing this re-articulated corporate social responsibility thus.
I, for one, would like to see all campaigning done by the dementia charities seen through this prism; and also bearing in mind the clinical, if not societal, question cui bono?
Tesco and Asda are two of the stores which have introduced ‘dementia friendly checkouts’ in supermarkets according to two reports.
Both reports refer to ‘training’ even though the Alzheimer’s Society state clearly ‘Dementia Friends’ is about information sessions, not training Both reports refer to the ‘Dementia Friends’ programme and the Alzheimer’s Society. I myself am a ‘Dementia Friends Champion’, and indeed I am due to give an information session at BPP Law School next thursday (details here).
Dementia Awareness Week was about sharing wider knowledge about dementia, rather than promoting the Alzheimer’s Society solely though the Alzheimer’s Society should be congratulated for giving the week momentum; and the the success of this, arguably, is reflected in the diversity and quality of tweets using the hashtag.
Alzheimer’s Research UK came up with an intriguing idea – the auction of hats to raise money for research into dementias. I myself know recipients of these grants, and the work invariably is outstanding. We must be keen to promote research into care as well as cure, however, and this needs the correct political lead.
Of course, by doing ‘Dementia Friends’ you’re not supposed to be “locked in” to working only as a volunteer for the Alzheimer’s Society. There is no such exclusivity requirement. And there’s no better time than now to campaign for dementia, such as the petition here against Hull Clinical Commissioning Group in their short-sighted decision not to commission Admiral nurses (a type of clinical nurse specialist for dementia).
The ‘dementia friendly communities’ policy tranche is indeed global, and spearheaded by a number of protagonists, including Innovations in dementia and the Joseph Rowntree Foundation. At a time when there is still much stigma and prejudice against dementia in society, the aim was to provide an environment which was conducive for people living with dementia, friends or families to lead fuller lives. This is, of course, a very laudable policy aim, and involves not just the health and care systems, but the wider ‘social determinants of health’ such as retail and banking, housing and transport.
It is worth at this point considering the irony of the approach of ‘dementia friendly checkouts’ in the context of the ‘Dementia Friends’ programme. One of the five key messages of this information session programme is that ‘There is more to the person than the dementia’. This was explained to me last year in Glasgow by Joy Watson as “putting the ME in deMEntia”.
The issue is that in person-centred approaches in dementia post-diagnostic care and support people aren’t defined by a label. For example, you should be very careful about the use of the word ‘elderly’. There are some NHS Trusts that define ‘elderly’ for the purposes of their acute medical take as patients above the age of 65; others above 85. And, as Chris Roberts said to me once, the differences between people aged 55 and 65, 65 and 75, 75 and 85, can be big or small. We all know 68 year olds who appear quite ‘frail’ but 85 year olds who appear quite ‘spritely’. But the issue is that, as far as commissioning is concerned in the NHS and the voluntary sector, things tend to get defined by their labels, such as new ‘million pound frailty units’. I’ve seen it before – that policy based on fashion or trends invariably ends in tears.
I think if you chat with people what they think about supermarket checkouts you will get a proportion of people who report that they’re chaotic stressful places. Many people without dementia dislike them. I in fact dislike them, not living with dementia; which is why I buy my shopping online. I also don’t know many people who meticulously count their coins in paying for their weekly shopping, so huge banners with coins may not help.
People living with dementia often describe members of the public raising the volume of their voice at them as if they’re ‘stupid’. It could be that you have problems in recognising the shapes of coins. This is called a ‘visual agnosia’. I know the late Sir Terry Pratchett described not being able to recognise a 50p coin from its shape, which is a touch form of the same cognitive condition, called ‘tactile agnosia’, which can signpost a diagnosis of ‘posterior cortical atrophy’ type of dementia.
“For some, they might struggle in a supermarket with finding the right change. That nagging voice in their head willing them to understand the difference between a 5p piece and £1 and yet their brain refusing to help them. Or they might lose patience with friends or family, struggling to follow conversations.”
Again a big banner won’t help. And for people with classical Alzheimer’s disease their long term memories will be very good as opposed to their short term memories.
A more appropriate term for examples such as the ‘dementia friendly checkouts’ might be ‘dementia inclusive communities’ – and this is indeed keeping with rights-based advocacy, where stakeholders uphold their equality (and for the time being human rights) rights under the law. But there maintains for me, and many others, this stubborn strand in policy in whether it is in fact creating inclusivity or ‘otherness’ for “people with dementia”?
“People with dementia” is a homogenous term which is not only an injustice to the hundred or so different types of dementia but also an injustice to the 47 or so million people living with dementia all with different abilities in cognition. ‘People with dementia’ are most likely to have cognitive disabilities more than ‘people with bowel cancer’, but one must be mindful of the fact one would think twice about having a special shopping aisle for people with operated bowel cancer (for people with colostomy bags).
Of course, the argument is at risk of getting utterly ridiculous. But this issue became very vibrant indeed as one of the producers of the film “Still Alice” asked the people living with dementia in a crowded lecture theatre in Perth, Western Australia, to stand up to identify themselves. The general ‘feedback’ is that this stunt was generally felt to be rather humiliating, and Kate Swaffer, Co-Chair of the Dementia Alliance International (DAI), received a number of complaints about it. The DAI is the leading international group consisting only of people living with dementia.
We are in a different place with stigma and dementia to where we were with physical disability, possibly. I am physically disabled, so I feel “within my rights” to discuss this. Many people find the word ‘disabled’ and being in a wheelchair “empowering” – many disempowering. You can take your pick as to whether people with dementia want to be identified in a separate shopping aisle in a public supermarket. But this criticism is not one which I have intended to level at proponents of ‘dementia friendly supermarkets’ – it’s simply a wider policy observation as to whether, yet again, the policy promotes inclusivity or otherness. There will be people who believe that ‘all publicity is good publicity’, but you can unfortunately have the wrong type of publicity (like the wrong type of snow).
And all this does matter if we are to bridge the lived experience of all people who’ve received a diagnosis of a dementia and what the crude policy levers are trying to achieve. I do, however, wish to thank the people behind ‘dementia friendly checkouts’ for their excellent work.
We’ve had circular discussions on ‘suffering’ before, to the point we probably agree to disagree, but have learnt to respect other people’s well meant perspectives. But I think it’s fair to say that the happiness and camaraderie which accompanied #ADI2015 is a very real one. I took this photo at a chocolate factory in Adelaide Hills. Nutrition and dementia, as it happens, was a key satellite theme of the #ADI2015.
Here’s a film by Arc Seven Communications of Beth Britton explaining the need to consider what people with dementia can do.
As it happened precisely on the day of our return, as I was travelling from Kuala Lumpur to Amsterdam, Australia aired a brilliant programme ‘Insight’ on living with dementia.
It had been a huge pleasure to have returned from spending time with Kate Swaffer, Peter Watt and Colin McDonnell who all featured in this remarkable programme. In place of fear, I felt a substantial integrity was provided by having so many delegates living with dementia attend this year’s Alzheimer’s Disease International (ADI, @AlzDisInt) conference. We met up in Perth, Western Australia, in the middle of April, for three wonderful days.
@legalaware@DementiaAllianc absolutely and it was epic to have 10% PWD in attendance! Hope that trend continues. — Dementia Advocate (@jball49) May 1, 2015
My talk was on whether dementia care would easily lend itself to private markets. I received a lot of useful feedback from delegates. I basically pointed out the problems of trying to put dementia care under the philosophy of insurance contracts because of the potential asymmetry in information between insurer and person/patient. This information asymmetry, I argued, could come from, say, a complete genetic screen, if NHS England get their way in moving towards personalised medicine/Big Pharma. The problems arise if someone with a high genetic risk for dementia seeks insurance knowing he or she is at high or low risk; or whether a person obtains an insurance policy and then behaves in a high risk behaviour. I argued that it was likely that there would need to be legislation in the English jurisdiction to protect against genetic discrimination, as in the United States.
However, I think I had most fun in the ‘poster session’, for me on Friday afternoon. I had the unexpected pleasure of chatting with Karen Harrison Dening at my session, over the need for a network of national clinical nursing specialists. As it happens, Karen has just published a brilliant book on culture and dementia, which I strongly recommend.
Thanks hugely to Chris and Colin McDonnell (@ColinMcDonnell) in helping me enormously during the poster session, which I do find stressful every time (particularly when you have curled up posters so vehemently they have no chance of sticking onto the board!)
This was for me the most interesting poster of the whole conference – on challenging behaviours, by Kate.
This blogpost explains its rationale in part. Even putting aside the general consensus that the dementias are under diagnosed in many jurisdictions, there’s a feeling that the recent scrutiny in dementia policy has overall helped.
Every 4 seconds someone in the world develops dementia. It’s vital we provide support, both now and in the future pic.twitter.com/qOURmB6IZg — ADI (@AlzDisInt) April 30, 2015
I was particularly impressed by the research presented by Prof Martin Prince on behalf of his group at King’s College London. I think Prof Prince has a clear understanding of the critical assumptions of his work, as you would expect him to have. I had a long chat with him after his lecture. He struck me as a very sincere, thoughtful man, who was open to wider repercussions of his work. In particular, we shared a common interest in seeking accurate estimates for the global prevalence of younger onset dementia.
The beginning of the conference (@ADIConference), I felt, was very surreal but pretty magical. I don’t particularly like the word ‘indigineous’ as I feel Aborigines as it can further division and divide, and I feel that Aborigines have experienced a very bad deal culturally from others exerting racial and cultural imperialism.
Here, I feel some of us must show some solidarity.
I personally bought a didgeridoo which I gifted to my mother on return (although I am mindful of the physiological limitations of the use of didgeridoo as a musical instrument by females). I was surprised to hear that didgeridoos (sic) are not permitted in hand luggage, however.
The conference itself was incredibly well organised. You can still access the book of abstracts for the conference here and wider information about the programme. I helped to review abstracts for the conference; I was indeed on the international advisory board for the conference, so reviewed abstracts for dementia friendly communities and younger onset dementia.
I am at the end of policy involved with living better with dementia, which includes advocacy across jurisdictions. I found an intense sense of hope and confidence from the conference, as opposed to the shock doctrine of Pharma which can be striking elsewhere in global policy on dementia.
The “vanguards” of dementia advocacy, globally, one may argue, are Kate Swaffer from Australia and Helga Rohra from Germany.
So it came to pass that we were all hugely proud when Kate Swaffer, Co-Chair of the Dementia Alliance International, a group consisting of people living with dementia, came to give her plenary.
I understand that videos of talks given by members of the Dementia Alliance International will be uploaded onto their website in due course.
Here’s for example Helga Rohra, Chair of the European Persons with Dementia, giving her plenary. I was deeply honoured to be name-checked in her talk. Helga is a friend, and someone whom I deeply respect.
(video from the DAI You Tube channel)
One of the plenary speakers was Al Power (@alpower12), Allen Power. Basically, I thought Al is terrific. I have now read his book “Dementia beyond disease”, which I feel is a groundbreaking reframing of the narrative towards treating people living with dementia as individuals with dignity, and how they should not be the target of pejorative language or assault through inappropriate medication.
I have known of Mick Carmody for ages. Mick has been instrumental in ‘rallying the troops’. I anticipate that his enthusiasm and focus will lead to greater things in global advocacy.
But I fell in love with Mick and his wife Sue from the moment I met them. They’d come from Brisbane, Queensland, and were hugely thrilled about participating in an international conference on dementia. Mick lives with dementia in Australia, and, it’s fair to say, had not been given sufficient or appropriate encouragement, pursuant to diagnosis. What changed the game for him was finding the Dementia Alliance International.
I am a card carrying member of the club that individuals who’ve been given a diagnosis of dementia are all unique individuals with a huge amount of experiences, and it’s not what people cannot do, as with us all, but what people can do. Here are Helga Rohra and Chris Roberts, powerful Dementia Friends Champion ambassador for the United Kingdom, as described here in the popular Alzheimer’s Society magazine “Living with dementia”.
Helga is simply larger than life, and I found many things Helga shared with me profoundly interesting. Society has come a long way, but there’s still a long way to go. Helga, I suspect, speaks up for a vast army of people who’ve been given a diagnosis as part of a large social movement, expecting dignity, acknowledgement of human rights, expecting improved employment relations post diagnosis, and calling for holistic care.
The #ADI2015 was simply triumphant for the Dementia Alliance International. I think part of this confidence has come from the new strategic alliance with the Alzheimer’s Disease International organisation, which has supported DAI, but gone to great lengths to preserve the autonomy of DAI. This brand new arrangement is described in a recent ADI “Global perspective” newsletter. Credit must be given to Kate Swaffer (@KateSwaffer) and Marc Wortmann (@marcwort), CEO of ADI, who, I feel, have been instrumental in making this vaguely possible. Thanks especially to Marc Wortmann for his kind remark about my (minimal) contribution to the #ADI2015.
It’s dangerous to underestimate how Kate Swaffer has totally altered the terrain of attitudes towards dementia, in a positive way. Kate was diagnosed with the temporal variant of frontotemporal dementia, and the personal story is well described elsewhere.
I travelled around Australia after the conference too with Chris, and I hugely enjoyed meeting John Sandblom (@jball49), Treasurer of DAI. We all basically agree John is a top bloke!
Here’s a picture of Chris Roberts, Mick Carmody and Sue Carmody having a look at the posters presenting the latest research into the dementias at #ADI2015. That #ADI2015 was successful in disseminating research to people living with dementia, comprising 10% of the delegates of the conference, I feel is a huge achievement.
I found Daniella Greenwood entirely focused on what the needs of the people with dementia in the care sector are. In the Australian jurisdiction, persons are called “consumers”. Parking this difference in terminology, the plenary given by Daniella emphasised the critical importance of relationships, and I feel this is to be broadly welcomed, in her analysis of ‘consumer directed care‘.
Chris was often to be seen manning the DAI stall in between satellites and plenaries at the Conference. But the atmosphere there was “buzzing”.
We did enjoy each other’s company. I’ve known @TruthfulKindnes (@truthfulkindnes) for ages, living with a constellation of dementia symptomatology in the United States.
One of Tru’s list of achievements has been acting like a conduit for the creative expression of many people living with dementia. She specifically mentioned, for example, the experience of visual hallucinations. Visual hallucinations can be a predominant feature, for example, of the diffuse lewy Body type of dementia, an important cause of younger onset dementia, typically with a fluctuating way of symptoms appearing.
Having witnessed Tru’s desire to promote the work of people living with dementia, and her wish to use her gift in public speaking to inspire people, I know how important it was for Tru to make it from California to Australia to promote the experience of people living with dementia.
Tru has a true gift for speaking, with perfectly modulated speech and content.
Finding this hope to encourage others is deeply meaningful. Here, for example, is Simone Willig’s film (@SWHerborn) of Helga speaking about music therapy.
This year there were some truly outstanding satellite symposia. One that springs to my mind was the one on employment and dementia. I contributed there on the need for a greater understanding of disability law by employers in terms of unfair dismissal and discrimination, consistent with Kate Swaffer’s talk there, and I urged the need for cognitive diversity in the approach from employers, resources permitting.
Research was a key pervasive theme of the #ADI2015, which took as its title, ‘Cure, care and the lived experience’. There was a keen sense of learning from each other, across jurisdictions. Again, I thank Marc Wortmann for his lead in the workshop I attended where Chris Roberts gave a powerful overview of the lived experience.
Canada, I felt, offered an useful steer in this workshop on research.
It is a remarkable testament to the solidarity amongst people living with dementia and people close to them that there’s a huge interest in dementia research; but this is, as many us feel, not just about testing new drugs like guinea pigs but a genuine interest in research in care and living well with dementia. Otherwise, in policy terms, I feel that living better with dementia becomes the ‘squeezed middle’ between prevention and the optimistic search for the cure by 2025.
I was struck too by the inclusion of social media in this narrative.
When a diagnosis of dementia is disclosed to someone, quite sadly often in a substandard manner by professionals, there is a clear impact on friends and family. I found the contributions from Jayne Goodrick (@JayneGoodrick) and Kate Roberts, Chris’ daughter, sensational, in telling delegates actually what is happening in real life.
Tru devoted a substantial part of her talk in outlining the importance of the DAI, as well as her “swiss cheese” model of dementia.
Completely by accident, I happened to bump into Glenn Rees (@Glenn_Rees), now Chair of the ADI. Everyone who has been following world policy in dementia is aware of Glenn’s remarkable steer of Alzheimer’s Australia, where he has been instrumental in promoting consumer views; and this has had a profound impact internationally on a number of arms of policy, such as campaigning against physical restraint, and campaigning against the inappropriate use of antipsychotic medication.
Chris, I felt, was a true gentleman, and very engaging as a person. I loved travelling with him in Australia, and with Jayne and Kate. Many happy emotions are brought up in thinking of what we got up to; including Chris’ use of the phrase, “That’s the kind of guy I am!”
And it was incredible to meet for the first time ‘imaginary friends’, quite safe really, such as Jac (@JacintaLynch), here in Adelaide sitting with Chris.
I don’t drink alcohol. The reasons for this are well rehearsed.
But this did not stop me in any way loving the landscape of the environs of Adelaide Hills. Australia is of course well known for famous brand names in wine, and the Barossa Valley. It, ironically, took me a journey all the way to Australia to appreciate ‘black pudding’.
The proof of the pudding was indeed in the eating.
I learnt to trust the restaurant judgments of Kate Swaffer, a pretty mean chef herself (here’s her culinary blog).
I don’t think Kate has the time to write a cookbook on top of her massive list of other commitments – but.. her work can be felt in remote areas too.
And – seriously – I have never eaten such a perfect Thai curry ever (the lower dish): cooked by Kate.
On a completely different matter, I learnt very many things in Australia; not least that kangaroos have big scrotums (sic).
And that Chris can stand very close to emus, looking as if he’s in fact eyeing them up for dinner. One thing I certainly am thankful to Mick for is explaining how emus are bloody stupid creatures.
I didn’t know what to expect from Sydney after the conference. But it turned out to be amazing – I spent time with “guess who” (Kate) and new found close friends Lynda Henderson (@yodsupporter) and Veda Meneghetti (@Veda_Meneghetti).
I have many happy memories of my time in Sydney – here are Veda (left) and Lynda (right).
Veda is fast becoming a leading global ambassador for one of the lesser known of the temporal variants of frontotemporal dementia, the logopenic variant of progressive primary aphasia. She lives with it, and retains remarkable abilities from her life as a professional musician (aside: hence explaining the need for ‘life story’).
It’s yet again a case of what people can do.
Look at this – there’s no way I can sequence rhythms as well as this.
In fact, my supervisor from Cambridge, Prof John Hodges, who also shares a professorial position with Neuroscience Australia (@NeuraAustralia) happens to be one of the leading neurological authorities on this important condition.
I was really impressed with my visit to see Prof Olivier Piguet, a mutual friend and colleagues of colleagues of mine, Prof John Hodges and Prof Facundo Manes. NeuRA, an innovative research hub in Australia, is something truly advancing the frontiers of cognitive neurology.
Whilst I did not have time to go to the Sydney Opera House (I think Kate has seen the iconic ‘Carmen’ there)..
I did have a very long chat with Prof Olivier Piguet. Olivier and I have the same strong interests in social cognition, the somatic marker hypothesis and the functions of the ventromedial prefrontal cortex, anticipation of future events, episodic memory and eating behaviours; the common link being the behavioural variant of frontotemporal dementia. This is of course what I specialised in for my PhD at Cambridge.
It is nice to be involved with promoting research in dementia, if only at a global level and not in this jurisdiction (England).
I am not, however, convinced that a US baseball cap is the best way to do this for me?
I also discovered Olivier is much taller (and wittier!) than me!
Places like NeuRA do inspire me. They should inspire the rest of the global research community in cognitive neurology too.
And Veda, it turns out, was buzzing about the work of NeuRA.
Chris, it turned out, was amazing at throwing a spear as in Aboriginal culture. He did far better than the other visitors at Uluru, but of course it wasn’t a competition. When I delicately asked Chris how he came to be so proficient at throwing spears, he explained that he used to enjoy throwing javelin in school sports. So again it’s about what you can do – and I can’t throw a spear with my chronic double vision!
Chris, a leading advocate for living with mixed vascular and Alzheimer’s disease, was pretty good at boomerangs too.
The landscape around Yulara Drive (and Uluru) was simply gorgeous. This per se of course is nothing to do with #ADI2015, but conveyed the flavour of hope and happiness that was present at #ADI2015.
Chris, Jayne, Kate and I watched Ayers Rock change colour. Jayne in fact recorded a remarkable time lapse video of this.
Chris taught me how to take photos of people; consisting of 2 eyes and 1 ear.
Ayers Rock gave us plenty of time to think about the beauty of Australia.
But we had to ease our way back to the real world in a thud, albeit via a 4.5* hotel in Sydney near the international airport.
Currently, there is quite a lot of convergence in mutual research interests. Here for example is output from Alzheimer’s Australia taking as a spotlight prevention and social determinants of health (discussed in my new book).
This was my old book ‘Living well with dementia‘ (from 2014), which I didn’t “flog” at #ADI2015 (though many were well aware of it, which humbled me.) The large poppy on the front is courtesy of, and photographed by, Charmaine Hardy (@charbhardy).
I got Kate, Helga and Al to sign a copy of my book published last year – in a completely narcissistic way (I do apologise.)
I myself met ‘virtual friends’, such as @JoanneAgnelli whose work on language and dementia is widely respected.
My new book (“Living better with dementia”) is significantly more discursive than the last one, and should be published around 21 July 2015. Thanks very much to Jessica Kingsley for publishing it. It contains a chapter on whole person (integrated) care, which is due to reach a prominence, hopefully, after the UK’s general election on May 7th 2015.
The ‘stub’ will give you a flavour of the topics I will cover.
“What do national dementia strategies, constantly evolving policy and ongoing funding difficulties mean for people living well with dementia? Adopting a broad and inclusive approach, Shibley Rahman presents a thorough critical analysis of existing dementia policy, and tackles head-on current and controversial topics at the forefront of public and political debate, such as diagnosis in primary care, access to services for marginalised groups, stigma and discrimination, integrated care, personal health budgets, personalised medicine and the use of GPS tracking. Drawing on a wealth of diverse research, and including voices from all reaches of the globe, he identifies current policy challenges for living well with dementia, and highlights pockets of innovation and good practice to inform practical solutions for living better with dementia in the future. A unique and cohesive account of where dementia care practice and policy needs to head, and why, and how this can be achieved, this is crucial reading for dementia care professionals, service commissioners, public health officials and policy makers, as well as academics and students in these fields”
And I think #ADI2015 has paved the way for this book (and my final one which will be on living at home and residential care settings in more progressed living with dementias.)
Let’s for the sake of brevity keep the definition of ‘stigma’ short – but of course it has to be attempted in some way.
Stigma, according to the current Oxford English Dictionary is defined as follows firstly.
“A mark of disgrace associated with a particular circumstance, quality, or person:the stigma of mental disorder to be a non-reader carries a social stigma.”
One of the issues about human rights is that you can’t ‘pick and mix’ human rights. You have to take the full package. You can’t buy into some, and not the others. They apply to everyone however.
In vogue at the moment is a ‘rights based approach’, but, since mooting the issue, Daniella Greenwood (who is here at the ADI Conference 2015) voiced some concern it could encourage a checklist approach.
Checklists are essentially useful, I feel, as the information in them, and can provide inappropriate totality.
Like ‘person centred care’ (the phrase that is), the operationalisation and marketing can obfuscate the real sentiment.
For example, prior to the necessary legislation, racial discrimination was lawful in South Africa, so Gandhi was the ‘boat rocker’ to use modern NHS slang.
There was nothing on the checklist about racial discrimination so notionally it was not a legal issue.
Freedom of expression is a human right, article 10 in the English jurisdiction.
It immediately for many conjures up the famous saying,
“I do not agree with what you have to say, but I’ll defend to the death your right to say it.” ― Voltaire
Along with #JeSuisCharlie and other horrific incidents, there has been further scrutiny of the wider operation of this right.
Take for example this, “The Right To Offend? Mehdi Hasan Denies ‘Absolute Right’ To Freedom Of Speech”.
” Speaking opposite Times columnist David Aaronovitch at a HuffPost/Polis debate, on the right to offend, Mr Hasan argued free speech was being “fetishized” and claimed many free-speech campaigners in the west were guilty of “brazen hypocrisy.”
“How can you construct a civilised, cohesive society if we go round encouraging everyone to insult each other willy nilly? Yes we do have a right to offend but it’s not the same as having a duty to be offensive. You have a responsibility not to go out of your way to piss people off. I have the right to fart in a lift, but I don’t do it because it is offensive.
“Some people want the right to be offensive but then get cross when people are offended.” “
There are various ways in which ‘dementia’ has become medicalised, which has supported the power of the medical profession over others in discourses, arguably. In the 1960s, warehousing of people with problems with mental health meant that drugs could be easily delivered. “Living better with dementia” in the community would’ve have been unheard of.
When Robin Williams took his own life, and who had been diagnosed with a dementia, immediately the potential for media explosion was commenced.
This subject combined two taboos – “dementia” and “suicide”.
Take for example this Daily Mail article entitled, “Robin Williams’ suicide was triggered by hallucinations from a devastating form of dementia”.
The article soon reveals,
“Court documents obtained by TMZ reveal that Williams, who was found hanging from a belt at his home in California last August, was suffering from dementia with Lewy bodies.”
Whether someone ‘suffers from dementia’ has been revisited numerous times, and I don’t intend to cover it here.
But the starting point, I feel, is that the stigma surrounding dementia goes a long way to explaining why people who have received a diagnosis of dementia don’t want to tell people about the diagnosis: sometimes called “coming out” with the diagnosis, to reflect perhaps a secret that could be hidden.
“Mental illness need not define a person as it often has in the past, but we have a long way to go to truly help those in need. Over the centuries, we as a society have ostracized, ridiculed, imprisoned, institutionalized, over-drugged, shamed, blamed, stigmatized and forgotten those who struggle with diseases of the mind. Quite unlike the history of physical ailments — which has had a distinctly different and more promising trajectory. Today we like to think we have a more enlightened view of mental illness, but countless people still fear the stigma of “coming out” with their mental health “issues” to peers and colleagues. How many among us try to hide our own struggles or those of our family members?
In the last half century society has moved away from overcrowded and often abusive mental institutions or asylums to a more humane community-based mental health approach. However, neither public funding nor insurance plans have ever provided the necessary support and resources to make such programs very effective. In fact, the lack of adequate community mental health services has given rise to jails and prisons becoming warehouses for the mentally ill in recent years. Even Minnesota faces a shortage of providers and hospital beds for those with serious mental illness as a recent legislative roundtable in west-central Minnesota revealed. And since William’s (sic) death, local media outlets such as Minnesota 2020 and MPR have been shining a light on the growing need for more mental health services across the state.”
So here we have one argument – that stigma is exacerbated by people not wanting to talk about their dementia diagnoses (“under expression”). Or, in the alternative, people feel bombarded with negative memes about dementia, e.g. “suffering”, “horrific”, “tsunami” or “time bomb”, in the general media. In any case, it can easily be argued that freedom of expression is a right that needs defending now as much as ever; it is therefore important to argue, say, freedom of expression “is the cornerstone of democracy, a vital foundation for tolerant societies.”. As this Amnesty International blogpost goes onto say, “According to the Committee to Protect Journalists, 61 journalists were killed last year in direct reprisals for their work. The most dangerous country was, unsurprisingly, Syria. Just over a week into 2015, and the CPJ’s figure is already at five. The most dangerous country? France.”
But is the content of the media something we should take some notice of?
According to Miriam Bar-on (2000), in the USA, ” based on surveys of what children watch, the average child annually sees about 12 000 violent acts,5 14 000 sexual references and innuendos,6 and 20 000 advertisements.”
Television has the potential to generate both positive and negative effects. It turns out that an individual child’s developmental level is a critical factor in determining whether the medium will have positive or negative effects. Current literature suggests that perhaps physicians can change and improve children’s television viewing habits, or even excessive television watching contributes to the increased incidence of childhood obesity?
“The term hermeneutics covers both the first order art and the second order theory of understanding and interpretation of linguistic and non-linguistic expressions. As a theory of interpretation, the hermeneutic tradition stretches all the way back to ancient Greek philosophy. In the course of the Middle Ages and the Renaissance, hermeneutics emerges as a crucial branch of Biblical studies. Later on, it comes to include the study of ancient and classic cultures.”
Kate Swaffer, Co-Chair of the Dementia Alliance International and living with a dementia, argued this recently in Dementia Journal in an outstanding paper.
“It is therefore imperative that we aspire to change views of and about people with dementia, and begin to include them in the research and conversations about them. [Ken] Clasper (2014) writes a blog about living with dementia, and said: ‘…we wish to raise awareness of dementia, is that we all live on hope, that we can in our own little way go a long way to remove the stigma which we hear of every day in dementia’.”
So this is a case of ameliorating under-expresssion of information, consistent with the notion that prejudice and discrimination arise from lack of information and/or ‘lack of changing your mind’ when presented with new information.
And Kate explains, why despite Voltaire, it is in fact a big deal to be offended,
“Whilst, we may have changed, we are all there. Whilst we may in fact suffer, many of us are not sufferers, and find that term offensive. We no longer refer to people with physical or intellectual disabilities as retarded or as retards, as it is offensive to them, even though technically they [we] are retarded. I place myself in the disabled category, as I have many disabilities caused by the type of dementia I have. Technically, people with dementia are ‘demented’ too; however, most of us find that and other terms offensive, and have a right to stand up and speak out about it.”
I have seen with my own eyes how the medical profession culturally in an institutionalised way harbour anti-dementia memes like “demented” when talking with other doctors. I’ve been on ward rounds where the Consultant has turned to junior medical staff, with the person with advanced dementia waiting to be discharged after an operation, and said, “But don’t worry about him as he’s got dementia”.
We have furthermore to be extremely careful or vigilant that the global policy of “dementia friendly communities” does not promote a sense of ‘otherness’, defeating the prime objective of inclusive.
Swaffer (2014) warns:
“The determination by governments and Alzheimer’s societies and organizations around the world to promote dementia friendly communities and dementia champions still mostly supports the ‘about them, with them’ position, which has the potential to further stigmatize people with dementia. To date, only a few people with dementia have been included in the discussions, planning and decisions about what makes a community or organization dementia friendly.”
But there’s little doubt in my mind that dementia friendly communities is a valuable concept, even if the nosology isn’t quite right?
Danielle White from Alzheimer’s Australia NSW hopes that “understanding of the condition will turn into action”, a similar if not identical to the sentiment behind the UK’s “Dementia Friends” initiative.
She has said: “These figures show why it’s so important for us all to look at how we can create communities where people living with dementia are included, respected, valued, and supported to maintain a good quality of life.”
In a paper entitled, “Dementia Discourse: From Imposed Suffering to Knowing Other-Wise”. Gail J. Mitchell, Sherry L. Dupuis, and Pia C. Kontos, this intriguing diagram pops up on page 12 which I felt was a useful summary infogram about the ecosystem of a stigma.
Venance Dey has said that, “awareness about the disease was almost non-existent in Ghanaian communities hence the formation of the AG to raise awareness about dementia in local communities that would encourage government to build systems for all those affected to have access to quality care and support they needed.”
But we should care about the age at which stigma memes might get implanted.
Psychologist Dr Jess Baker has for example in Sydney’s west observed a group of Scouts watching DVDs about dementia. The video forum is part of a UNSW-led project that aims to create a more dementia-friendly society by educating the next generation. Information gleaned from the children will be used to develop an online education program, designed to align with Australia’s education curriculum.
.“We know that children are more responsive than adults to anti-stigma education because their beliefs are not as firmly developed,” according to Dr Jess Baker.
But the impact of mass media and popular culture should not be underestimated. A group of 11–14 year olds interviewed for a British dementia study made repeated references to the “dementors” in the Harry Potter movie series – half-dead creatures that feed on happy thoughts and memories leaving their victims in a mindless state.
“Rowling, by her own account, created the dementors after a time in which she, in her own words, “was clinically depressed”. Dementors can therefore be viewed as a metaphor for depression.”
First problem – the confusion between depression and dementia. Indeed, some depression might get confused as dementia (or vice versa); but there is a co-morbidity between depression and dementia.
“Despite their attachment to human emotion, dementors seem to have difficulty distinguishing one human from another, as demonstrated by Barty Crouch Jr.’s escape from Azkaban, wherein they could detect no emotional difference between the younger Crouch and his mother.”
Having abnormal emotional responses can be a feature of the frontotemporal dementias. Indeed, Prof John Hodges from NeuRA and Prof Simon Baron-Cohen have both been very interested in how the neural circuitry involved in reading others’ minds might go awry in behavioural variant frontotemporal dementia.
“The dementors are “soulless creatures… among the foulest beings on Earth”: a phantom species who, as their name suggests, gradually deprive human minds of happiness and intelligence. They are the guards of the wizard prison, Azkaban, until after the return of antagonist Lord Voldemort.”
In popular culture, dementia is often portrayed as robbing people of their happiness.
“The presence of a dementor makes the surrounding atmosphere grow cold and dark, and the effects are cumulative with the number of dementors present. The culmination of their power is the ‘Dementor’s Kiss’, wherein the dementor latches its mouth onto a victim’s lips and consumes its soul or psyche, presumably to leave the victim in a vegetative state.”
And of course there are people like me who feel that your “Self” is not “robbed away from you” during dementia.
And finally,
“Beneath the cloak, dementors are eyeless, and the only feature of note is the perpetually indrawn breath, by which they consume the emotions and good memories of human beings, forcing the victim to relive its worst memories alone.”
Emotional regulation is affected quite late on in Alzheimer’s disease because of the usual time path of the condition, but the analogy of which memories are “robbed first” does not even correspond to actual life – in actual life, in the dementia of the Alzheimer’s type, recent memories go much earlier than later memories (the “so called temporal gradient”), and in fact worst memories might be emotionally charged such that they’re actually very vivid (a similar phenomenon happens with the effect of the stress hormone cortisol on memory formation.)
If we ‘go’ with the “rights based approach”, it’s pretty likely we’ll have to take ‘the full package’, which includes freedom of expression conversing with a person with dementia but also a freedom of expression of a person with dementia. Except…. there’s a catch here. If somebody’s acting badly with a person with dementia, it might be ‘freedom of expression’. If the person with dementia dares to say something back, it ends up being ‘agitation’, ‘aggression’ or ‘challenging behaviour’.
It essentially is a finely balanced deck of cards, where it just takes one thing to make the whole thing come crashing down.
Reading
Bar-on, M.E. (2000) The effects of television on child health: implications and recommendations, Arch Dis Child 2000;83:289-292 doi:10.1136/adc.83.4.289.
Swaffer, K. (2014) Dementia: Stigma, Language, and Dementia-friendly Dementia 2014 13: 709
We’re nearly there. Between 15th and 18th April 2015, Perth Australia will be the host for the 30th International Conference of Alzheimer’s Disease International.
If you ever an opportunity to listen to Tommy Whitelaw for an hour, do it. It’s really easy for people interested in English and global policy like to me to become obsessed with the usual macro policy details, but many people aren’t interested in macro. They want to know how the organisation of health and care systems will affect them individually.
We need to face facts. That is, there are about a million unpaid caregivers often members of a family, like a child or a spouse, in some form of care or support rôle. They do not see themselves as being labelled ‘carers’, but are fully aware of the rewarding and demanding aspects. Invariably they describe how they’ve never been given any formal preparation, just chucked in ‘at the deep end’.
It’s still pretty amazing that there are people who, despite being incredibly busy, find time to go on courses such as my friend Charmaine.
And here’s another crucial ‘issue’. I know nothing about what it is like to live with dementia, nor to care for someone with dementia. I am not a fan of the term ‘co-production’. There is, however, nothing more important than research and service provision being designed around the needs of the people who want the system to help.
I of course like the idea of ‘primary care support workers’, but I do like the idea of GPs being able to diagnose dementias more confidently (particularly differentiating the younger onset dementias, such as frontal dementia, from psychiatric syndromes such as anxiety or depression).
I like the idea of trained specialist nurses being able to get to know a person living with dementia more. I would like greater clarity of how professionals, people in a care or support rôle, and people living with dementia can work together, share knowledge and views, come to a plan while managing beliefs, concerns, expectations and conflicts. I would like this without the bubblewrap of selling “person centred care” and policy wonks, managers and politicians getting fixated with their measurement and gaming.
There will be a few highlights for me in the Alzheimer’s Disease International conference coming up. Not least is Al Power who I’ve got to know reasonably well in the last few weeks – and who seems to be one of the guys who ‘gets it’.
The programme is amazing, with lots for everyone to get their teeth into.
There are fewer things more humbling than to listen to Kate Swaffer or Helga Rohra. Of course, it is a tall ask to be able to be representative of any of the 47 million people living with dementia, but you get immediately a flavour of what these two view as important from them speaking. They want things better for other people living with dementia, and they are living in the here and now. They don’t deny making the world a better place for the future, but they want people with dementia to emerge from being hidden from view to being active people in society wherever possible.
Of course, the diagnosis of dementia itself is a big deal, and I personally feel, like Chris Roberts, living with mixed vascular and Alzheimer’s dementia in Rhuddlan Wales, and prominent Dementia Friends Champion, that more care has to be paid to preparing the ground for the diagnosis, the diagnosis itself, and what happens after the diagnosis.
And pay attention to Kate Swaffer, Co-Chair of the Dementia Alliance International, who politely queries how her investigations were done without clear explanation. I find this approach from the medics ‘underhand’, but Kate would be far too polite to say so, I reckon.
People with dementia have human rights, and it’s become accepted, sadly, for people including professionals to abuse those rights, e.g. physical restraint in residential homes.
Helga, Chair of the European Working Group for People With Dementia (with Alzheimer Europe), doesn’t refer to ‘stages’ of dementia, and I agree with Helga; ‘stages’ is a very medical term, and I have never known such clear linearity (people varying at symptoms in different presentations and rates). But whatever ‘faces’ of dementia, people with dementia and those closest to them have an inalienable right to dignity.
I’ve been honoured to have advance notice of what will be in Truthful Kindness’ presentation. That too will also be a smorsborg of creative astonishment on how one person from California has successfully inspired others around the world to live with symptoms of a dementia.
I do not deny the incredible work being done in dementia friendly communities and young onset dementia around the world. I know, because I reviewed a lot of the abstracts for the conference in these categories, being on the advisory committee for the conference.
But, above all, it’s a chance to meet up with people I like, and whose work I respect, like Simone Willig. There is a real sense of global solidarity I feel currently, including of course the traditional work being done in translationary neuroscience.
I will be looking forward to bumping into Marc Wortmann while dunking my biscuits, as usual; and I look forward immensely to meeting Glenn Rees, the incoming elected Chair elect of Alzheimer’s Disease International.
I reckon I’m all set – I’ve only got this far in organisation for this ‘trip of a lifetime’, thanks to Jayne Goodrick.
“Urgent” and “call for action” have become the potent memes in messaging radical transformative change. Hence the title of the statement about the #globaldementia event, held earlier this week in Geneva, came as no surprise to me. What did genuinely come as a surprise was how accommodating both WHO and the Alzheimer’s Disease International were to the views of people with dementia there.
This was the public image; rather reminiscent of GCHQ, an omniscient and omnipotent body talking to each other. And indeed I found the communication between officials between different countries useful, even some still clung onto the deeply stigmatising language such as ‘horrific’ and ‘devastating’.
The word though ‘urgent’ does merit some scrutiny. It implies that time is running out – and indeed Hillary Doxford, the representative of the World Dementia Council living well with dementia, explained that “time is the currency of people living with dementia”. Hillary herself explained how she was only given a finite length of time to live, according to her initial disclosure diagnosis. And this is not the first time that I have heard this issue being totally mishandled. The actual truth is that it can be very difficult to predict how long a person will live, and actually imparting a diagnosis of dementia should not bring that person any closer to their time of death. In fact, ideally, we want to be able to get to the stage where most people, after a diagnosis of dementia, are able to ‘live better with dementia'; and indeed initial evidence appears to support the notion that active social networking or even diet may have a beneficial effect. But Kate Swaffer brought out a point which I do feel is urgent; that high quality research into care and living better with dementia needs to have parity as that sort of research which ultimately yield a ‘cure’. The ‘experts’ this week had enormous difficulty in identifying what a cure for dementia might look like, and this is not surprising given that there are about a hundred different types of dementia.
We didn’t hear much from caregivers themselves at the conference, which is not unexpected given what a full time job caregiving is. The “call for action” this time around. “Call for action” has become the call for arms for charities campaigning on dementia, but it is becoming increasingly clear that self-generating social movements campaigning for a change in how dementia is perceived by others is gathering considerably more momentum than the ‘dementia friendly communities’ construct. ‘Dementia friendly communities’ should not be underestimated for reframing aspects of communities around the needs of people in society with dementia to lead fulfilling independent lives, but it remains dangerously close to a “does he take sugar?” modus operandi. Even the “no decision about us without us” mantra assumes division of “them” against “us” – which led me to do my own personal #globaldementia pledge this time around.
I am looking forward to participating in an event hosted by the Mental Health Foundation on 26 March 2015 entitled, “Rights, dementia and the social model of disability: a new direction for policy and practice?” I must admit that I was expecting to be somewhat at odds with this report, but I found it spot on. I’d therefore like to extend my personal thanks to Gráinne McGettrick, members of the project Advisory Group, 26 March speakers and participants, especially people living with dementia.
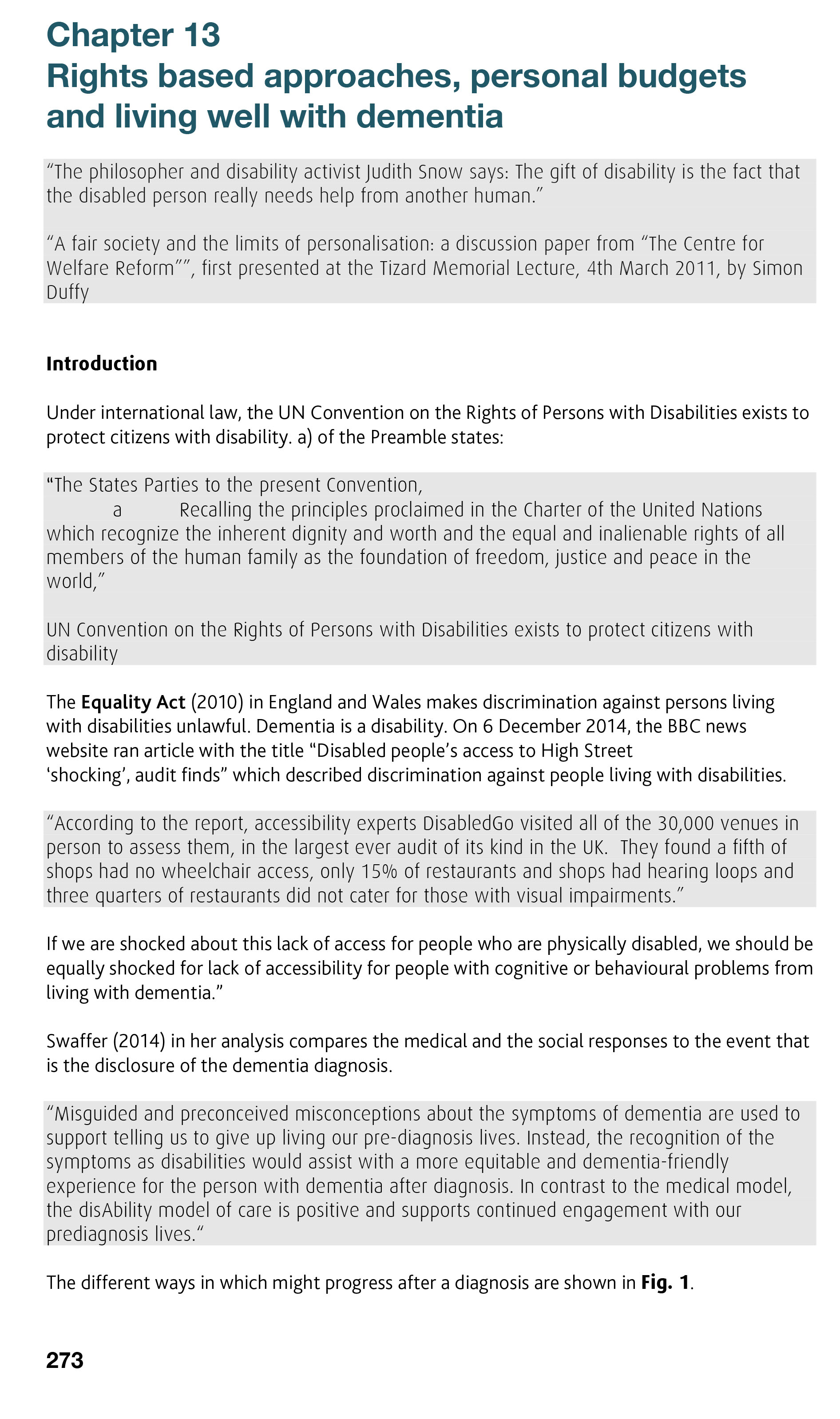
The document is very much in keeping with chapter 13 of my book “Living better with dementia: Good practice and innovation for the future”, with three forewords having been written by Kate Swaffer, Co-Chair of the Dementia Alliance International, a ‘peak body’ of people living with dementia, Beth Britton, celebrated blogger and campaigner, and Chris Roberts, living well with dementia. The narrative of my book is ambitious; it basically puts people living with dementia, with an aspiration to live better, ‘in the driving seat’, and argues for a rôle for an individual who has received a diagnosis, a member of family or friend, and professional to take part in an extended network to help to deliver a personalised care plan. In chapter 13, I found myself confronting the rather individualistic approach of human rights, being reconciled with the ‘dementia friendly communities’ policy currently in vogue worldwide.
For me the Mental Health Foundation report throws up a number of critical policy issues which will need to be confronted sooner or later. I suggest sooner; perhaps even I suggest ‘urgently’ with a similar ‘call to action’?
The issues for me are as follows.
1. Definition of dementia under English law
The guidance for the Equality Act (2010) helpfully includes dementia as a disability. The case law, I feel, is more helpful than the statute law.
For the law, the link between ‘disability’ and ‘impairment’ is a key one Section 6(1) Equality Act [2010] states that a person (P) has a disability if P has a physical or mental impairment, and the impairment has a substantial and long term effect on P’s ability to carry out day to day activities.
In essence, the claimant must therefore show that there is an impairmen, the impairment has an adverse effect, the adverse effect is substantial, and the effect is long term.
Not all of the points have to be proved, and it has generally been accepted that claimants living with cancer, multiple sclerosis, or HIV/AIDS will have no problem in fulfilling this statutory definition. The legal issue is how a medical condition affects a person ((e.g. mobility, manual dexterity, co-ordination, continence, ability to lift/carry, speech, hearing, eyesight, memory, ability to learn, perception of risk or physical danger).
The medical model requires the clear identification of deficits; whereas the social model, one which people themselves with dementia tend to prefer, looks at what people can do rather than what they cannot do. Arguably, attending a medical ‘check up’ which emphasises what you cannot do now compared to before, or brain shrinkage on your MRI scan, can be very demoralising and not particularly constructive for a person living his or her life.
How the impairment is caused is irrelevant in English law, and we know this from Power v Panasonic UK Ltd [2003] IRLR 151, a case decided under the Disability Discrimination Act. There are possibly as many as hundred different types of dementia, and they all present with different ways, although it is certain that no two people living with dementia present the same. This calls into sharp focus of questioning what the point of the label is – such as the diagnostic category of dementia. In ‘diffuse lewy body type’ of dementia, certain medications are best avoided. Whereas dementia of the Alzheimer type typically is best characterised by early difficulties in learning and memory and spatial navigation, semantic dementia is best characterised by loss of specific types of knowledge, posterior cortical atrophy is best described as loss of higher visual processing early on, and behavioural variant frontotemporal dementia is most often characterised by an insidious change in personality and behaviour in the absence of cognitive deficits early on observed by others.
2. The enforceability of the law (access to justice)
Having an emphasis on the law is great to bolster that this a serious issue, rather than the more namby pamby softly softly approach of ‘dementia friendliness’. However, the usual criticisms of using a legal approach in my opinion apply; adherence to the law without a genuine change in cultural attitudes, a possible ‘race to the bottom’ with more enthusiasm about compliance than outcomes-focused regulation, or a sheer lack of enforceability due to drastic cuts in legal aid provision. In England, there has been quite savage cuts here consequent upon the Legal Aid and Sentencing and Punishment of Offenders Act (2012), which some rightly view as a demolition of the ‘welfare state’. One could and should argue, perhaps, that access to justice should be a necessary and critical part of a dementia friendly community?
3. The lack of cultural diversity considerations
The rights based approach is technically worthy of the same criticism as ‘dementia friendly communities’ in that in the drive to universal concrete individual rights there is little consideration of the cultural background of the person living with dementia (e.g. BAME communities, LBGT communities). But human rights by their nature are supposed to have a non-negotiable, inalienable fair about them, a universality which can be relied upon, so this may in fact be an advantage rather than a criticism. However, it could be argued that ‘dementia friendly communities’ offers a much more culturally-sensitive tool than rights-based approaches (see for example Dementia Friendly Gurudwaras).
4. Are rights and capacity connected?
The recent R v Cheshire/Chester case has brought to the fore the precise inalienability of human rights, which cover a mass of issues such as liberty, even if a person is legally without capacity. There is a broad consensus that a human person should not lose his or her human rights if he or she loses capacity, but this prerequisites a robust definition of capacity, which many feel we have simply not arrived in the current English jurisdiction (nor a consensus on the best way to implement the Mental Capacity Act (2005)).
5. Institutional vs ‘successful living’
Across the last few decades there has been a general move away of institutionalising people with mental health conditions including learning difficulties and dementia. There is nonetheless a tension which does interface with the ‘rights based’ approach and disability activism, in that people who are not able to live alone should not be deemed as ‘failures’ of policy.
6. Does the United Nations Convention of Rights for People with Disabilities inform on what might constitute a dementia friendly community? (e.g. enjoyment of sport)
The legal definitions under the United Nations Convention for Persons with Disabilities, as pertaining to dementia, are indeed interesting, as they refer to specific things such as enjoyment of sport. Of course, prescribing such a list lays the Convention to the attack of “expressio unius est exclusio alterius“, that only things specified n the list are worthy of consideration.
But they do potentially offer the basis of minimum legal standards for a dementia friendly community which could even be legally enforceable (in theory), such as article 30 (participation in cultural life, recreation, leisure and sport). Actually, I am quite interested in article 29 (participation in political and public life), which emphasises that the same democratic principles should apply for people with dementia. There was in fact a clear violation here, as the current nominee for the World Dementia Council, living well with dementia, was not democratically elected.
7. Implications for needs assessment under the Care Act (2014) in the English jurisdiction
The phenomenon that some people with dementia “have good days” and “have bad days” is well known not least to people with dementia and caregivers themselves. In certain types of dementia, such as diffuse Lewy body dementia, it is not unusual for cognitive performance to be ‘fluctuating’. The traditional description of ‘multi-infarct dementia’ (or ‘post stroke dementia’) has been of a ‘stepwise’ progression, although many have queried the correctness of this term.
Whatever the precise details, it is generally accepted that the needs of a person with dementia will change, not least because dementia, whatever the precise nosological definition, is considered to be progressive (unless the symptoms of dementia present from causes other than dementia or the dementia is ‘reversible’ e.g. plasma exchange for paraneoplastic dementia). This poses a critical question as to how rights are related, if at all, to the fluctuating symptoms of dementia? This logistically poses an issue of how often needs should be re-asssessed and how such ‘results’ are interpreted by professionals. Ideally, the benefits system linked to the Care Act (2014) regulations needs to be responsive to the care needs of any individual with dementia at any particular place and at any particular time. This certainly warrants careful scrutiny.
8. Shift from a medicalisation to a social model (rôle models, development of a cure, training of workforce)
This is of course is THE big one in England, requiring a huge radical transformative change in England, combining health and care.
This requires breaking down organisational silos, different funding schemes, different power structures, different workforce requirements, different cultural attitudes, the breaking down of barriers of information transfer, a more collaborative or distributive style of leadership, better coordination between different forms of care and health provision, the double declutching from a fragmented illness repair service to a national health service. The change required is enormous.
I have always believed that political leaders or CEOs of big charities do not hold the key to bringing out ‘urgent change’. And here you really have to define what change one is trying to bring about. Even the mantra “care for today, cure for tomorrow” has brought about division, as people have asked, “why not care for tomorrow as well?” Kate Swaffer, Co-Chair of the Dementia Alliance International, has warned that there is no imminent cure in the pipeline, so there is a genuine issue of expectation management. How are even the most altruistic of the 45 million people living globally with dementia supposed to get excited about a cure or Big Data advances in dementia for 2025?
Very difficult, if you’re being honest.
I believe rôle models, of people living well with dementia, such as Ken Howard, Kate Swaffer, Chris Roberts, Mick Carmody or Helga Rohra, hold the key here. They are THE authentic voice – to tell the organisers of the health and care services what is urgently needed from them, e.g. not 15 minute disclosures of diagnoses in the absence of loved ones with reference to an information pack in a busy clinic.
9. The power of the media
For all the efforts of destigmatising dementia, it is helpful if you have leaders in WHO or political Ministers of State calling “dementia” incessantly “horrific” and “devestating”. Nobody of course is asking for the negative aspects to be airbrushed out, but all most people want is some form of balance rather than ‘shock doctrine’ tactics. The stronghold of the media is not inconsiderable, especially if people with dementia are themselves to give birth themselves to a social movement, but here the tools of the new media, such as Facebook or Twitter, might help. One suspects that principal media outlets should be given much more stringent guidance on what is acceptable, and what isn’t.
10. Effective rehabilitation
Kate Swaffer herself noticed that ‘rehabilitation’ was noticeably absent from many if not all discussions. Why? Kate raised the point that if she had been given guidance on how to adjust to her diagnosis, on what she could do rather than what she could not do, she might have been able to carry on paid employment. Many people with dementia do not wish to take their employers to court over unfair dismissal, as that is a sure fire way to bring about a break down in employer-employee relations. That is an example where implementation of legal rights might bring about more damage than good. For many having received a diagnosis of dementia, effective engagement with the society and community is more beneficial than a lump sum payment from the employer, as we keep on being told in policy (because it is true) that marked loneliness often accompanies the diagnosis of dementia in all jurisdictions.
11. What is the end point? Equality versus diversity.
There is a sense that we do not actually know what the end point is for anything. We don’t even know what the end point for the cure for 2015 is, as we don’t have a coherent explanation of that despite numerous requests. Kate Swaffer suggested that a cure which gave somebody a protracted slow death might not be ideal either. And the “dementia friendly communities” policy is fixated on equality, not diversity, which means that even if both rights-based approaches and dementia friendly communities were implemented to the hilt across all jurisdictions to the hilt the policies would clearly not satisfy everybody because of individual differences in diagnosis and service provision.
12. Are the services in place which do not inadvertently encourage division?
Even the most professional professional this week confused dementia with a condition of ‘old age’. I have had this dispute with Kate Swaffer. In fact, we both agree. Many old people live with dementia. As you get older, your risk of getting dementia increases. But there are many younger people with dementia too. We haven’t reached a point yet where points of service provision are not ageist, and therefore immune from judicial review. How far do you take rights? I’ve asked Chris Roberts whether he feels that old people’s homes are appropriate for younger people with dementia, and Chris reliably tells me that he has not intrinsic difficulty into going into a home with older people as he loves meeting people (also telling me that the difference between 45 and 55 should not be given greater attention than the difference between 65 and 75).
13. Is involvement of charity a good thing? (Problems to do with corporate and regulatory capture; does involvement of “charity” inadvertently reinforce a ‘victimhood’ nature of living with dementia?)
The system is clearly geared up to reinforce the medical model; you can see the way possible cures for dementia are promoted by certain corporate-like charities; and this is reinforced by the regulator such as NICE setting rigid guidelines for such interventions (such as cholinesterase inhibitors) with less attention to say the potential of an iPod to improve the quality of life of a person with dementia through ‘musical therapy’. The cost of distributing iPods may be more ‘cost effective’ value-wise for improving quality of life of people living with dementia than medications which do not, for most, slow down progression nor have a beneficial effect of symptoms further to a very limited time window for some? Surely this is the sort of discussion we need to be having, as well as the ones we saw at #globaldementia? The time may have to come where large charities are recognised more as being as the problem than the solution, particularly if they appear to dismiss calls for a national network of clinical nursing specialists in dementia.
My somewhat reluctant conclusion is that rights-based approaches put people with dementias on a much firmer footing, and this cannot be a bad thing. However, my concern with this approach is that whilst right-based approaches appear fine in theory how they are actually implemented in real life which provide the acid test.
The national minimum wage sounds great, but…
Furthermore, one wonders whether the notion of living better with dementia rests easily with the concept of ‘victimhood’ which can inadvertently encroach on work.
Take for example, this recent section from an article from Norman McNamara’s Kickstarter to make a documentary about him and his initiatives:
“He added: “The Purple Angel Dementia Awareness Campaign has now become global and is being embraced by all four corners of the world.
“People who matter have come together for one cause – to help those less fortunate than themselves.”
It is unclear to what extent certain people with dementia are happy with this ‘victim status’ portrayed by others?