The general starting point is that risk taking is essential for innovation to succeed.
“Forbes” magazine recently put it this way:
“Risk taking is not about being foolhardy. The innovation risk-taker brings good judgment and self-awareness to everything, but understands that there is a point – just there, beyond the safe, beyond the secure – where there are disproportionate rewards. In any organization, there are plenty of fumbles, missteps, train wrecks, and failures. But these are less the result of risk-taking, and more of ineptitude. Look for the places in your organization where there is lots of homework being done, lots of direct, plainspoken conversation and a strong sense of fun, and you’ll find the risk-takers there. Risk-takers resist the temptation of the status quo and continuously push organizations into new – and quite possibly innovative – areas.”
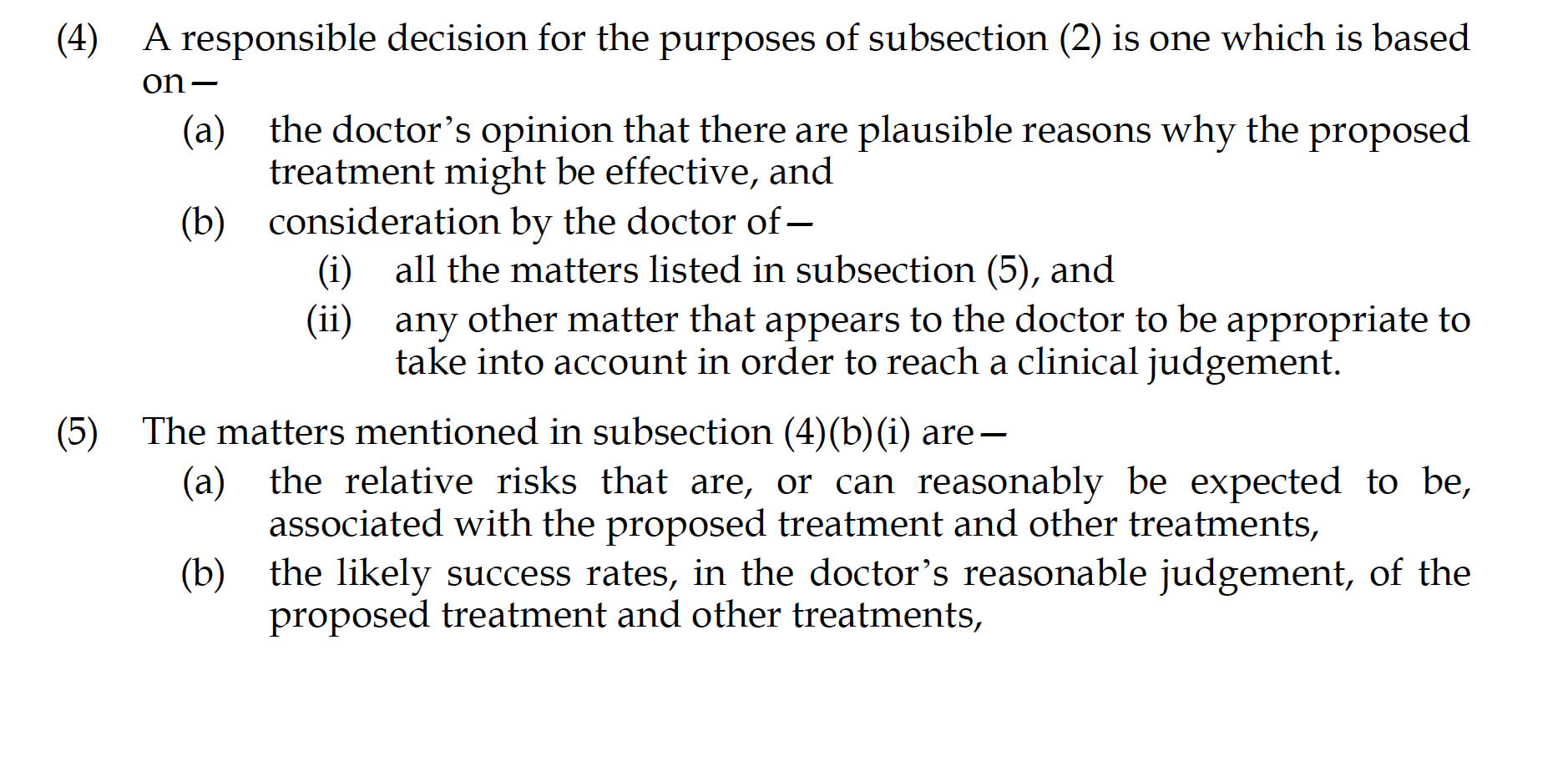
The Medical Innovations Bill [2014] has been published as follows:
The regulatory underpinning is clear.
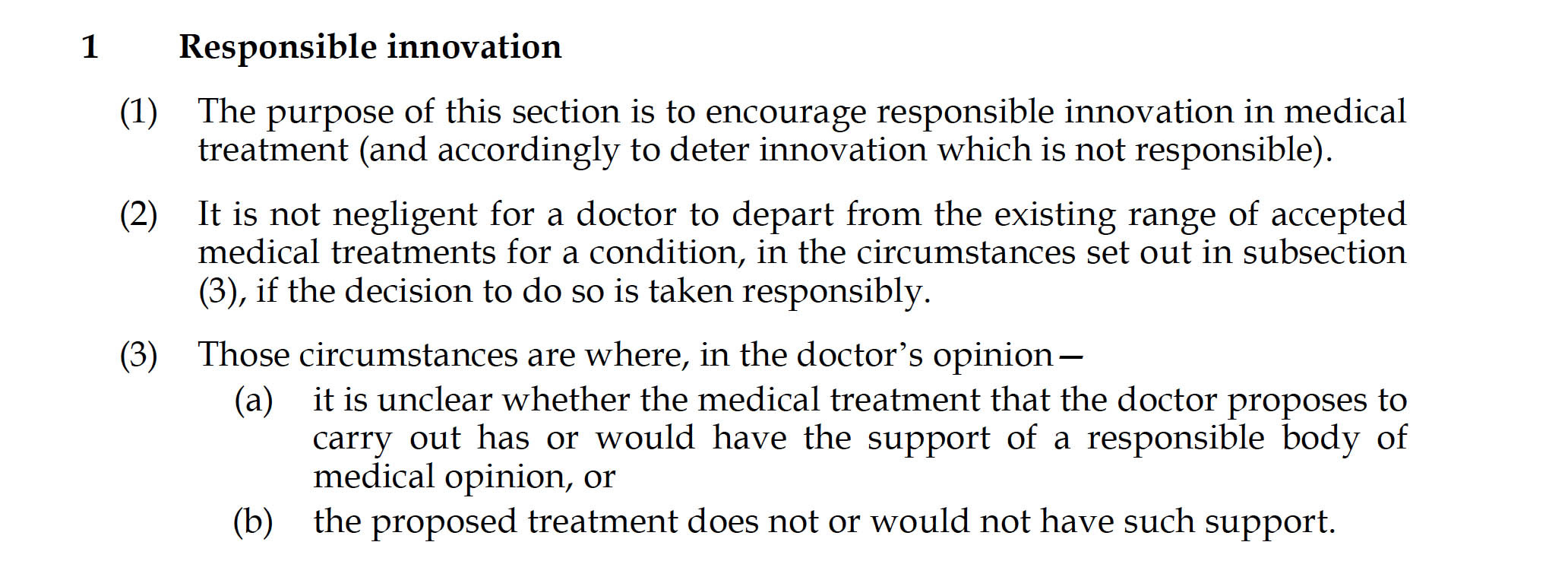
And so are the caveats.
Risk taking and patient safety have always been two conflicts for the medical profession.
A central ethical (and professional regulatory) tenet is ‘primum non nocere‘ – at first do no harm.
The question is partly a question of semantics: can a physician expose to a patient to some degree of harm knowingly, or can a physician expose a patient to that harm recklessly? And should the law or regulators stop this? The General Medical Council has of course a statutory underpinning in the s.1(1) Medical Act [1983] to promote patient safety – this is unambigious.
Part of the problem is that it can be in real life to ascertain what precisely is the degree of harm which can be exposed. For example, even with the most ‘simple’ of scenarios, it can be difficulties to work out what proportion of patients have had ‘significant’ side effects of common medications such as high cholesterol ‘busting’ drugs such as statins.
A further problem is how the regulators deal with the issue of whether it is permissible to allow common side effects of rare drugs compared to rare side effects of common drugs.
And rare drugs can be used to ‘treat’ common conditions.
Of the 800,000 people living with dementia, it is uncertain how many people will want a medication to put a complete stop to a dementia illness, though one could have a good guess.
Conceptually, it’s also difficult to ascertain how many people will want a dementia illness to be slowed down but there would still remain a degree of inevitability about the condition.
And yet a further complication for this, for dementia, is that people with dementia legally might lack capacity – formally lack the lgal ability to make ‘competent’ decisions.
The “Bolam test” has always been highly significant for the clinical negligence experts.
Bolam v Friern Hospital Management Committee [1957] 1 WLR 582 is an English tort law case that lays down the typical rule for assessing the appropriate standard of reasonable care in negligence cases involving skilled professionals (e.g. doctors): the Bolam test.
Where the defendant has represented him or herself as having more than average skills and abilities, this test expects standards which must be in accordance with a responsible body of opinion, even if others differ in opinion. In other words, the Bolam test states that “If a doctor reaches the standard of a responsible body of medical opinion, he is not negligent”.
Meanwhile, for the Judiciary, the case Simms v Simms and Another/A v A (A Child) and Another, Family Division from 17 December 2002 [2002] EWHC 2734 (Fam), [2003] Fam. 83, in front of Dame Elizabeth Butler-Sloss P is a pivotal one.
In the judgment, Butler-Sloss notes that:
“48 To the question: “Is there a responsible body of medical opinion which would support the PPS treatment within the United Kingdom?” the answer in one sense is unclear. This is untried treatment and there is so far no validation of the experimental work done in Japan. The Bolam test ought not to be allowed to inhibit medical progress. And it is clear that if one waited for the Bolam test to be complied with to its fullest extent, no innovative work such as the use of penicillin or performing heart transplant surgery would ever be attempted: see Lord Diplock in Sidaway v Board of Governors of the Bethlem Royal Hospital and the Maudsley Hospital [1985] AC 871, 893. I do, however, have evidence from responsible medical opinion which does not reject the research. Mr T is a very experienced and clearly very responsible neurosurgeon. He has carefully thought through at considerable length in his two reports, the research, its implications, the uncertainties, the risks and the doubts about the benefits to these two patients. He has come to the conclusion that “it is in the best interests of [JS and JA] to be treated and I would personally be prepared to carry out that treatment”.
The comment ‘per curiam‘ runs as follows:
“The Bolam test ought not to be allowed to inhibit medical progress since it is clear that if one waited for that test to be complied with to its fullest no innovative work in medicine would ever be attempted (post, para 48).”
Iain Chalmers and Lester Firkins of the James Lind Initiative, Oxford, n a letter to the British Medical Journal on 23 April 2014 wrote as follows:
“We have direct experience of the adverse consequence of an important omission from Judge Butler-Sloss’s judgement.”
“We co-chaired the MRC Prion-1 trial steering committee at the time (17 Dec 2002) that the father of a young man with variant Creutzfeld-Jakob Disease (vCJD) appealed to the High Court for permission to seek treatment for his son using pentosan polysulphate injected into the brain. The father believed that the drug might slow his son’s decline because it appeared to have done this in an animal model of the disease studied in Japan. Judge Butler-Sloss granted permission for the father to seek treatment for his son, and similar judgements were made subsequently in respect of other sufferers of vCJD.”
“In making her ruling Judge Butler-Sloss suggested that treatment with penicillin might never have been attempted if the Bolam principle had been applied. What she failed to do was to require organised, prospective documentation and publication of the characteristics and progress of patients receiving pentosan polysulphate for vCJD, as had happened with the first series of cases treated with the penicillin. The consequence of this important omission from her judgement has been that patients, their parents, and the people involved in the PRION 1 trial and other related research remained and remain unnecessarily ignorant about the possible benefits and harms of this proposed treatment.”
And the ‘degree of risk’ is important according to previous case law.
In, for example, Sidaway v Bethlem Royal Hospital Governors [1985] AC 871, the material facts themselves are very interesting.
The claimant suffered from pain in her neck, right shoulder, and arms. Her neurosurgeon took her consent for cervical cord decompression, but did not include in his explanation the fact that in less than 1% of the cases, the said decompression caused paraplegia. She developed paraplegia after the spinal operation.
Rejecting her claim for damages, the court held that consent did not require an elaborate explanation of remote side effects. In dissent, Lord Scarman said that the Bolam principle should not apply to the issue of informed consent and that a doctor should have a duty to tell the patient of the inherent and material risk of the treatment proposed.
Crucial to all this, “it’s the consent stupid” – but here the law is complicated for anti-dementia drugs for people whose dementia symptomatically is advanced sufficiently such that individuals lack consent (and may have to have decisions made in their best interests).
The relevant clause is s.1(8):

In the first ‘Google Talk’ ever to be held in the House of Lords, a panel featuring Max Pemberton and Lord Saatchi includes opinions such as how patients with only six months to live, whose chances of survival, are quite desperate to try any treatments, even if they have a low chance of success.
This is not an insignificant argument.
Specifically, do the GSK-3 inhibitors ‘offer a ray of hope‘ for people with dementia?
They’re ‘new kids on the block’ which might “stop dementia in its tracks”.
The biochemical problems with this class of drugs are elegantly described by the authors:
“The main disadvantages of the first group of discovered GSK-3 inhibitors were their lack of selectivity and the competition with ATP for its binding site. Apart from GSK-3 inhibition, these compounds were able to inhibit other kinases such as CDK1 or CDK2. Although the lack of selectivity is a disadvantage in the development of a potential AD therapy, the therapeutic application for the treatment of parenchyma renal diseases of CDK/GSK-3 inhibitors have been recently described. CDKs and GSK-3 have been recently recognised as key players in the progression and regression of many kidney diseases.”
And the authors couldn’t be clearer:
“However, typically, there are two major concerns for the clinical use of GSK-3 inhibitors for chronic treatments such as that required for AD. First, since GSK-3 plays important roles in so many tissues, the risk of severe side effects is present.”
But put yourself in the shoes of the person with a dementia who might be a candidate for such a drug, in the early stage of the dementia, who has legal mental capacity.
Would you knowingly like to take the risk of taking a drug that could stop your dementia and give you a massively improved quality of life, or would you like to take the risk of having the drug ruin your life forever cutting short any quality of life by many years?
My concern is that neither the medical nor the legal profession have the sufficient expertise to make such tricky ethical decisions.
I once remember the brilliant LJ Laws talking about the difficulty for senior Judges if they wished to impose ethical moral judgments on their complicated legal judgments to do with social justice.
That comment has made a longlasting impact on my view of the law, in fact.
And yet my gut instinct is to refrain to think about innovators on the fringe of wackiness and insanity.
I once had the honour of meeting Dr Walshe.
I remember looking up his paper on penicillamine, in the late 1960s, in the library of the National Hospital for Neurology nad Neurosurgery at Queen Square. This paper uniquely was proposing a novel innovation in therapy for Wilson’s disease, an inherited problem with copper metabolism which if unchecked could cause liver cirrhosis or dementia.
I met him in fact at the Royal College of Physicians at a meeting on orphan drugs in medicine.
Anyway, I look forward to resolution of the legal debates to do with medical innovation. I understand that the General Medical Council will simply wish members of their Register to uphold the law whatever that is in the future. The problem of course comes if the case law conflicts with the staute law even negligently or innocently.
