One amazing phenomenon is that it’s possible to stimulate memories in people living with dementia by the presentation of football memorabilia, as described by Rachel Doeg here.
The transformation is quite remarkable: “reeling off expert knowledge and sharing collective memories that bring laughter and camaraderie to the group,and a boost to their self-esteem.”
“Bill’s story” is another brilliant example from “Sporting Memories“:
“Sporting memories” was established to explore the stimulation of living well in people with dementia, through conversations and reminiscence.
The Dementia Friends programme supports people who want better to understand all the implications of the condition. Last week saw celebrities and people living with dementia teaming up with the Dementia Friends Campaign to encourage even more of us to sign up. It is hoped that one million will be recruited by 2015.
One of the ‘talking points’ in ‘Dementia Friends’ might “the bookshelf analogy of Alzheimer’s Disease”.
This video taken from the “Dementia Partnerships” website shows Natalie Rodriguez, Dementia Friends Champion, using this analogy to describe how dementia may affect a person.
This simple explanation, orginally devised by Dr Gemma Jones, can be helpful for Dementia Friends Champions to explain dementia to others. A full description of it is given here.
The usual explanation of the early features of Alzheimer’s disease using the ‘bookcase analogy’
In this analogy, the brain has a number of ‘bookcases’ which store a number of memories, such as memory for events about the world, memory for sensory associations, or emotional memory, to name but a few.
Let’s now focus on the memory for events about the world bookcase.
The top shelves contain more recent memories, and, as you go down the bookshelf, more old memories are stored.
When you jog this memory shelf, the books on the top may wiggle a bit, causing minor forgetfulness about recent events, such as where you put your keys.
As you jog it a bit more, the books on the top shelf may fall off altogether, making it impossible to learn new stuff and retain stuff for a short period of time.
The bottom shelves of the short memory bookcase remain unperturbed.
The jogging of this memory for events about the world bookcase is equivalent to what happens in early Alzheimer’s disease, when something goes wrong in the top shelves only.
The top shelves correspond to the hippocampus part of the brain – it’s near the ear, and so called as it looks like a sea-horse. That’s where disease tends to happen first in Alzheimer’s disease.
So you can see what happens overall. In the early stages of Alzheimer’s disease, a common cause of dementia, problems in short-term memory for events about the world can be profound, while long-term memories around the world are relatively infact.
As they correspond to different bookcases altogether, sensory and emotional memory are left relatively intact.
How the ‘bookcase analogy’ can be used to explain the phenomenon of “sporting memories”
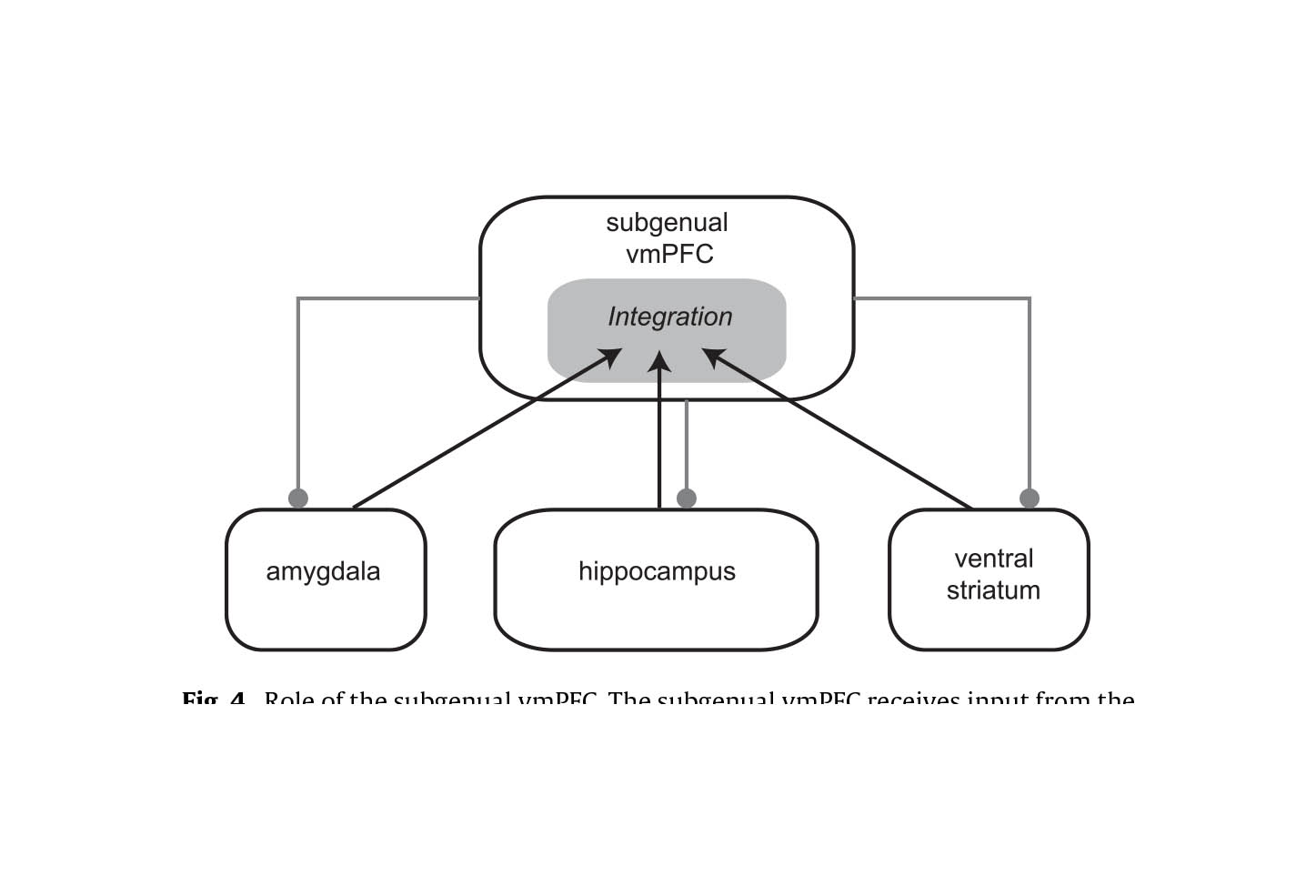
I haven’t mentioned another bookcase altogether. This is a memory of events about yourself – so-called “autobiographical memory” – and this is held in a part of the brain by the eye (the ventromedial subgenual cortex).
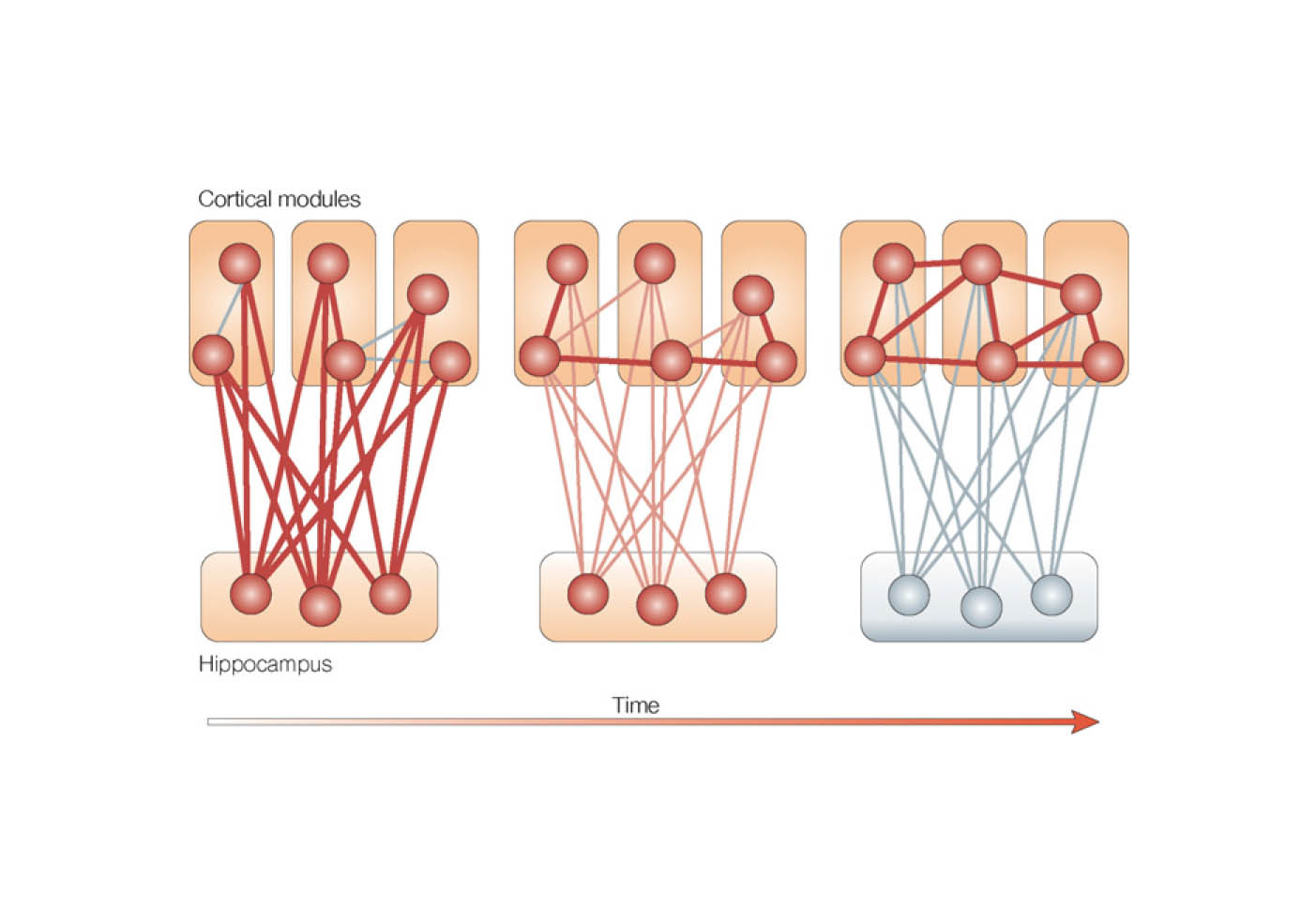
There’s a very good review from a major scientific journal, called “The role of the ventromedial prefrontal cortex in memory consolidation” by Ingrid L.C. Nieuwenhuisa and Atsuko Takashima published recently in 2011.
Autobiographical memories, such as sporting matches, are first formed in the hipppocampus, and they then get dispatched to a totally different part of the brain, the ventromedial/subgenual cortex as these memories become “consolidated”.
In other words, books can come from the events around the world bookcase, but while this is wobbling the autobiographical bookshelf is unscathed.
The crazy thing though is that the intact ventromedial prefrontal cortex is also connected with the intact amygdala in early Alzheimer’s disease, which means the autobiographical bookcase can arouse emotional memories in that bookshelf.
Sporting memories and “dementia friendly communities”
This is because they are shaped by the environment in unique ways, even if they have exactly genetic sequence as the blueprint which designed them.
It therefore cannot be any surprise that no two individuals in society are in the same, as you can easily witness with the range of opinions on your timeline on Twitter.
A person with a dementia might be very different to another person with a dementia.
There are a hundred different causes of dementia, tending to affect people in different age groups in distinct ways at different rates? Let’s pick one type of dementia, the most common cause, Alzheimer’s disease.
A 83 year-old with Alzheimer’s disease might have a number of different problems, for example memory – or even with problems in planning, aspects of language, or behaviour.
And of course it’s pretty likely that 83 year-old might be living with another different condition too, such as heart disease.
Your perception of that 83 year-old might vary from your next-door neighbour, according to, perhaps, your own personal experiences of dementia, good, bad or neither.
So, in raising awareness over the uniqueness of individuals through “Dementia Friends” or “Dementia Champions”, there’s an inherent contradiction.
How do we build ‘dementia friendly communities’, given one’s desire to embrace diversity?
I have for some time explained elsewhere why I think the term is a misnomer. I don’t see the point of “asthma friendly communities” or “chronic demyelinating polyneuropathy communities”, worthy though they are.
I think when you pick off any of the ‘protected characteristics’ in the Equality Act, such as ‘disability’, ‘sexual orientation’ or ‘age’, you have to be careful about not inadvertently homogenising groups of people, worthy though the cause of ensuring that they do not suffer any unfair detriment is.
It could be that people in the early stages of Alzheimer’s disease, due to how the condition tends to affect the brain, could have particularly problems with spatial memory or navigation. Therefore, it would be desirable perhaps to have places with clear landmarks such that such individuals can navigate themselves around.
But take this situation to an extreme. Would society feel comfortable with people with dementia having their own cafés?
After working all day, Parks boarded the Cleveland Avenue bus around 6 p.m., Thursday, December 1, 1955, in downtown Montgomery. She paid her fare and sat in an empty seat in the first row of back seats reserved for blacks in the “coloured” section.
The bus driver moved the “coloured” section sign behind Parks and demanded that four black people give up their seats in the middle section so that the white passengers could sit.
Rosa did not move.
A legitimate learning objective of ‘dementia awareness’ sessions is to think about what a person with dementia might or might not be able to do.
But if we then meet this learning objective, that people with dementia are all unique, we should steer away from stereotypes that people with dementia act ‘a certain way’.
This, I personally believe, is a big failing of this ‘dementia friendly communities awareness video’.
Whatever the rôle of the person providing care or support to a person living with dementia, excellent communication is essential. The time wasted scrabbling around for essential information about a person for any ‘service’ with which that person ultimately encounters, whether that’s housing, the NHS, social services, education, leisure, or even the police, should ideally be kept to a minimum.
One of the biggest problems with the ‘medical approach’ to dementia is that – unless you’re taking a professional psychiatric history – you can gloss over the finer details over the details of the events which contribute to how a person feels about his or her life. A person’s idea of self will almost certainly be affected by his or her past, ability to perceive the outside environment, an ability to assess the environment, and of course what that environment is (including the people within it). Unless relevant to the ‘diagnosis’ of one of the hundred or so types of dementia, it is perfectly possible for a medical doctor to gloss over such details, provided some targeted blood tests, brain scan, psychology or some cerebrospinal fluid confirm the diagnosis. And in fairness, the diagnosis is relevant to perhaps repeating the same investigations after a finite period of time, with medications of limited effect in the earliest stages.
It is perfectly possible for a medical Doctor to impart next to no information about what to expect might be effects of the condition; or what to expect in people’s reactions. That Doctor can provide next to no information about to how to engage with the benefits system.
Nor how to work with a local authority to get housing most suitable to his or her needs. Nor how the person can be somehow be given a chance to be educated about the condition. Nor about any activities, such as a local day club, which might be a happy, supportive social environment.
The term ‘whole person care‘ has enormous scope to be extremely fluffy: in thinking about the person as a ‘whole’. But when you think about how a person living well with dementia might be able to have a positive outlook with the right care and support the narrative changes.Sure, there are negative perceptions of what dementia can be like, but in the early stages the outlook does not have to be so bleak, full of words such as ‘devestating’, ‘horrific’ and ‘suffering’. But there’ll be a stage in a person’s life with dementia where he and she can be through a whole person approach be living in a way which promotes independence and wellbeing.
I envisage the health and wellbeing boards in the next parliament will be essential for this. Commissioning of services needs to be in the hands of people who know what they’re doing, and certainly it’s the current intention that existing structures will be requested to run the health service, including social care, in a Labour government. Local authorities I feel will be fundamental in ensuring right services are commissioned, including social care as part of the NHS, housing, education and leisure. But the country will need to ensure that knowledge sharing, with appropriate safeguards, is in the best interests of the person.
Take two alternative scenarios for a person with moderate dementia, who is a 76 year-old, in a privately run nursing home. He has only recently gone to that nursing home, having been independent for several years following his diagnosis in 2008.
This nursing home is ‘attached’ to a GP providing on-call medical cover. Recently, he has had recurrent episodes of urinary retention due to enlarged non-cancerous prostate gland. A member of the care staff notice him having very vivid nightmares, and very acutely confused on waking.
The question is what now?
Scenario 1.
The on-call GP is unable to catherise him, but diagnoses a full bladder. He is referred to his local A&E at 3 am. There are no medical notes transferred with him. The on-call A&E doctor does not catheterise him, but to beat the three hour target, admits him.
There are no ‘care of the elderly’ beds available, so he ends up on an adult general surgery ward. This surgical ward has been in the local newspapers for being the most “unfriendly dementia friendly ward ever”.
He is seen on the post-take ward round the following morning as an “outlier”, and then catherised with substantial urine drained. He is still noted to be confused.
That night, he, on a ward with persons without dementia, becomes anti-social, and agitated.
He then falls out of bed, and sustains a fractured neck of femur. He is referred to an orthogeriatric team in the hospital, who refuse to ‘accept’ the patient unless a full work-up for confusion is initiated. Various investigations are initiated, including a chest x-ray, urine culture and blood cultures.
On day 3, the orthogeriatric team agree to accept him urgently, and he is no longer confused. He has a hip replacement, and spends two days in hospital recovering.
On day 9, he is eventually discharged back to the nursing home, as the nursing home were not willing to accept him back.
Or take Scenario 2.
The information that he has recurrent episodes of urinary retention is made known through the electronic records system, and known to the on-call Medical Admissions doctor. The decision is taken for him to be catherised at the privately run nursing home, and their GP decides to start him on antibiotic treatment. His confusion resolves of its own accord within a matter of days.
There are clearly many scenarios (sic) like this one, but there are various points I’d like to make. These points are how disorienting a change of environment can be for an unwell person with moderate dementia, how the medical situation easily became hyperbolic, and how a hospital admission caused his medical problems to become much worse. But it’s a world apart from he could have been looked after the first place.
While ‘whole person care’ sounds quite fluffy for persons with dementia, it could be just what the Doctor ordered.
“The biggest disease today is not leprosy or tuberculosis, but rather the feeling of being unwanted, uncared for and deserted by everybody” Mother Theresa
I cannot recommend highly enough this account of loneliness in the context of primary care by Dr Jonathon Tomlinson in his powerful blog ‘A better NHS’.
In this, loneliness is a separable issue from whether a corporate can secure advantage by being ‘dementia friendly': it is an important social construct.
Earlier year in a prominent medical journal, it was reported that feeling lonely rather than being alone is associated with an increased risk of clinical dementia in later life and can be considered a major risk factor that, independently of vascular disease, depression and other confounding factors, deserves clinical attention.
The campaign against stigmatising stereotypes of people with dementia is a worldwide one.
And yet Norman Lamb frontloaded a standard shill for the Alzheimer’s Society ‘dementia friendly communities’ programme with an elaborate fictional description recently with an elaborate description of a bed-wetting confused person. Such negative propaganda severely runs the risk of further evaporating goodwill for the Alzheimer’s Society.
Lamb comments, “But dementia can be a cruel condition, both for those who have it and for the people who love and care for them.”
It is hard to know precisely what this ‘shock doctrine’ is supposed to achieve, other than to inject a feeling of fear and moral panic for readers of the Guardian. But the article is an extremely manipulative one. It identifies a really important social issue, but makes no room for discussion for anything other than a discussion of the Alzheimer’s Society and their ‘dementia friendly communities’ programme.
Lamb comments, “One million [dementia friends] are expected to be recruited by 2015.” But who’s doing the expecting? What are the penalties for not reaching this particular target?
There’s the bind. This exclusivity exists because one more ‘dementia friend’ somewhere is one fewer ‘Dementia Friend’ on the official scheme.
This can’t be called anything else but exclusivity.
So Norman Lamb has used a discussion about isolation in dementia to encourage exclusive behaviour. This makes us a laughing stock in our English dementia policy in the eyes of the rest of the world potentially.
Lamb refers to this scheme thus: “All of this should be just the start, the beginning of a massive social movement.”
But how organic is this ‘massive social movement’? The answer is not at all.
It is known that the £2.4 million programme is funded by the Social Fund and the Department of Health. And an eye-watering amount of money has been spent by Public Health England on this marketing campaign just gone as reported here, also to promote “Dementia Friends”.
Clearly not everyone is benefiting from local commissioning decisions to promote dementia. And these decisions have had a catastrophic effect on social interactions for some people with dementia, under the lifetime of this parliament.
For Norman Lamb to pop up and complain about loneliness in dementia having promoted this policy actively in England would it be like a Tory MP complaining his local law centre had suddenly shut down.
Earlier this year, a popular day care centre for people with dementia was reported as closing down. Staff at Mundy House day care, in Church Road, Basildon, were left devestated. Larchwood, the firm which runs the centre and adjoining residential home, claims the day care facility is not making any money.
Meanwhile, last year, a council was considering plans to close up to seven centres providing specialist care for older people suffering from dementia. East Sussex County Council’s cabinet were reported as set to discuss proposals which could see the closure of a number of centres providing day services for older people in Lewes, Bexhill, Hailsham, Crowborough and Hastings.
And, simultaneously at the other end of the country, a residential care home and day centre for elderly and vulnerable adults look certain to close in a shake-up. Plymouth City Council said Lakeside in Ernesettle and St George’s in Stonehouse were to be shut. The council said it was under financial pressures and numbers using the buildings were dwindling. It admitted that some staff would lose their jobs.
But ‘dementia friendly communities’, regulated by a strict standards protocol, or a badge of ‘Dementia Friends’, encourage exclusivity. Lamb in his article makes no attempt to widen the discussion to other possible means of inclusion.
“If you care for a relative with dementia life can seem very isolating. Carers sometimes live in a bubble, the roundabout of caring, sorting out finances, juggling family responsibilities and struggling with the challenge of keeping their relative safe, comfortable and happy. There may be issues such as family members not doing their part, or the carer may also have paid employment, young children or grandchildren to care for, or their own health issues. Many of the carers who contact me express their frustrations at feeling alone and unsupported.”
“Social media can be a great way to find other carers, and there’s a wonderful community on Twitter who support each other, share tips and good practice and lighten the day with comments, photos and light-hearted banter. If you are not already connected to the dementia challengers, I’d recommend you spend some time finding out how to use social media so that you can connect with this group of people. It’s easy to dip in and out of conversations when you have the time, or to use that five minute breather between other responsibilities to catch your breath and talk to someone in the same or a similar situation. Here are some tips about how you can use Twitter and Facebook to engage with other carers.”
And – providing supportive evidence for Lee’s argument – is a tweet by someone with familiarity with a rarer type of dementia, known as “posterior cortical atrophy”.
And, if loneliness is so valued by Norman Lamb and colleagues, shouldn’t funding be flooding in for initiatives such as the Healthy Living Club in Stockwell? The group meets for four hours each week for a programme of activities as a focus for the local community, to promote the mental and physical wellbeing of those people well with dementia. Each meeting is run as a social event, which people attend to meet each other, have a good time and share experiences. The Club is run with a team of volunteers and some sessional contributors, led by a paid co-ordinator. It is seen as a blue-print for future dementia care in the community.
“The Dementia Friends scheme is the country’s biggest ever project to change the way people think about dementia.”
In detail,
“By 2015, 1 million people will become Dementia Friends. The £2.4 million programme is funded by the Social Fund and the Department of Health. The scheme has been launched in England today and the Alzheimer’s Society is hoping to extend it to the rest of the UK soon.Each Dementia Friend will be awarded a forget-me-not badge, to show that they know about dementia. The same forget-me-not symbol will also be used to recognise organisations and communities that are dementia friendly. The Alzheimer’s Society will release more details in the spring about what communities and organisations will need to do to be able to display it.”
The campaign slots in very well to an infrastructure which acts as a safe ecosystem to promote “Dementia Friends”. The support of Government in this in allowing mechanisms of marketing, such as press releases, as well as resources, e.g.. for marketing campaigns, here is invaluable. A clear policy problem arises here as to whether it is the Alzheimer’s Society and “Dementia Friends”, or the concept which has a longstanding global policy footing.
The “cultural web”
To help understanding how corporate culture works, the “Cultural Web” came about.
The Cultural Web, developed by Gerry Johnson and Kevan Scholes in 1992, provides an approach for looking at and changing your organization’s culture. Using it, you can expose cultural assumptions and practices, and set to work aligning organizational elements with one another, and with your strategy.
The Cultural Web identifies six interrelated elements that help to make up what Johnson and Scholes call the “paradigm” – the pattern or model – of the work environment. By analysing the factors in each, it is claimed that you can begin to see the bigger picture of your culture: what is working, what isn’t working, and what needs to be changed.
But actually you can easily see how a corporate approach is supporting the methodology of ‘Dementia Friends’. Rather than it being an ‘organic movement’, it is a highly orchestated and organised example of a marketing campaign fitting of any large corporate.
The six elements are:
1. Stories
The past events and people talked about inside and outside the company. Who and what the company chooses to immortalise says a great deal about what it values, and perceives as great behaviour.
“Who decides what is great behaviour” is clearly a thorny issue.
It can be rather judgmental to consider what is a worthy community initiative, and what isn’t. Such an initiative can therefore potentially be incredibly divisive.
“In March 2012 the Prime Minister issued a national challenge on dementia – one of the key aspects of the challenge is creating dementia-friendly communities. Since then communities, individuals and organisations have all risen to the challenge and made Britain a better place for people with dementia. From local shops to large cities, buses to banks; we have heard so many inspirational stories of people and organisations making changes that help people living with dementia and carers in their communities. To celebrate all the hard work happening, we are holding the first Dementia Friendly Awards, sponsored by Lloyds Banking Group and supported by The Telegraph. The Awards recognise communities, organisations and individuals who have helped to make their area more dementia-friendly. This year the awards were open to entries from England only.”
“Awards ceremonies” form official recognition of the control systems too, as well as producing great marketing around an event.
It might seem rather dubious to ‘pick winners’, in that there will inevitably be ‘disappointed losers’ who do not ‘make the grade’, but the idea is to generate lots of positive publicity for the people involved and the sponsors, as well as for the Alzheimer’s Society obviously.
2. Rituals and Routines
The daily behaviour and actions of people that signal acceptable behaviour. This determines what is expected to happen in given situations, and what is valued by management.
3. Symbols
The visual representations of the company including logos, how plush the offices are, and the formal or informal dress codes.
The new “forget-me-not symbol” was launched on 8 November 2012, “embodying the UK’s social movement on dementia”.
There are certain restrictions on the use of this symbol regarding exclusivity (e.g. whether you’ve done on the course but gone onto wish to do your dementia awareness course without the use of the branding).
It is a monopoly trademark right, as demonstrated in its registration across an excessively high number of intellectual property classes on the UK trademark register.
However, “Dementia Friends”, many at the coalface feel, is a rather contrived movement with so much money being pumped behind it to force it to succeed.
When you enrol onto the “Dementia friends” website, there’s a mechanism by which you can receive your ‘Dementia Friends’ badge:
And the amount of free advertising that MPs can give for this is incredible.
“I pay tribute to my right hon. Friend for raising this issue. We have turned the zero on No. 10 into the dementia flower today to help to boost the importance of raising awareness of this issue and of encouraging more people to train as Dementia Friends.”
Such an initiative is great for the current administration which can paper over the cracks and terrible shortfalls in social care for dementia.
And marketing is a wonderful thing.
A lot of money, it seems, has been diverted from frontline care into making this project succeed.
The current Government were known to be pitching for professional marketing of ‘Dementia Friends’ last year. Agencies on the Government’s creative roster attended a briefing with the Health Secretary, Jeremy Hunt, on Wednesday (9 October). The campaign was aimed at promoting the concept of dementia friendship, and it would also encourage people to join Dementia Friends, an initiative run by Alzheimer’s Society to improve public understanding.
It is reported that Public Health England would invest up to £4 million a year until 2014/15 and expects significant additional funding from partnership marketing. “The scale of the challenge demands far greater ubiquity than we alone can fund,” a PHE spokeswoman said. The campaign was due to break in March 2014, with pitches will be held on 7 and 8 November and an agency will be selected by the end of that month.
The idea of celebrity endorsements, of course, is not new. Every day consumers are exposed to thousands of ads. and this will hamper companies to create a unique position and receive attention from consumers. Using celebrities can help companies to create unique ads and engender a positive effect on the attitude and sales intention towards the brand. Celebrity endorsement has been applied for many years. Already in 1979 one in every six commercials used a celebrity and in 2001 that percentage grew to 25%. The usage of celebrity endorsements has increased in the last decades and at the same time also the corresponding cash flows grew. In the year 1996 US companies paid more than 1 billion dollar to celebrity endorsers for endorsement deals and licensing rights.
In the latest video, celebrities star in a new advert to encourage people to become “dementia friends” to help boost volunteering, education and support for the growing number of people with the condition.They join up to sing a classic Beatles song to raise awareness of the isolation felt by those living with Alzheimer’s. The Dementia Friends campaign features Lily Allen, Chris Martin, Eamonn Holmes, Simon Pegg, Paul O’Grady, Sir Terry Pratchett, and many more all singing the track With A Little Help From My Friends.
The ways that the organization is controlled. These include financial systems, quality systems, and rewards (including the way they are measured and distributed within the organization.)
In January 2012, it was announced that a man in the early stages of Dementia wants his home town of Torbay in Devon to become “dementia friendly”.
Norman McNamara, a member of Torbay Dementia Action Alliance (TBAA), wants shops and businesses to recognise signs of the condition and to help local customers. In the meantime, he has gone onto build a massive genuine social movement, called the “Purple Angels”.
This is particularly odd given that here is Norman McNamara even pictured with the Prime Minister:
Norman had said he wanted the resort to back the campaign and eventually advertise it to potential holidaymakers.
Torbay District Council said it supported the idea and could see both the resort and visitors benefiting.
The question here is: what is a relevant standard of a ‘dementia friendly community’?
In the missive cited above, further details are provided:
“Development of a code of practice on dementia friendly communities
Building on the foundation stage of the recognition process, the Alzheimer’s Society has commissioned British Standards Institution (BSI) to develop a code of practice for dementia friendly communities. The ambition is to have 15 communities signed up to the BSI code of practice by March 2015.”
But here having a standard ‘code of practice’ means that commissioners can readily say that their community is ‘dementia friendly’, irrespective of what is actually happening on the ground.
It serves as a lazy tick box mechanism for local commissioners. And people become ‘locked into’ getting tenders from the Alzheimer’s Society. This is clearly unacceptable when there are many serious good innovative social enterprises, and other dementia charities, who are at a big risk of being disenfranchised.
It suits the signatories of that missive to tell Government they are doing a good job on dementia friendly communities.
It allows the current Secretary of State to report to the public (via compliant newspapers), that they are doing a great job on dementia friendly communities, despite any range of fiascos of poor dementia care on the ground such as Winterbourne.
6. Power Structures
The pockets of real power in the company. This may involve one or two key senior executives, a whole group of executives, or even a department. The key is that these people have the greatest amount of influence on decisions, operations, and strategic direction.
Conclusion
A range of techniques from the standard corporate marketing literature has been loyally harnessed to promote a corporate ‘cultural web’ around ‘dementia friendly communities’ from the Alzheimer’s Society. The Alzheimer’s Society, together with the current Government, have been able to secure competitive advantage, even harnessing appropriate use of legal monopolistic intellectual property rights. However, the drawbacks of such a well orchestrated approach is that it has not been able to mute genuine ‘word of mouth’ criticism which is mounting everyday over this policy on the social media. In light of the recent targets culture in the NHS, some experienced people have been publicly opining whether “Dementia Friends” is in fact hitting the target but in fact missing a point in genuine organic development of dementia friendly communities. It has become a vehicle being used primarily to promote this Government (Department of Health and Secretary of State), the Alzheimer’s Society, marketing companies, sponsoring corporates, and some celebrities, in as much as, or even much more, than persons with dementia or even the million-or-so army of unpaid caregivers.
In a popular group on “Facebook”, somebody has written the following:
“This will be my last message on this group as my husband has finally received the diagnosis that we have been waiting for. For years he has been diagnosed with dementia, firstly Lewy body Dementia and then for the last 2 years it has been FrontoTemporal Dementia but now we know the truth – he has Lyme Disease caught from a tick bite he didn’t know he had during our trip to The Rockies in 2003. For the last 10 years he has been seeing a procession of medical professionals including Neurologists, Psychologists and Psychiatrists but they have all said that he didn’t typically fulfil the criteria for any of the conditions that he has been diagnosed with but they have treated him as though he did, therefore he has had a boat-load of medication that his body didn’t need. If he had been tested for Lyme when he first started to baffle the medical profession then it could have saved us many years of traumatic symptoms, incorrect treatment and medical professionals openly saying that they felt his symptoms were ‘all in his head’, ‘nonsense’ and a ‘childish ploy for attention’. I THINK NOT ! Unfortunately we have had to go private to get the testing done but now we have a definitive diagnosis and a treatment plan. – it is typically successfully treated with an extended course of intravenous antibiotics and supplements to support the body through the treatment period. There is now a very bright light at the end of a very long, very dark tunnel.
I do appreciate that many of you will not agree to this message appearing on here but it is entirely possible that may be a few who have been in a similar position to my husband and I would urge you to consider the possibility of obtaining private testing (the tests are sent to Germany and USA as the tests done there are more sensitive and accurate than in UK) in the likelihood of having had a tick bite at some point. I have attached a short video that explains the problems with getting Lyme diagnosed and once again apologise if this message seems inappropriate.
The current Government, in partnership with the Alzheimer’s Society, is trying to improve the diagnosis rates of dementia.
The medical profession has been consistently warning, on deaf ears, that every misdiagnosis of dementia is potentially a tragedy.
For every incorrect diagnosis of dementia, a person is being denied treatment for the correct diagnosis.
For every incorrect diagnosis of Alzheimer’s Disease, a person is being denied treatment for a different, but correct, cause of a cognitive problem.
It is dangerous that this policy exists in England, which promotes ‘dementia awareness’, but which has not improved resources for specialist clinical services for the diagnosis, investigation and management of dementias.
Dementia is part of a wide ‘differential diagnosis’, meaning that many conditions can mimic dementia particularly in the elderly.
The infective agent of Lyme disease is the spirochaete Borrelia burgdorferi, usually transmitted in tickbites.
The disease occurs sporadically in parts of North America, Europe and Asia, but true prevalence is unknown. Infection can lead to a whole manner of presentations in any part of the nervous system.
Clinical symptoms include an acute rash (erythema chronicum migrans) at the site of the bite within a month, which is indicative. Relapsing, migratory, large-joint arthropathy and carditis may occur.
Overall, 10–15% of affected individuals develop neurological symptoms. Cognitive impairment, inattention and emotional lability may be present, with usually mild chronic confusional state.
Subjective memory loss has been suggested but a clear dementia syndrome is very rare is very rare.
Specialist testing would have been necessary to identify this in the NHS.
For an investment equivalent to the cost of ‘Dementia Friends’, £2.4 million, it’s quite likely that a disaster like this would have been avoided in this jurisdiction.
The timebomb which is ticking is not the numbers of dementia.
Do pardon the bad pun.
In this jurisdiction, evidence now points to a falling prevalence of dementia cases.
The real “timebomb” for dementia is the number of unsafe diagnoses from non-specialists.
There are fewer than 365 days until the next general election on some happier news.
Dementia was mentioned twice today in Prime Minister’s Questions.
There was a ‘big announcement’ today from the Alzheimer’s Society which could have been used to convey the meaning of how people living with dementia could be encouraged to live well in productive lives.
As part of this publicity, Terry Pratchett was pictured holding up a placade saying, “It’s possible to live well with dementia and write bestsellers “like what I do””.
“Up to £1.6 billion a year is lost to English business every year, as employees take time off or leave work altogether to provide at-home care for elderly relatives, according to the report, compiled by the Centre for Economics and Business Research (CEBR).”
“On top of those that stop working, another 66,000 are making adjustments to their work arrangements, such as committing to fewer hours or working from home.”
Paul Burstow MP brought up the first question specifically around this initiative.
Here is the Question/Answer exchange as described in Hansard:
The answer fails spectacularly to address the issue of living well with dementia, but is a brilliant marketing shill for ‘Dementia Friends’.
There’s no attempt to include any other charity working in dementia.
It doesn’t mention the C word either – Carers.
And then it was left up to Hazel Blears MP to provide another question on dementia.
This time it’s a bit different.
There’s no answer on how zero hours contracts cannot specifically in the care system promote living well for either carers (including unpaid careworkers) or persons with dementia.
But it’s exactly the same otherwise.
A brilliant marketing shill for Dementia Friends, and no mention of any other charity working on dementia.
Quite incredibly here, Cameron produces an answer on ‘caring’ in dementia without mentioning carers or careworkers.
With Ed Miliband, Ed Miliband and David Cameron all wearing their ‘Dementia Friends’ badges, is it any wonder you never hear about Dementia UK’s Admiral Nurses any more?
There is undoubtedly a rôle for all players in a plural vibrant community, but this should never have been allowed to become an ‘either’/’or’ situation.
Innovations can not just be about products. They can be about fundamentally a whole new way of doing things.
The traditional large charity for dementia model has its advantages. It, through economies of scale and large operational efficiencies, can implement large projects, liaise with governments, and have a lot of media backing in the implementation of their projects.
The down-side to this is that it can too easily suffocate innovation from small social enterprises. It can also pursue agendas which are biased in one particular direction.
One example is witnessed in the the appointment of the World Dementia Council.
As it is, large charities, in promising to deliver new orphan drugs for dementia one day, can totally ignore the need for high quality research into living well with dementia. They can treat their associated persons with dementia as ‘subjects’ for future drug trials.
This is incredibly problematic and obstructive for those people with dementia – and their supporters including researchers – who wish to pursue an agenda of quality of life in dementia for current people living with dementia.
Even in the press bulletin for the first meeting of the World Dementia Council, dementia is referred to as a ‘timebomb’.
Currently, the evidence for the feasibility of this approach is very poor, however.
But something quite amazing, and indeed “disruptive”, happened quite recently. To say it could be explosive for international policy is in fact an understatement.
The ADI welcomed Glenn Rees, current CEO of Alzheimer’s Australia, as its Chair-Elect. This is a highly significant appointment, and one which people who promote the living well with dementia philosophy extremely warmly welcome.
So what?
A plucky group of people with dementia emerged, gave talks, and presented cutting-edge research. It was no longer a case of ‘listening to people with dementia’, but rooms packed full of people mesmerised by original contributions from a totally different perspective.
One academic in stigma was overheard to say to a person with dementia: “You don’t look like a person with dementia.”
That person commented that the academic didn’t, either.
Dementia Alliance International is a non-profit group of people with dementia from the USA, Canada, Australia and other countries that seek to represent, support, and educate others living with the disease, and an organisaton that will provide a unified voice of strength, advocacy and support in the fight for individual autonomy and improved quality of life.
Membership in Dementia Alliance International is free and open to people with dementia only, in any country.
Membership is open to any person with dementia who would like to be part of a global community of others with dementia where members support and encourage each other to live well with dementia, or oin others in fighting against the stigma, isolation and discrimination of dementia.
In addition to the larger countries, there has been interest from Taipei, New Zealand, St Maartens, Spain, Puerto Rico, and Japan, to name but a few. Of course, such an initiative is immediately attractive to a lot of other people who have the cash, including world philanthropists who have some personal connection with dementia.
This group has even been ‘noticed’ by the larger corporates and corporate-like entities in dementia, but people close to this group report that they are desperate to keep their autonomy and identity, despite possible (legal) enticements.
They know that they are on the threshold of massively disrupting current policy. They know they won’t be one or two bums occupying seats on research panels of large charities any more, only.
They will be there now leading the pack.
1. ADI staff get recognition for their work.
2. Final panel on Sunday includes person with dementia from USA, Scott Russell.
3. Final Panel with Scott Russell.
4. Person with dementia from Puerto Rico, Julio, speaks out as keynote. He got the only standing ovation of the morning’s speakers.
5. The DAI team
6. Kate Swaffer, from DAI, before her presentation of her model, “Prescribed disengagement”
Personal budgets held by individual people might allow more flexibility in choice and control over health services. So what’s the harm in them?
Barry Schwartz’s famous book “The paradox of choice”, summarising a lot of other evidence, contests the assumption that maximising collective welfare of citizens is achieved through maximising individual freedom.
On May 8th 2015, there’ll be a change in government in the UK (unless the arithmetic happens to throw up another Conservative-Liberal Democrat coalition, which is quite unlikely). It is likely that all the major political parties will wish to implement a form of ‘integrated’ or ‘whole person care’, with the merging of health and social care. It is a moot point how early on people, if at all, will be offered the chance of a ‘unified personal budget’.
No matter how much effort you put into ‘compassion’ or ‘Dementia Friends’, the care system is never going to be acceptable in the light of dangerous financial cuts to social care.
The “one size fits all” philosophy seems to be pervasive in the Government approach to personal health budgets, whichever Government pursues it. It’s as if it doesn’t matter who is the singer is because the song is the same: like Pharrell’s “Happy” was originally recorded by Cee Lo Green (allegedly).
Certain people with early dementia might be particularly prone to impulsive or risk-taking behaviour, so there is a reasonable question whether some persons with dementia – despite full legal capacity – are “safe” to have personal health budgets themselves. But this I feel strengthens my argument for a proper system of delivery of personal health budgets, not undermining them. When personal budgets work for dementia, as explained by Colin Royle here, they work very well.
A potential danger is that somebody is given a list of ‘options’ for care support planning, and effectively told to get on with it. It can be difficult to get to the precise details of resource allocation systems, and, without knowing such details, it is difficult to ascertain whether they legally constitute a process acting to the detriment of the group of people with dementia. This leaves individual local authorities open to an accusation of indirect discrimination, offending the Equality Act (2010). There are various sources of factors which might cumulatively cause certain people to be more disadvantaged than others: e.g. an ability to ‘self-assess’ one’s needs in a questionnaire (with age being a confounding factor).
Personal budgets might be offered in a number of ways: namely those which were directly commissioned and managed by the local authority, third party managed accounts, direct payments or a mixture of these things. Concerns might come from all sorts of quarters: such as actual budget holders who don’t feel that the resources allocated meet their needs, or the professions who don’t feel that certain candidates are suitable in the first place.
This is perhaps one of those uncommon instances where ‘cutting out the middle man’ is in fact a dangerous idea. The actual calculation of resource allocation for an individual candidate is emphasised rather than the calculation of running the whole system adequately, in much the same way that the improvement in wellbeing in a personal budget might accrue from having a choice at all rather than the actual proposed care intervention.
“Quality support planning needs the investment of time. In the ideal world, presented by those who ‘run with’ the agenda, everyone is able to take an active part in making decisions for themselves and choosing their own care to meet their needs, as defined by themselves. The reality is that some groups have not been able to engage in the process of taking an active role in their own support planning; they are effectively excluded. This may be because they lack the capacity to manage a direct payment or organise a personal budget themselves, or because they lack support systems around them, such as family to help them do this.”
Clearly not everyone has benefited from the “Prime Minister’s Dementia Challenge”. For example, the Dementia Advocacy Network went bust at the end of last year. And yet this is precisely the time when people with dementia, and caregivers, need emotional support, and need to be safeguarded against forms of abuse including financial and legal. It appears that people who have benefited most from personalisation are those with the best advocacy and loudest voices.
Even with the most-straightforward appearance of self-assessment application procedures for personal budgets might require an enormous amount of professional support. There are various reasons why persons with dementia might have special obstacles in their uptake of personal budgets, as articulated well by the Mental Health Foundation: two for example include a residual stigma and discrimination against such citizens, and also the fact that some citizens might not have a reliable correct diagnosis in the first place.
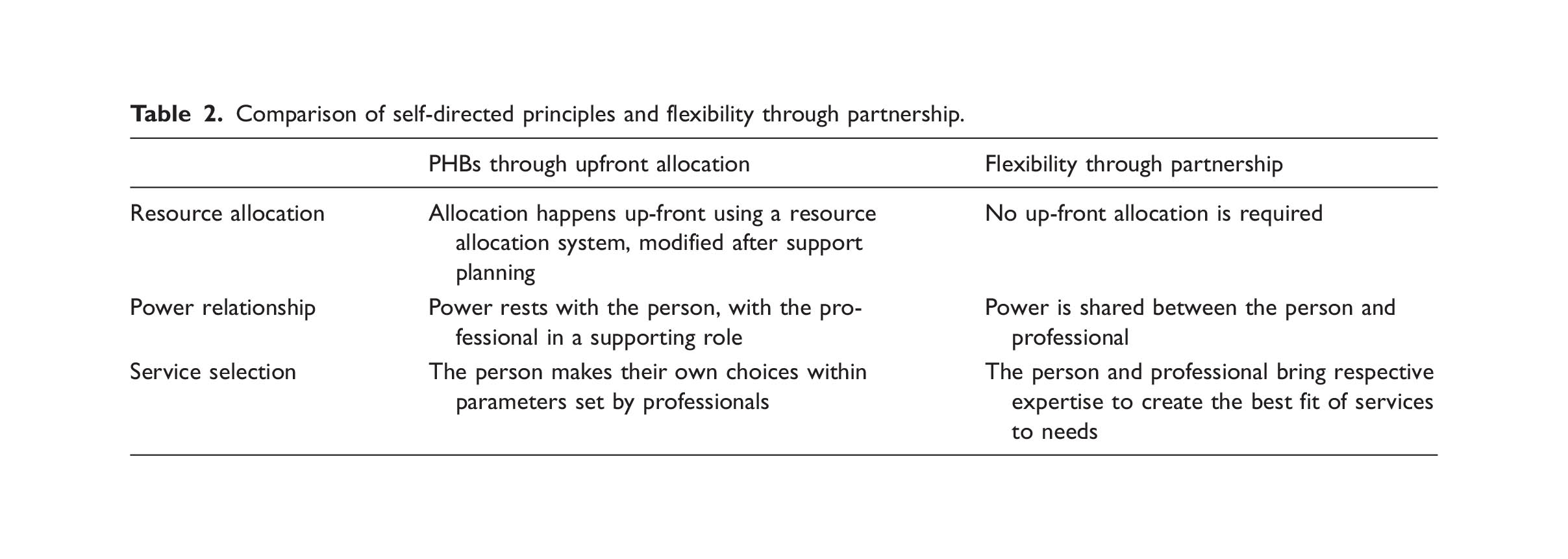
Self-directed support (SDS) has as its central feature a personal budget arrived at through an ‘up-front’ allocation of money; though up front allocation to give people power is one element of SDS amongst others and therefore it would be unfair to generalise across all the resource allocation systems techniques. It was introduced as formal policy in 2008, with an original target that all service users should have a personal budget for social care by 2011. In a recent helpful article, “Personalization of health care in England: have the wrong lessons been drawn from the personal health budget pilots?“, various well-known methodological problems with the original pilots are considered. The authors do, however, propose an extremely constructive way of moving forward, what they call “flexibility through partnership”.
Cheekily, the authors observe:
“As Gadsby points out ‘It seems that in many cases, additional resources[in the PHB group] were provided that enabled individuals to pay for extra services or one-off goods. It is perhaps unsurprising, therefore, that overall improvements were found in wellbeing amongst budget holders’”.
Without advocacy services, then, we really do run the danger of running a two tier service, and this is extremely dangerous, aside from the swathe of legal aid cuts. For a government which prides itself on parity, particularly for empowering new private providers to enter a liberalised market, any proposed system of personal budgets will require the same quality and opportunity for flexibility to all user groups including those who have no recourse to advocacy. A strengthened social care system would go a long way here.
Nobody has a single right answer for personal budgets in dementia so it might not be able to have the exclusive kite mark to match. It’s clear whilst there might be excellent ways of implementing them, there are plenty of bad ways too.
Unfortunately, time is running out a bit, and political leadership and adequate funding – including for advocacy services – are now both essential.
And who will benefit? If they work well, they will shift power to the people able to make ‘correct decisions’ in care, but I feel that the whole system has to be fit-for-purpose not the budget mechanism itself. That’s where the State comes in. Who the correct advocates are, as they might not necessarily be carers including unpaid caregivers (though they might be.) Ultimately, the most offensive irony would be to make the tool that offers choice and control compulsory, but this could be expected from politicians who like to give an illusion of choice.
There are still deeply engrained issues about whether people will have enough money to meet their needs. It might be easier to hide downsizing of budgets if they’re called a yet further new name. There are obviously huge problems with merging one universal system intended to be comprehensive and free at the point of need with one which is not and means-tested; and this would not necessarily benefit the person with dementia. And at worst, the wrong type of broker, not professional advocates including social workers, could be profiting but not providing overall benefit. Introducing any transactions into a system absorbs resources, however you attempt it.
We now have to be very careful with resolution of this potentially useful policy plank – otherwise it might be a case of ‘You’ll do’, rather than ‘I do’.