This morning I had a present for Andy Burnham MP (@andyburnhammp), about to lead the Labour troops into battle for the European elections. The present is of course a copy of my book ‘Living well with dementia’, which is an account of the importance of personhood and the environment for a person living with dementia.
“So, if one had unlimited funds, what sort of service could be designed to provide care and support for people with dementia? In my opinion, the answer is a very different one. Ideally, all services, which could include healthcare, housing and legal systems, would adapt quickly and flexibly according to the needs of the individual living with dementia. This would need to be managed by a named, long-term co-ordinator of care and support.”
“The idea of a care navigator able to call on and coordinate all available health and social care, as well as housing support and voluntary sector provision is a persuasive one. It is something that the Richmond Group of charities, among others, have for a long time called for – and it is something I would like to see the Liberal Democrats deliver in the next government. Better managed and coordinated care would be a huge step forward and could make all the difference to dementia sufferers and their often strained carers.”
In this framework, a “care co-ordinator” acts as a single point of contact and works with the patient, their carer(s) and the multidisciplinary team to develop a care plan.
Once this has been agreed, the co-ordinators work with the team, the patient, the patient’s family and other care providers to deliver co-ordinated and coherent care. Personal continuity of care is actively encouraged, and the care teams work hard to ensure an immediate response to care needs as they arise.
The care co-ordinator becomes he patient’s advocate in navigating across multiple services and settings providing care directly in the home environment.
He or she also communicates with the wider network of providers (outside of the core multidisciplinary team) so that information about the patient/carer is shared and any actions required are followed up.
The King’s Fund has previously found that the type of person undertaking the care co-ordination function varied greatly.
Most care co-ordinators had been community or specialist nurses, yet the role has also been taken on by non-clinical ‘link workers’ (in Sandwell) and health and social care co-ordinators (in Torbay).
There also appears to be a continuum from the non-clinical approach – primarily providing personal continuity to service users and acting as their advocate to ensure that care is co-ordinated around their needs – to the clinical approach, in which a case manager would also be able to provide clinical care directly.
It’s very much a n0n-authoritarian, non-hierarchical approach where each person, including the person living with dementia, has an important part to play.
Influences on someone living well with dementia might include design of a home or ward, assistive technologies, ambient-assisted living, “dementia friendly communities”, for example.
With the introduction of ‘whole person care’, it’s possible that the care co-ordinator for a person living well with dementia might become a reality.
In this construct, Andy Burnham MP, Shadow Secretary of State for Health, is trying to stop the overhospitalisation (and overmedicalisation) of people.
In everyday English, a “last chance saloon” means a situation beyond all rational hope.
After decades of working on drugs for Alzheimer’s disease (AD), the best the industry can manage is some drugs which have some effect on symptoms for a few months, but for which there’s no evidence they delay the progression in the long term.
Big Pharma have maintained this deception uptil the very last minute, indeed uptil the patents ran out.
They know they’re now drinking at “the last chance saloon”.
David Cameron backed Maria Miller, and that failed.
He backed the Big Society, and that failed.
Now he has backed research into dementia-busting medications.
After a 16-month inquiry, a verdict was reached on Maria Miller.
Commissioner Hudson found that Miller should have designated the Wimbledon property as her main residence, that she should have reduced her claims by two-sevenths to take account of her parents’ presence and that she overclaimed for interest on the mortgage by around £45,000.
Nonetheless, there was no indication Miller had done anything unlawful or illegal in her deception.
On the other hand, the Japanese drugs company Takeda was fined a record £3.6bn ($6bn) by a federal court in the United States on 8 April 2014 following claims that it concealed a possible link between the drug pioglitazone and bladder cancer.
The fine is the largest to be imposed on any pharmaceutical company.
Takeda’s US partner Eli Lilly, who marketed and sold pioglitazone in the United States between 1999 and 2006, also received a £1.79bn ($3bn) fine.
The diabetes drug pioglitazone, marketed as Actos in the US, received marketing authorisation in Europe in 2000. Actos is marketed and sold in the United Kingdom by Takeda UK Ltd.
Today we found out that Tamiflu doesn’t work so well after all. Roche, the drug company behind it, withheld vital information on its clinical trials for half a decade, but the Cochrane Collaboration, a global not-for-profit organisation of 14,000 academics, finally obtained all the information.
Putting the evidence together, it has found that Tamiflu has little or no impact on complications of flu infection, such as pneumonia.
The huge scandal, of course, is that scandal Roche broke no law by withholding vital information on how well its drug works.
Elsewhere, standardised tobacco packaging is intended to reduce the appeal of tobacco products by removing advertising and increasing the prominence of health warnings.
This measure has strong support from health professionals, particularly as rates of child uptake of smoking are still unacceptably high.
Tobacco industry misrepresentation of the evidence in order to try to block public health interventions by manipulating policy making and public opinion is now well documented.
On March 2011, the National Health Service’s National Institute for Health and Care Excellence (NICE) concluded that donepezil hydrochloride (trade name Aricept, Pfizer) could be ‘recommended as (an option) for managing mild as well as moderate AD’.
The conclusion was drawn despite reportedly poor cost efficacy3 and opinions that the use of the drug is a ‘desperate measure’.
The NICE decision was based on two meta-analyses (the second was an update of the first) of randomised controlled trials (RCTs) that demonstrated donepezil’s effect on measures of cognition, behaviour, function and global skills.
Of the 19 studies included, 12 were produced by the companies that manufacture and market donepezil. And a recent study has found that the effect size of donepezil on cognition is larger in industry-funded than independent trials and this is not explained by the longer duration of industry-funded trials.
The history of anti-dementia drugs is inglorious. This is significant because every pound spent in flogging this dead horse is a pound denied from current persons living well with dementia.
Tacrine is an oral acetylcholinesterase inhibitor previously used for therapy of Alzheimer disease. Tacrine therapy has been linked to several instances of clinically apparent, acute liver injury.
Because of continuing concerns over safety and availability of other acetylcholinesterase inhibitors, tacrine was withdrawn from use in 2013.
And it is widely reported that current candidate drugs for Alzheimer’s disease are running into problems because of their side effect profile.
Maria Miller may have finally left the ‘last chance saloon’.
But it can’t have escaped Big Pharma, despite ‘the G8 dementia summit’, possibly the largest PR stunt for pharma and research funded by pharma in history, that they are currently drinking there.
The deceptions might be so far be legal.
Maria Miller’s claims might have been hyperbolic; at least she didn’t have a highly staged G8 summit afterwards.
But, as with Maria Miller, the court of public opinion may provide otherwise.
Some ‘symbols’, such as the ‘Purple Angels’, clearly offer much reassurance.
I am genuinely interested in what ‘dementia awareness’ is.
Raising awareness can mean different things to different people.
It’s easy for me to overestimate what dementia awareness might be, as I have done my undergraduate finals, my Ph.D and my postdoc in brain conditions, and mainly dementia.
I’ve never seen a Dementia Friends script.
I’m mildly worried about whether the information in this script is accurate, but not any more than any other information from any other awareness publications.
Having worked in two head offices of large medical charities, I am more than aware of the crap that is used for fundraising.
But I do worry in case what you’re promoting is simply a source of income, and dwarfs entirely what the message is.
The message here is raising awareness of all things dementia.
We have to be very careful that befriending initiatives do not inadvertently end up belittling the whole issue of dementia.
I don’t particularly mind if people wish to purchase ‘Friends for Dementia’ air fresheners (spoof).
I don’t particularly mind if people wish to purchase ‘Friends for Dementia’ furry care dice (sic) (spoof), either.
Some thought inevitably has to go into ‘raising awareness of what’?
Chris Roberts, a supporter of the ‘Dementia Friends’ programme, suggested,
“To educate people, so they can spot symptoms early, help others in the community and help carers cope better, to show people in early stages are not to be written off, it’s all about education.”
This is of course a laudable aim.
But spotting symptoms of dementia in yourself may not be as easy as spotting a breast lump or a testicular lump (which admittedly can be difficult to spot).
Some people living with dementia are unaware of their symptoms, a phenomenon known to clinicians as ‘anosognosia’.
Raising awareness of the practical difficulties that Admiral Nurses have had in being commissioned?
And the stories keep on coming of potential or actual actioned cuts of dementia services in the real world: such as this one in Devon, and one in Essex.
I asked Kim Pennock, a prominent dementia campaigner in England, whether campaigners for dementia were concerned about cuts in social care.
“- many are now shouting loudly as the cuts are ridiculous and will put vulnerable people at risk”
Meanwhile, the Alzheimer’s Society have introduced a scheme for accreditating ‘dementia friendliness’.
The process is designed to enable communities to be publicly recognised for working towards becoming dementia-friendly and to show that they are following common criteria that are based on “what we know is important to people affected by dementia and will truly change their experience.”
It would be odd if the Alzheimer’s Society would be the sole arbiter of dementia friendliness.
Innovations in Dementia has in the past been working through the Ageing Well programme with two areas, Hampshire and Sheffield, to support their work to create dementia friendly communities.
As part of the work in Hampshire, they have produced a dementia friendly communities toolkit, which was designed to support work at a local level.
The tools have even been used by the Alzheimer’s Society locally.
But the Alzheimer’s Society has a massive business advantage nationally.
The Alzheimer’s Society has just appointed Lida to creating a series of campaigns that aim to increase the acquisition of new supporters and grow its mass participation events.
But accreditation can be good for ‘competitive advantage’.
The UK division of Hilton Worldwide has become the first hotel company to be awarded the Carbon Trust Standard after measuring and reducing its carbon footprint.
The award requires organisations to measure, manage and reduce their carbon footprint and make reductions vear-on-year.
Hilton believes the accreditation will give it a competitive advantage over rivals when the government’s Carbon Reduction Commitment league table begins next year.
There’s no doubt in my mind that dementia ‘friendliness’, however delivered, is a wonderful societal aim.
But it should not be a cover for cuts in social care or in the NHS.
And also it’s widely established that ‘Dementia Friends’ cannot be used in place of training for those who need more than basics.
I, too, will be doing my bit too though for raising awareness too.
I’ll be doing a ‘Meet the author’ slot at the London Alzheimer’s Show.
I think also it’ll be possible to see my book, a book which is very ‘un-medical’ in its approach. It’s all about celebrating the individuality of a person, what he or she can do, and how the environment is so important for quality of life.
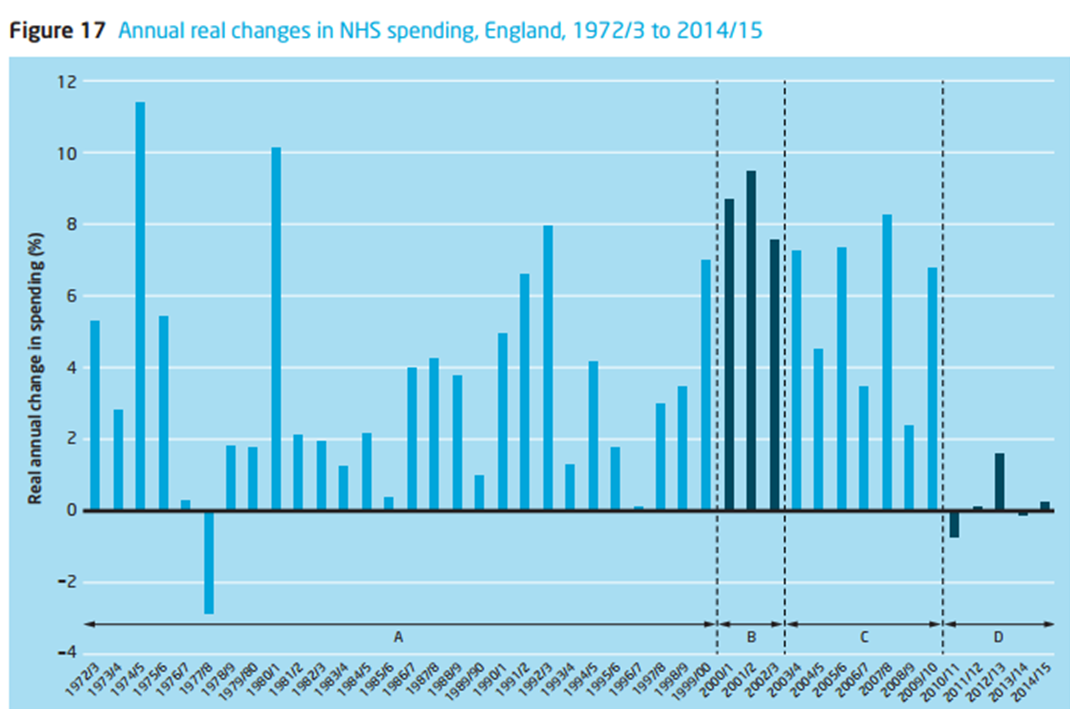
With commissioners having to make crucial decisions about acute and chronic healthcare, and, with an ever increasing budget being engulfed for some by paying PFI loan debt repayments, it has never become more important to have properly funded resources for medicine, nursing and social care. Gimmicks, such as badges and pledges, or talks given by people with worse than a very basic knowledge of dementia, can have their place, but they are never a replacement for care and support from the State which needs adequate financial funding.
With graphs such as this displaying real time spending in the NHS as a whole, cutting back on care might seem like an easy option, especially with a supine media promoting ‘awareness’.
Awareness cannot be ascertained by how many stickers you have in a shop window, or how many corporates you have to got to sell your gimmick with your logo. It’s about a dialogue about the dementias are about, what medications can and cannot do, and possible strategies for supporting living well with dementia or what makes a care home, amongst lots of other issues.
There is an alternative to trivialising dementia. I am now actively avoiding twitter conversations which trivialise dementia to a gimmicky or an equally superficial level where you flit about talking crap to another.
From the point of an initial diagnosis, to navigating your way through an increasingly complex health and social care and benefits system, and to experiencing the raw emotion of it all, the experience might be called a ‘journey’. This term clearly has its limitations, as there aren’t any suitcases packed, and there’s no return ticket.
There are questions to be asked, invariably.
What form of dementia is it? There’s probably about a hundred different types of dementia, though Alzheimer’s disease is the most common form,
Is there medication which might slow down the symptoms? Recent years, with different agendas to blame, have witnessed obfuscation and subterfuge of this basic issue. See my recent blogpost here, for example.
Either way, what is the prognosis? How will the illness develop? What alternative support mechanisms are there? Can the person with dementia, at various stages, be supported to stay at home?
Or would a residential home offer a better quality of life? What determines a good residential care home? Could a member of the family accept the person into their own home? What is the role of the social services – will three 10 minute visits every day go anywhere near alleviating the family’s worry?
These questions are invariably important.
Yet, if the GP or the Consultant who diagnoses the condition, pointed the family in the direction of Dementia UK’s Admiral Nurses, so many of the family’s questions would be answered immediately and the “journey” now being undertaken would not be so lonely. It has struck me how keen people are for ‘befriending’ schemes run by people who literally have no idea what dementia is, while criticising vehemently the ‘care model’ of Admiral nurses. This is simply not on for me.
The problem is that there are far too few Admiral Nurses, and the name is not widely known – although, of course, it should be known by the medical profession. Until recently, Admiral nurses, only formed part of community nursing teams. But now the principles are being used in hospitals too.
Even if there is no Admiral Nurse in your geographical location, the medics could at least suggest Admiral Nursing Direct’s telephone help line. This is staffed by experienced Admiral Nurses and offers practical advice and emotional support to people affected by dementia. Admiral Nurses are supported by Dementia UK. The charity works with NHS Trusts and other not-for-profit organisations- such as Making Space, Age UK and the Royal British Legion – to set up the services.
It costs £80,000 per year for an Admiral Nurse – £50,000 for the salary (the NHS standard wage for someone who is as highly skilled as Admiral Nurses need to be) and £30,000 for the Admiral Nursing Academy costs, Pioneer work and other overheads. Dementia UK provides the £30,000 needed to train a Registered Mental health Nurse to become an expert in Dementia care and the salary is paid by the NHS or other not-for-profit organisations.
At the moment, there are only 85 Admiral Nurses in the UK and, clearly, with cases of dementia now topping 800,000 in England, many more of these qualified Nurses are – and will be – needed. Very many people have asked, “Would it not be better to invest the £2.4 million – set aside for the Dementia Friends Initiative – in the recruiting, training and expanding the network of Admiral Nurses?”
One thing that the general public are not is stupid.
All nurses can make a contribution across the dementia pathway, defined as the right care, support and treatment for a person with dementia in the right place and right time. This should be rrespective of provider, whether it’s within the NHS, social, private, voluntary or prison sectors.
This support starts right from living well with dementia, empowering persons with real information about what to expect from the condition, and reducing social stigma, through to early identification, diagnosis, and maintaining health and wellbeing. This will need ultimately to come to a helpful and constructive candid discussion about end of life care and bereavement support for carers and their families.
All nurses – public health nurses, midwives, mental health nurses, learning disability nurses, district nurses, community nurses/matrons, practice nurses, Admiral Nurses, specialist nurses including specialist dementia nurses, acute nurses, Macmillan nurses and palliative care nurses – all have their part to play in achieving, and sustaining, better outcomes for people with dementia, at all ages.
To find out if there is an Admiral Nurse in your area, please ring 0845 257 9406 (phones are answered Tuesdays-Thursdays 11am-8.45pm and Saturdays 10 am-1pm) or email direct@dementiauk.org
If you are a carer for someone with dementia, you might think about joining Dementia UK’s “Uniting Carers”, which is an involvement network of family carers of people with dementia. The aim of the network is to give carers the opportunity to raise awareness and increase people’s understanding of dementia – and find support from others in the same situation. Click on the link on Dementia UK’s website.
Finally, it’s struck many of us that many hospitals are ill-equipped for patients with dementia when they are admitted with a medical problem. People with dementia don’t go into hospital because they have dementia, they are there because they are physically unwell but, unfortunately, acute hospital staff have been ill-equipped to deal with the added needs that dementia presents, both for the person with dementia and their carers.
With the introduction of ‘efficiency savings’, some acute medical departments took on the atmosphere of a conveyor belt.
This is alarming also for the junior staff who have to work in such conditions, whilst simultaneously expected to deliver ‘compassion’. Of course, for many who have never done a clinical rôle in their life, such as worked in entertainment or politics, it can be low hanging fruit.
Under such conditions, it can seem that meeting the physical and psychological needs of patient gets given a low priority.
And simple things can make a massive difference.
For example, if patients are confined to bays, they might be tempted wander off and be at risk to themselves or others.
On the other hand, if you give them a table and encourage patients to join each other for a biscuit and a chat, they will relax and have a much more positive experience of being in hospital.
Some nursing leaders clearly are passionate about reforming hospital care for patients with dementia and their families.
Take for example development of the pioneering dementia-friendly ward for patients with memory problems who are admitted with a medical condition, which includes brightly coloured doors to help patients remember which bays they are staying in and a lowered nurses’ station renamed “reception” to improve accessibility and ensure patients feel more comfortable.
So let’s give the gimmicks a bit of a rest, and invest in proper care and support for once?
.@legalaware Wow-thanks for such a detailed statement of support for Admiral Nurses! You’ve really captured their uniqueness&our challenges
We were joined by top marketing consultants this morning to advise on our crowdsourcing campaign.
The draft details of my crowdsourcing campaign, to raise awareness of decisions, the importance of decisions in dementia, and how decisions can possibly be influenced, are here on my Kickstarter page.
This campaign is not live yet.
Most marketing strategists will agree that creating customer value is fundamental to both profit-seeking companies and nonprofit organizations.
Indeed, creating superior customer value is a necessary condition for a company securing a niche in a competitive environment, not to mention a leadership position in the market.
A price signal is information conveyed, to consumers and producers, via the price charged for a product or service, thus providing a signal to increase supply and/or decrease demand for the priced item.
A large focus of our discussions was ‘market segmentation’.
Market segmentation is a marketing strategy that involves dividing a broad target market into subsets of “targets” who have common needs and priorities, and then designing and implementing strategies to target them.
Market segmentation strategies may be used to identify the target “backers”, and provide supporting data for positioning to achieve a marketing plan objective.
As a result, I might develop product differentiation strategy, so that the website I am designing fulfils diverse needs, such as for people with early dementia, journalists or NHS commissioners.
One of the leading consultants advised that for my particular project, and this is a difficulty any product-oriented kickstarting campaign, that “content is King”.
He advised me that a big problem with my pitch is that the figures asked for seemed very ‘budget’. I think, in fairness, he was concerned about my project looking too “bargain basement”.
Too cheap or too expensive can both be off-putting.
We’ve been advised to maximise use of all marketing channels, and to synchronise properly rewards to the different market segments.
This all seems very sensible.
But it’s all the same very exciting.
I hope to get hold of the makers of this short animation, based in Serbia, I think so that they can make a short animation on the importance of decisions for people living with dementia (for a stated revised budgetary cost of my output of crowdfunding campaign.)
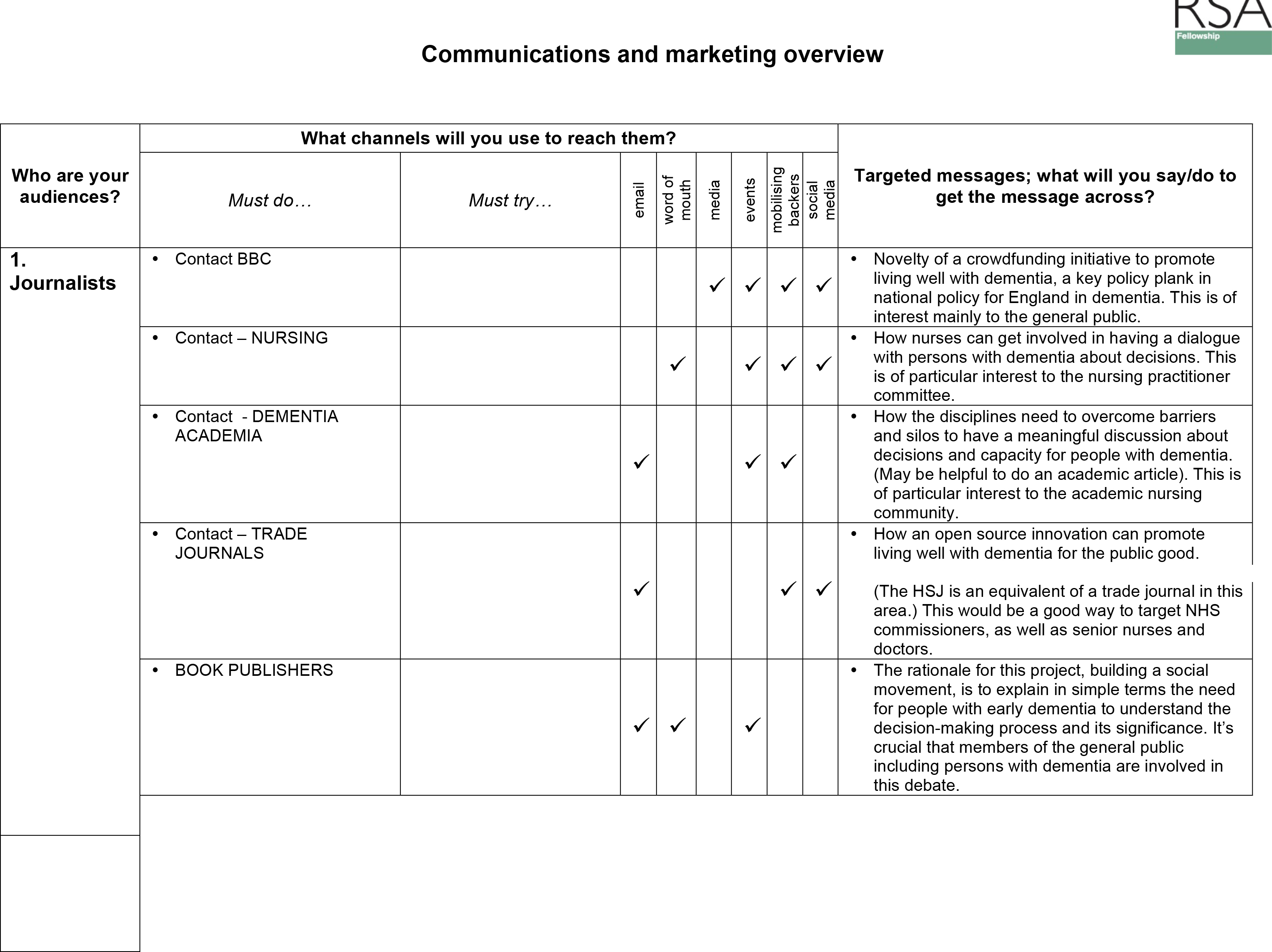
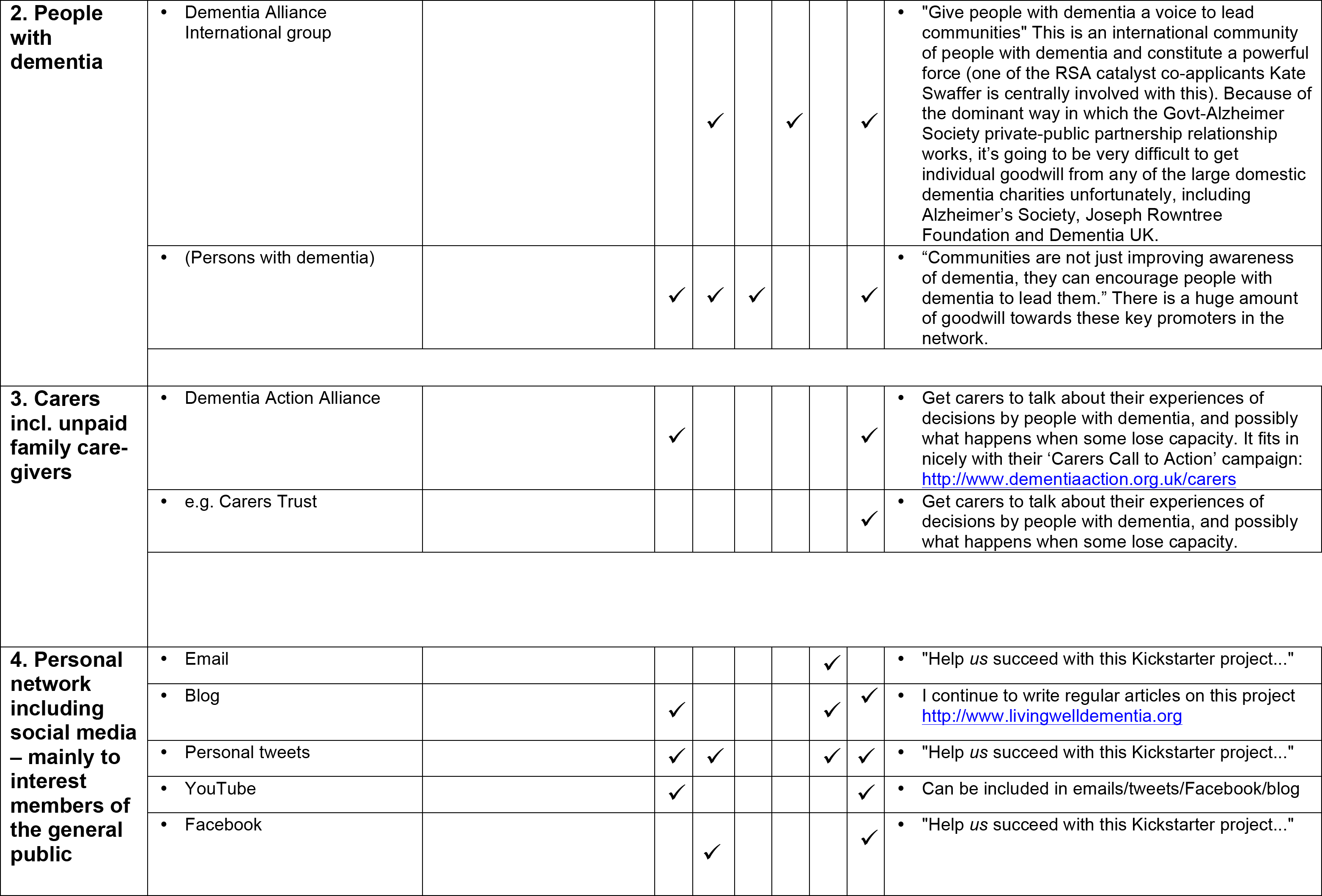
This is by the way how I intend to maximise use of marketing channels (some details redacted.)
I have previously discussed the Alzheimer’s Society Drug Discovery Programme video here.
About 13-14 seconds in, Fiona Phillips – who is actually an outstanding campaigner for dementia causes – says clearly, “Current treatments only help with symptoms for a short while.”
About 15-16 seconds in, Fiona Phillips says, “They don’t stop dementia from progressing“.
The current CEO of the Alzheimer’s Society is Mr Jeremy Hughes.
In the July-August edition of Journal of Dementia Care, volume 12, number 4, page 12, for 2013, Hughes states the following in response to an article by Dr Martin Brunet in the same journal.
And this has been clearly at odds with the NICE guidance.
Here is for example what the judicial review on these guidelines had demonstrated.
I must admit that this is only going from bad to worse.
Today, in the BMJ, Dr Peter Gordon wrote as follows in an article entitled, “No evidence exists that “anti dementia” drugs modify disease or improve outcome” (BMJ 2014;348:g2607):
“More than three months have passed since the G8 dementia summit was held in London, allowing time for critical thinking over its most laudable aim to “create disease modifying treatment to try to stop, slow, or reverse the condition.”1 This was less than a year after I gave an interactive talk based on one question: “What do we mean by Alzheimer’s disease?”2
In my talk I presented what evidence told us about currently available “anti-dementia” drugs, that, as yet, there is no conclusive evidence that they modify disease or improve outcome.3
In sharing this evidence with my audience of health professionals, many seemed to exhibit furrowed brows and looked at me as if I were an “outlier.” During and after my talk the evidence I presented was challenged by several of those who attended. These drugs, they confirmed, in their understanding, did modify outcome and that is what they told patients. It was further explained to me, after my presentation, that this was the “prevailing” understanding.
Leading world experts established at the G8 dementia summit that there was no evidence that existing drugs modified disease, and the World Health Organization director-general Margaret Chan summarised this for G8 in the following way, “in terms of a cure, or even a treatment that can modify the disease, we are empty-handed.”4
This story seems to show that my profession was perhaps not following evidence but, rather, wishful thinking and, indeed, mythology. I am left wondering why this happened and why such evidence was not properly shared with patients. It also occurs to me that industry, politicians, and national leads seem to have made little effort to challenge this “prevailing understanding,” at least until the “anti-dementia” drugs had largely come off patent.5 Our patients deserve better. They deserve truth. We all need to do better with that cherished and high ideal of informed consent.”
There is clearly something going wrong with the quality of debate about dementia from clinicians and non-clinicians.
I remember having immense difficulties with this issue in the final chapter (18) of my book ‘Living well with dementia’, as per the following extract:
It would be helpful to know if Mr Hughes has changed his mind between then and now, with the #G8dementia having intervened; of course it is possible that the Drug Discovery programme video is genuinely at odds with the views of Hughes. It is noteworthy that Pharma themselves are sending out different mood music concerning the efficacy of their “anti-dementia drugs” which I mention here in my G8 dementia summit survey blogpost.
All of this really does matter if we as academics with some knowledge about this area are to conduct the correct discussion about dementia on behalf of persons with dementia and carers including unpaid caregivers.
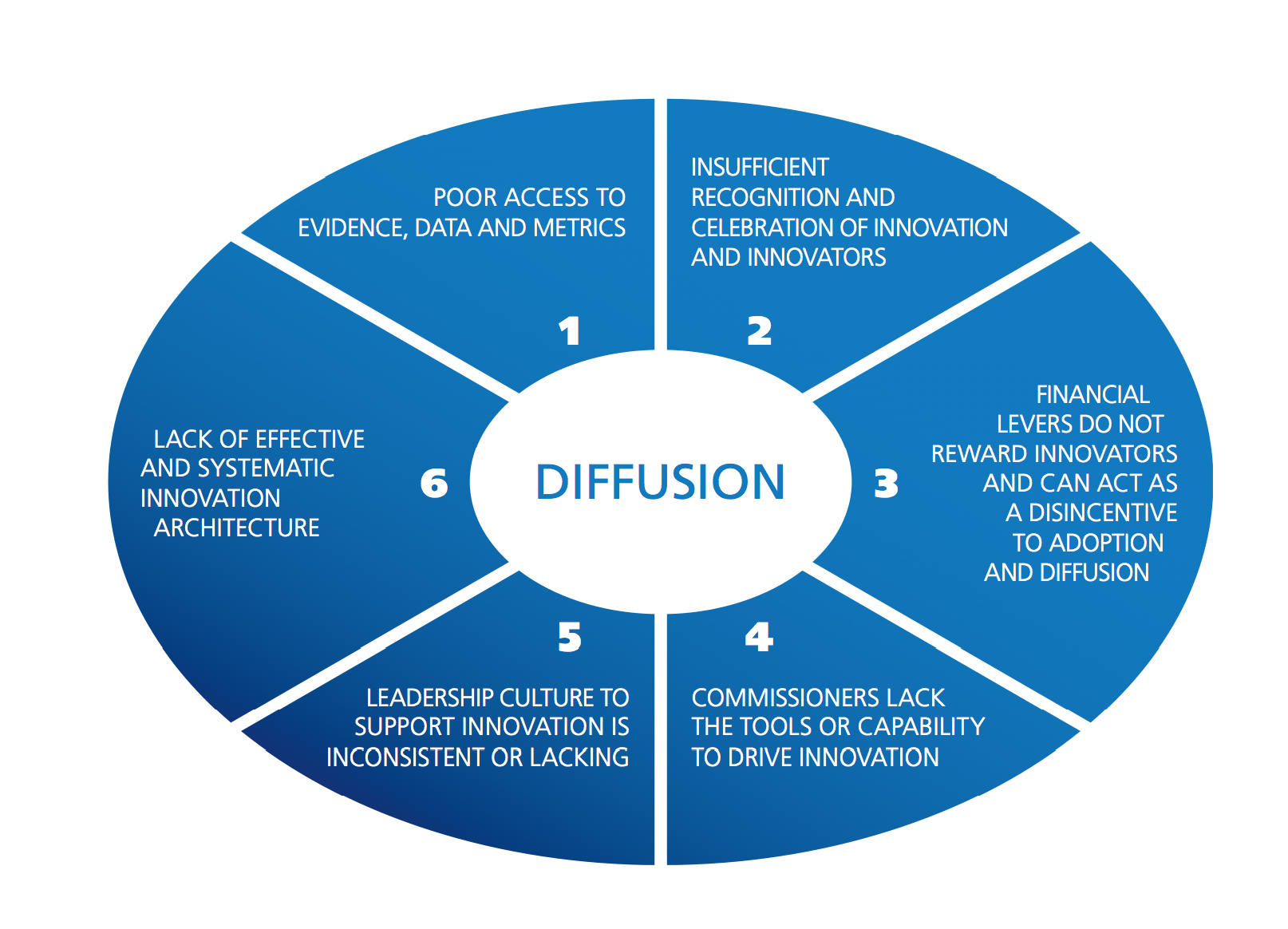
The barriers to innovation are well known. The report indeed provides a good synthesis of some of the more common barriers.
Simon Stevens, as NHS England’s new CEO, in identifying private healthcare firms as key players is bound to have produced fireworks.
Simon Stevens has highlighted “the innovation value of new providers” in the provision of health services. He said failure to appreciate that value was one of a number of issues the NHS collectively had got wrong.
This to me is a reasonable point, even if articulated somewhat aggressively.
For every good innovative idea, there are thousands of turkeys. For this, you need to take creative risks in a healthy innovative culture.
The NHS really has problems with talking risks particularly in light of the intense ‘zero fault’ memes sent out by Jeremy Hunt, the current Secretary of State for Health.
Also there’s another elephant in the room.
Many junior medics get through medical school without any training in any form of business management, let alone innovation management.
Innovation management is a rewarding field which I studied for my MBA.
It’s not simply doing ‘more for less’ as popularly espoused by self-appointed ‘entrepreneurs’ and ‘innovators’.
Therefore, measuring any beneficial outcomes in the NHS, and rewarding them is intrinsically difficult. For this, the NHS needs to be seen to rewarding and training properly its innovators.
Addressing an audience of 300 health professionals in Newcastle, Stevens said he was “struck by the misplaced consensus that seems to exist within the health service on various issues”.
There is also, though, a powerful consensus amongst some that the NHS “can’t do “innovation.
Drawing on his decade of experience in global healthcare working for the US company UnitedHealth, Stevens said: “Things that are assumed to be inevitable care delivery constraints here often turn out not to be in other countries.”
I don’t particularly know what Stevens’ motives are.
It could be that the present government wishes to promote social enterprises and mutuals, through longer-term investor tools such as social impact funds, so that multinational corporations can go into strategic alliances with social enterprises to compete with the NHS for contracts.
This might be consistent with “the critical role of the third sector, and the innovation value of new providers”.
Certainly, the private sector does an important rôle to play in innovations in dementia, such as assistive technologies and ambient-assisted living.
But the idea of outsourcing innovation to the private sector is one for me which lacks imagination, but will transfer resources from the NHS to multinational corporations and social enterprises.
I actually do not have an ideological objection to this, though many will do.
But I do find sad that Stevens has given a speech which acts as a powerful market signal to his intentions. It’s almost as if Stevens in one foul swoop has intimated that the NHS is incapable of “doing” innovation, and – even more dangerously – has ignored the progress which had been made.
Various funding mechanisms for long-term care for dementia have come under scrutiny, including private insurance, drawing on the experience of various jurisdictions (e.g. Hayashi, 2013).
An insurance contract is a contract whereby, for specified consideration, one party undertakes to compensate the other for a loss relating to a particular subject as a result of the occurrence of designated hazards.
The normal activities of daily life carry the risk of enormous financial loss. Many persons are willing to pay a small amount for protection against certain risks because that protection provides valuable peace of mind.
The term insurance describes any measure taken for protection against risks.
In an insurance contract, one party, the insured, pays a specified amount of money, called a premium, to another party, the insurer. The insurer, in turn, agrees to compensate the insured for specific future losses. The losses covered are listed in the contract, and the contract is called a policy.
You can often have more information than the person with whom you enter into a transaction – or vice versa. This is a potent phenomenon called “information asymmetry”.
Following the seminal work by Arrow (1963), the notion of information asymmetry have by now been recognised as a cornerstone of modern insurance theory.
George Akerlof was the the author of a landmark study on the role of asymmetric information in the market for “lemon” used cars.
His research broke with established economic theory in illustrating how markets malfunction when buyers and sellers — as seen in used car markets — operate under different information.
This seminal work has had far-reaching applications in such diverse areas as health insurance, financial markets and employment contracts. It could now impact on the way the National Health Service acts in the future in implementation of “needs based commissioning“.
Health economists, not least Prof Julian LeGrand of the LSE, in the frenzy of New Labour and subsequent English administrations have been hell bent on introducing a ‘market’ into the NHS. And this introduction of the market or ‘quasi-market’ has had a profound impact on resources and planning, as well as large charities.
According to numerous news reports, a global study involving more than one million people to look at the influence of genetics and lifestyle in Azheimer’s disease will be led by scientists from Cardiff University.
The £6m project will combine the power of multiple studies from around the world to explore the roles of genes and lifestyle choices to produce the most comprehensive understanding of the disease’s risk to-date.
Information gathered by researchers from across the globe will provide scientists with the best evidence yet for creating a fuller picture of why the disease develops and the degrees of risk it poses to different individuals.
This study clearly has implications for the future.
Sir David Nicholson spotted these implications at once.
@legalaware this coupled with data coming from genetics means that whole pop risk pools supported by tax funded systems is the future
And in fairness David‘s starting point is fundamentally one of universality.
CCGs, or clinical commissioning groups, do not particularly need to be manned by clinicians, though that it is how the concept has continued to be marketed to the public and GPs. They are simply state-run populations pooling risk, and there has never been any precise guidance on their exact size (in terms of number of people in each catchment).
Aim
With such recent upheavals in health policy in England, with discussion of an insidious ‘privatisation agenda’, this online survey was undertaken with a view to working out whether members of a general public exhibited views with the functioning of private insurance markets.
Methods
I completed a study. Respondents were invited from my Twitter account @legalaware with close to 12000 followers.
I used ‘SurveyMonkey’ to carry out this survey. With ‘SurveyMonkey’, you cannot complete the survey more than once.
There were 125 respondents in total.
The sample is possibly biased, in that I have a predominantly left-wing follower list consisting of about 11000 followers of mainly well-informed people.
Exclusions
None.
Results
However, in fairness, it is worth noting that certain key policy planks have cross-party support, including free-at-the-point-of-need and personal budgets.
A rebuttable assumption of universality
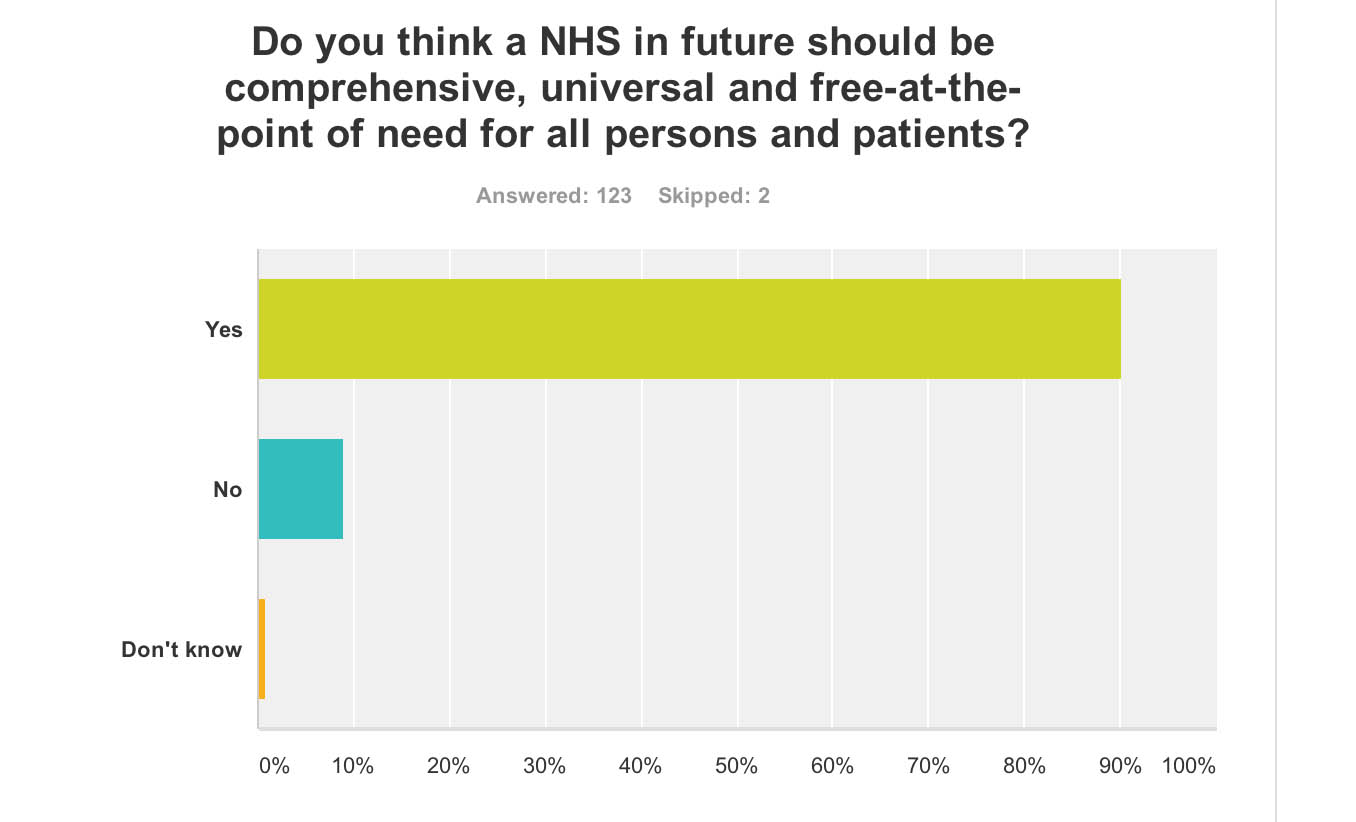
In answer to “Do you think a NHS in future should be comprehensive, universal and free-at-the-point of need for all persons and patients?”, 99% answered yes (n = 123). The problem with this is that opinions about the extent to which the NHS offers a comprehensive service is qualified by some degree of ‘rationing‘ already.
However, I did ask “Do you think the NHS of the future should be wholly funded out of general taxation?”. I used the word ‘wholly’ meaning completely. Despite this high threshold, 79% said ‘yes’ (n = 126).
The NHS provides the majority of healthcare in England, including primary care, in-patient care, and long-term conditions. The National Health Service Act 1946 came into effect on 5 July 1948. Private health care has continued parallel to the NHS, paid for largely by private insurance, but it is used by less than 8% of the population, and generally as a top-up to NHS services.
A number of various solutions to the NHS “funding gap” continue to be produced – see for example Wilby (2004) here in the Guardian:
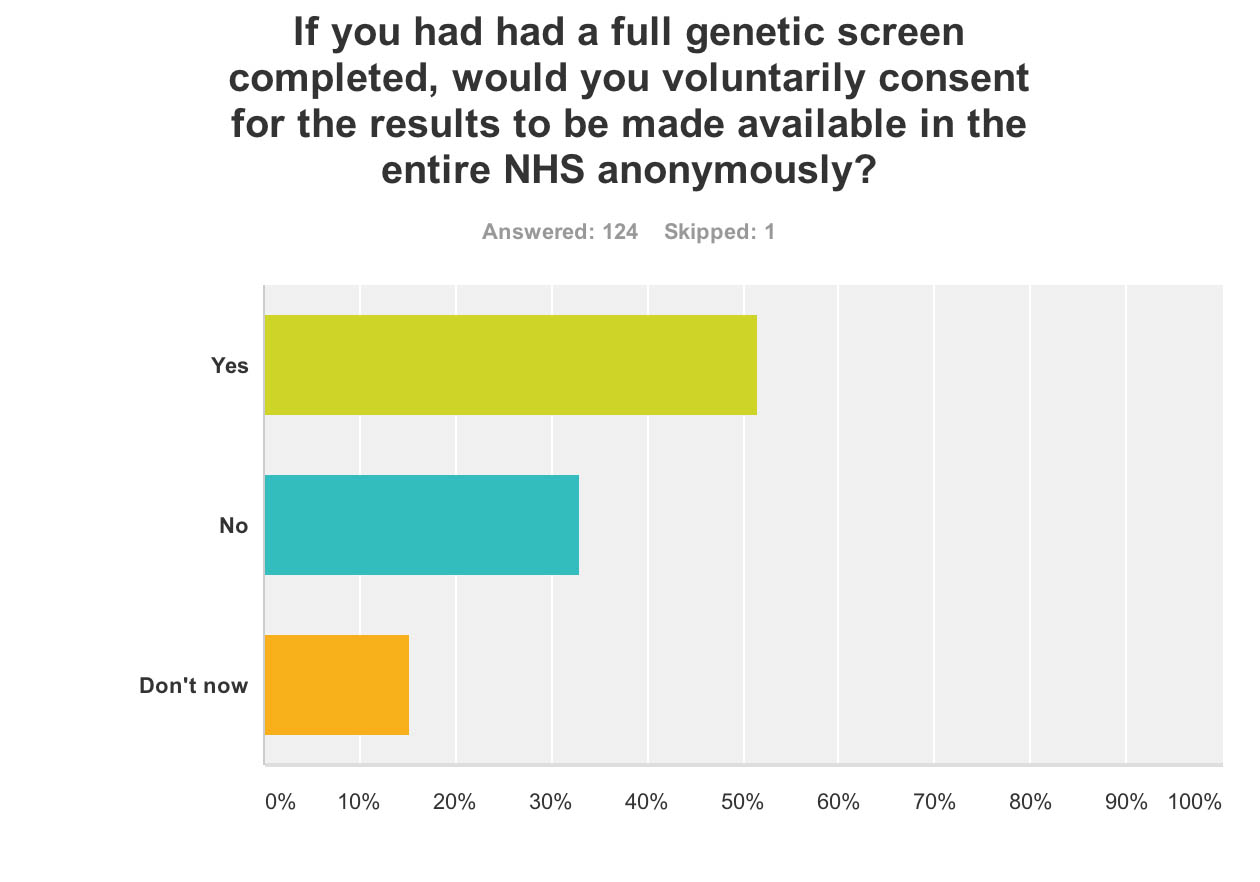
Data sharing of genetic risk within the NHS
I also asked, “If you had had a full genetic screen completed, would you voluntarily consent for the results to be made available in the entire NHS anonymously?” This produced a very mixed response: yes – 52%, no – 33%, don’t know – 16% (n = 124).
This is interesting in light of the ‘case finding’ approach in England, where a possible diagnosis of dementia might be chased up even if not initiated by the person directly involved, exacerbated perhaps in the drive from politicians and the Alzheimer’s Society for improved diagnosis rates.
It could be that the recent furore over care data, through the subject being badly managed by NHS England with the general public, may have impacted on this general lack of willingness of a member of a general public to share details of a genetic screen with the NHS at large.
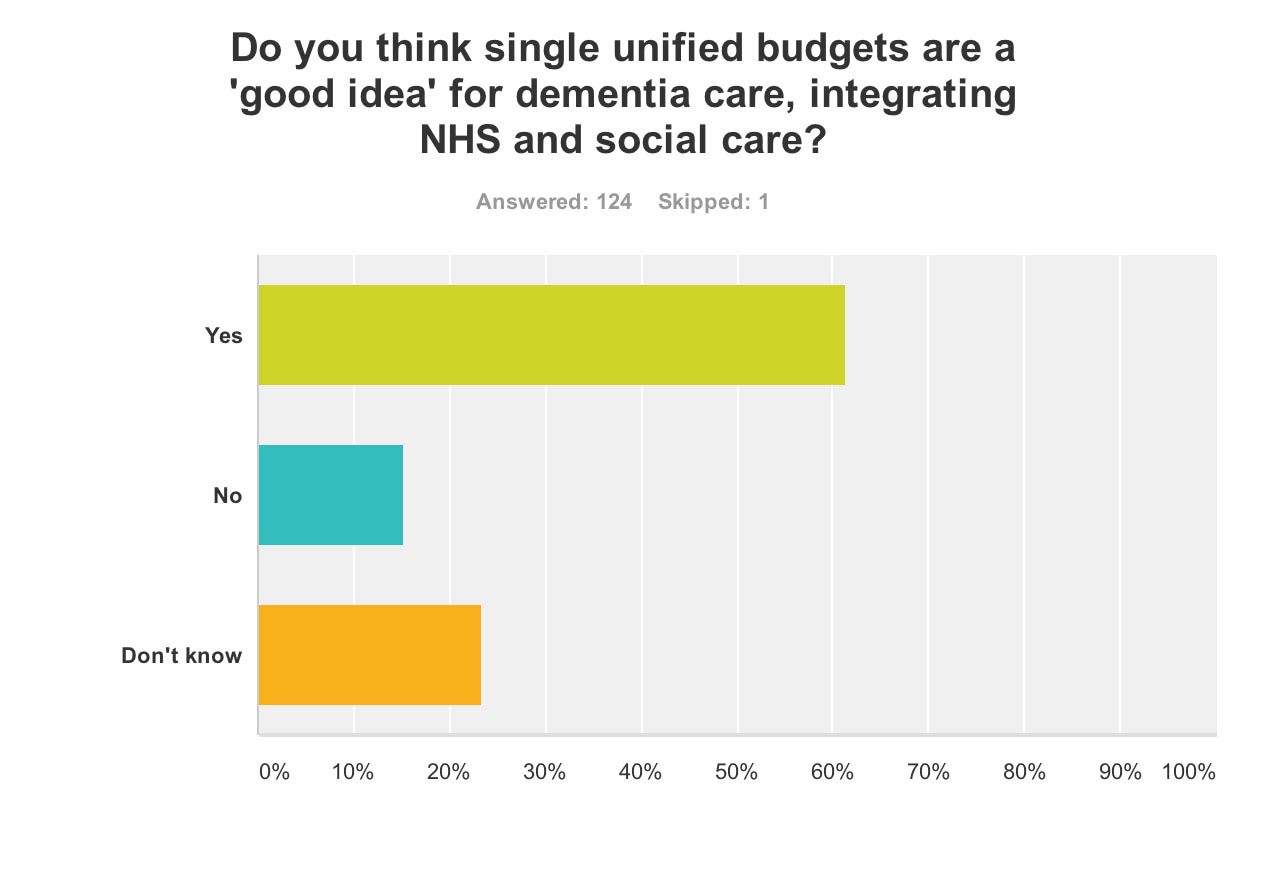
Single unified budgets
A consistent policy strand of late has been the desire to introduce personal budgets for dementia (and this is across all main political parties).
I asked, “Do you think single unified budgets are a ‘good idea’ for dementia care, integrating NHS and social care?”, and it is noteworthy that the majority (61%) said yes, with only 15% saying no. The proportion saying they don’t know (23%) constitutes, though, a sizeable minority (n = 124).
Taken with the above finding with the general popularity of universality, one might infer that people generally don’t want to see single unified budgets as a backdoor mechanism of introducing care for which you have to pay extra.
The uncertainty for this is indeed interesting.
The recent interim report from the King’s Fund “Barker Commission” (2014) on the future of health and social care made the following observation:
“If they become widely adopted, it is difficult to see how anyone could be prevented from topping them up – that is, buying additional health care privately that goes beyond the agreed package.”
Nonetheless the notion of a ‘shared budget’ continues to gain traction. McNeil and Hunter (2014) in their recent IPPR report comment:
“More third-party organisations, such as community groups, faith organisations, mutual support groups and micro-enterprises should be invited to take on responsibility for developing packages of care and support for individuals in this way if they meet certain core criteria.”
And so – therein lies the crunch. The devil lies in the detail?
Information asymmetry and markets
Profiling someone’s risk is exactly how private insurance markets work.
They process your dividend according to your risk. There are concerns that the NHS is heading towards a private insurance system, if only to be integrated fully with one.
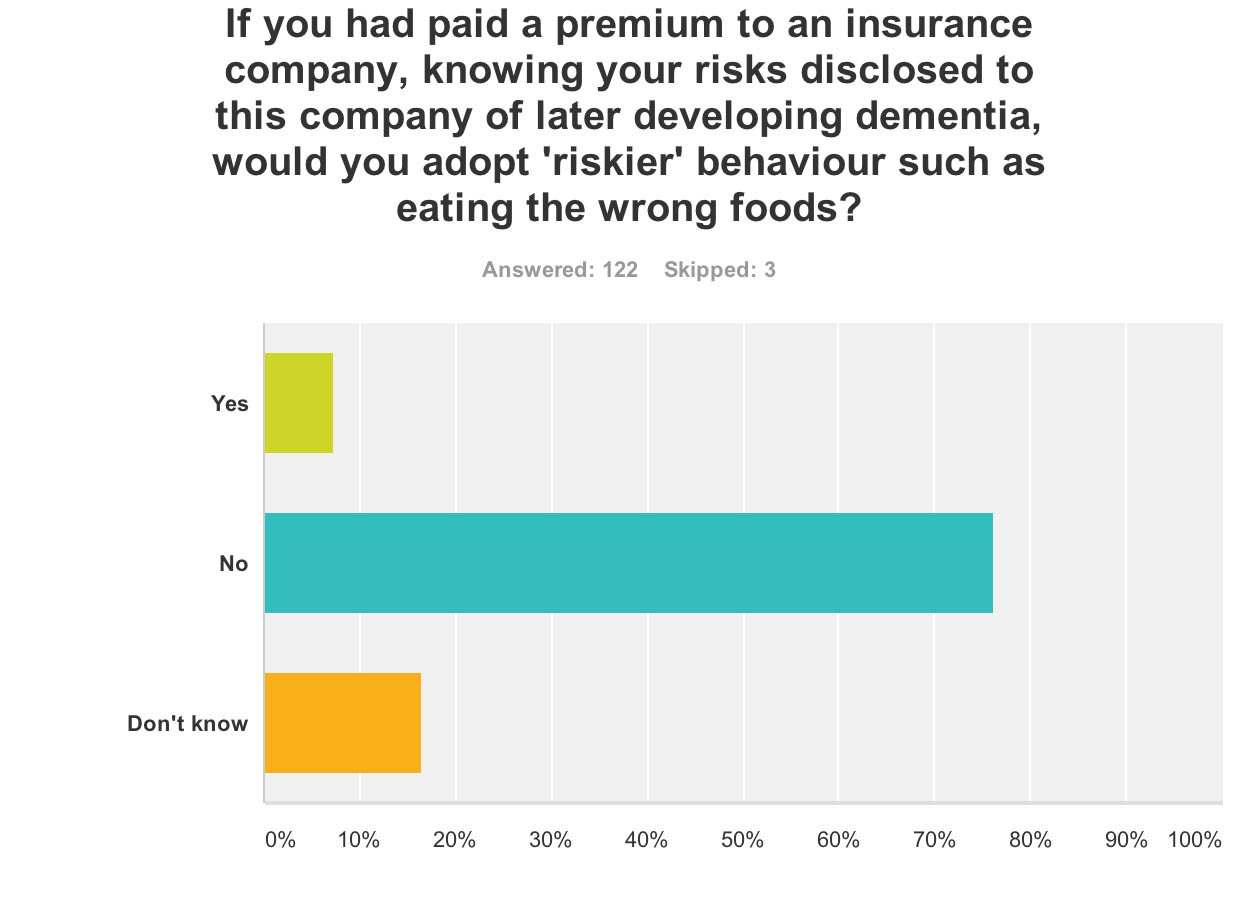
Moral hazard
The question “If you had paid a premium to an insurance company, knowing your risks disclosed to this company of later developing dementia, would you adopt ‘riskier’ behaviour such as eating the wrong foods?” produced a very interesting observation.
This is “moral hazard”.
In economic theory, a moral hazard is a situation where a party will have a tendency to take risks because the costs that could result will not be felt by the party taking the risk. In other words, it is a tendency to be more willing to take a risk, knowing that the potential costs or burdens of taking such risk will be borne, in whole or in part, by others. A moral hazard may occur where the actions of one party may change to the detriment of another after a financial transaction has taken place.
7% said yes, but 76% said no (17% said don’t know) (n = 122).
This for me demonstrates that the general population in this scenario does not behave like a typical insurance market for goods, and this could be something to do with a person will not wish to take risks with their personal health irrespective of the scientific evidence.
And in fairness, a genetic risk for dementia might not be nearly as important as environmental factors for someone developing a dementia, and people are reluctant to take risks with that.
Adverse selection
I asked, “If the outcome of a genetic screen was that you had an extremely low risk for dementia, would you seek to purchase private health insurance where your premiums might be very low?” Amazingly, despite 21% of respondents saying yes, 56% said no and 23% said they didn’t know (n = 123).
This is “adverse selection”.
The term adverse selection was originally used in insurance. It describes a situation wherein an individual’s demand for insurance (the propensity to buy insurance and the quantity purchased) is positively correlated with the individual’s risk of loss (higher risks buy more insurance), and the insurer is unable to allow for this correlation in the price of insurance.
Limitations
All respondents were in the UK.
There might have been political bias in the sample, though it is useful to note perhaps that personal health budgets and a comprehensive universal NHS, free at the point of need, have currently cross-party support.
Conclusion
Clearly a much larger sample is going to have to ascertain what these trends are.
There is no doubt that the furore over care data sharing and the policy to improve diagnosis of dementia rates will have a legacy on future dementia policy, and possibly a very negative one.
And finally, evidence from moral hazard and adverse election demonstrate that individuals assessing their risk for dementia may not behave like traditional insurance markets.
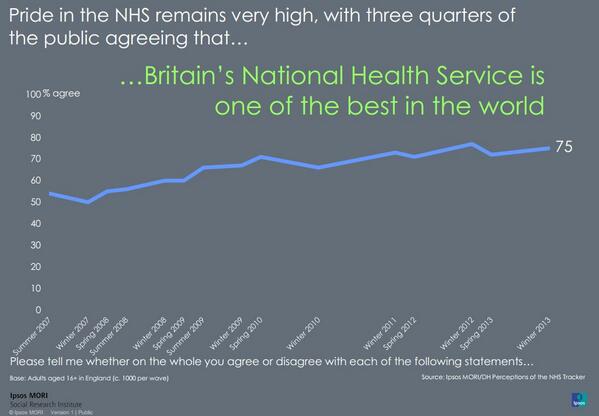
Reasons for this might include the facts that adults in fact prioritise their own health and do not wish knowingly to put it to risk, they appreciate the rôle of factors in the environment which could throw havoc for insurers’ calculations, and that they have a deep-felt genuine ‘brand loyalty’ and affection for ‘that national religion’, the NHS.
This is all very problematic if the ultimate goal for increasing awareness of dementia was to boost the private insurance industry and Big Pharma. It looks as if the NHS might have the last laugh after all.
References
Arrow, Kenneth J. (1963) “Uncertainty and the Welfare Economics of Medical Care”, American Economic Review 53 (5), pp. 941–973
Hayashi, Mayumi (2013) The lessons Japan has for the UK on dementia, The Guardian (link)
McNeil, Clare, Hunter, Jack [for IPPR] (2014) “The generation strain: collective solutions to care in an ageing society”, link here.
Wilby, Peter (2014) The NHS needs a life-saving idea – how about a health tax? The Guardian (link)
This was the famous selfie from the Oscars which went viral all over the internet, partly thanks to social networking sites such as Twitter.
But this snap photo explains why Liza Minelli was unable to make it.
That things might not be quite as they first appear is nothing new.
Kate Swaffer (@KateSwaffer), living with dementia in Adelaide, has remarked in the past how she feels like a duck all serene on the surface, but paddling really hard underneath.
The co-production of public services has been defined in a variety of ways – e.g. “Co-production means delivering public services in an equal and reciprocal relationship between professionals, people using services, their families and their neighbours” (New Economics Foundation).
Or in the alternative, “the public sector and citizens making better use of each other’s assets and resources to achieve better outcomes and improved efficiency” (Governance International).
Research into dementia, more so following the G8 Dementia Summit, has been dominated by analysis of Big Data genetics with a view to ascertaining risk pools and personalised medicine, possibly means for asymptomatic screening or early detection, and new pharmacological interventions.
The amount of resource allocation put into this some might say has not been matched by the successful outcomes from this research, though the corporate capture in the large charity, politics and media are well known.
But I believe strongly research into quality of care, or indeed living well with dementia in support settings, should not be regarded as ‘inferior’.
Careful research attention should be put into assistive technologies, assistive living, the innovation culture, design of wards and homes, and, of course, how you measure living well in the first place.
Co-production, however, offers a chance for people with early dementia to be able to shape the services for care, as well as to shape research.
I have latterly become involved in a crowdfunding campaign where I explain the critical importance of decisions for a person with dementia in the science of dementia as well as the implications for our law on mental capacity.
But I also want this to initiate a dialogue between people with early dementia and other interested parties with the law and neuroscience, and other possible stakeholders such as the NHS.
I’m mindful that my book ‘Living well with dementia’ does look through the “personhood lens” – a lens which has done much to challenge the stigma and discrimination associated with dementia – and some people don’t like that.
Darren Gormley (@mrdarrengormley) immediately pointed me to an area of work, in particular a paper called “From personhood to citizenship: Broadening the lens for dementia practice and research” by Ruth Bartlett and Deborah O’Connor in Journal of Aging Studies 21 (2007) 107–118.
“One of the main boundaries of personhood is its lack of political dimension. In cognate literatures, including social gerontology, critical psychiatry and disability studies, a citizenship lens is used to promote the status of discriminated groups of people to that of an equal citizen, with the same entitlements as everyone else.”
“These disciplines use citizenship to understand and expose discrimination against marginalized groups such as people with physical disabilities and to reframe and politicize understanding of the experiences of people with mental health conditions; the scope of this work is wide ranging and goes beyond care issues to include discrimination in the workplace and communities generally.”
The need to promote citizenship, as well as personhood, is beginning to be recognised within the dementia care literature, and I am hoping that this with an emphasis on living well with dementia will percolate into the research arena too.
A result of this shift is that, gradually, research has begun to emerge aimed at capturing the perspectives of persons with dementia. This body of research now clearly documents that persons with dementia are often quite aware of their situation, and can contribute important and unique insights about their experiences and needs.
“In addition, people with dementia were generally regarded as a ‘sufferer’ lacking insight into, and ability to articulate, their situation. This discourse silenced people with dementia. However, since attention was drawn to personhood and the exclusion of the perspectives of persons with dementia in understanding and influencing the dementia experience the focus has shifted to incorporating the voices and understandings of persons with dementia into both research and practice.”
However, my own particular interest is research for dementia, so this intrigued me massively since, if you pardon my phraseology, some of my best friends live successfully with dementia.
“The importance of making the shift to citizenship is further evidenced when one considers the potential direction of dementia care research. Currently, Alzheimer’s Society, UK has people with dementia on its research review panel, and there is a small (growing) body of literature to help academic researchers involve people with dementia more creatively in the research process.”
“People with dementia are clearly seen and treated as important players in the research process. However, little of the research looking at user perspective has gone to the next step of either pulling together or examining what happens in research projects in a way that is political.”
“For example, in most user perspective studies, individual needs are spoken of and contextualised using themes or general categories related to care provision; data are not generally seen in the wider political context of the need for social change.”
“Additionally, people with dementia are rarely involved in the early formulation and planning of projects, which raises questions about the relevance of current research to people with dementia. The point is not to criticize user perspective studies but to highlight how a shift to citizenship would ensure people with dementia were seen and treated as people with power, specifically people with the power to instigate and shape the research agenda.”
And that for me is the issue of a two tier nature of who decides research agendas in practice.
Kate Swaffer and I often discuss behind the scenes our concerns about ‘tokenism’, both from quite different personal viewpoints but with similar themes.
How things appear might not actually how they are in reality.
And I’m clearly bound to be very happy that currently there’s a massive ESRC grant looking into this.
“Finding that people with dementia are willing and able to campaign, and presenting this at national and international conferences, has captivated academics and improved their understanding of people with this condition.”
This also has profound implications for service development for dementia consistent with the current trajectory.
A rhetoric of ‘user involvement’ became a central part of NHS policy during the establishment of the Community Health Councils in 1973. This had continued through the proliferation of “New Public Management” principles and the growing importance of measures of satisfaction in the 1980s. The NHS and Community Care Act[1990] established a formal requirement for service user involvement in service planning.
From 1997, patient and public involvement were a central tenet of New Labour’s NHS modernisation agenda, and the NHS Plan was committed to creating a patient-centred NHS with user needs at the centre of service design and delivery.
Arguably, the roots of the phenomenon of ‘experts by experience’, potentially an abreaction to the medicalisation of mental illness, can be found in a history of mental health activism as far back as 1620, when inmates at “The Bedlam Asylum” petitioned for their rights.
After some initial disgruntlement, I’ve now decided I would never dream myself of being an ‘expert’ in anything to do with dementia, but rather a well-informed enthusiast.
People living with dementia and all carers including unpaid caregivers are the real experts.
The somewhat political term “survivors” refers to those who have survived not only their mental health difficulties, but also experiences of psychiatric services, and/or the accompanying general social exclusion.
Or you can the viewpoint, particularly if you’ve been influenced by some, that ‘users’ of mental health services are ‘consumers’ and help to design them.
A lack of co-production possibly caused the problems in entitlement and funding which meant Sally (@nursemaiden) was at the receiving end of a bad experience of services looking after her father who was living with dementia.
@RichardatKF@legalaware Thank you Richard I still feel at times I let him down that I should have fought harder against the system.
In fact Sally has written about this in the Foreword to my book.
What unites both the consumerist subject position of service user and the position of “survivors”, is that they are both legitimised by virtue of their experiences of mental distress and/or of service (ab)use, and seek progressive developments in the treatment, perception and governance of the experiences of mental health.
I’m one such survivor, as I’m in recovery from alcoholism for seven continuous years now. I also live with physical disability.
It’s not enough merely to ‘involve’ carers though; carers patently need to be involved in research as without them the entire service would collapse. And carers themselves often need support, over all sorts of health issues, legal or financial matters.
It’s also essential to ‘involve’ people actually living with dementia who may or may not have some similar concerns, and some different.
But ‘involving’ is not enough.
I feel passionately that people with early dementia should be given the power and control to shape the research agenda in their interests, such as the brilliant work by Ruth Bartlett. This may or may not include living well with dementia: that’s not my choice, but I’m pretty sure I know what the answer might be. Otherwise, ‘co-production’ is merely an illusion of involvement, and as regards living well with dementia is not at all what it seems. Suffice to say, I am not afraid about shouting loud about this on behalf of people living well with dementia.
The thing is, I don’t buy into the profoundly negative imagery of the media, including memes such as “crippling”, “horrific”, “timebomb” and “explosion”.
Whilst some people, and caregivers, are undeniably “suffering”, you can’t expect all people to agree with this particular narrative at all times, I feel.
One of the things I’ll never forget was when my Ph.D. supervisor, Prof John Hodges, received a complaint about me doing neurocognitive assessments in a person with frontal dementia back in 1997.
This type of dementia, commoner in an age group below 60, is characterised by a personality and behavioural change early on, often in the absence of deficits in thinking such as memory or perception. You need an account from someone very close to that person with dementia, as the person himself or herself can have no insight into the changes.
I remember saying to the wife of a young man with this type of dementia, “I would never have guessed that he had a dementia”. This comment had upset her very much, and by that stage I was years into my medical training.
This one event is something I’ve never forgotten in the 16 years subsequently.
I remember I literally didn’t sleep for a week, and I was profoundly upset by this. But it does lie to the heart of some of my reservations about the term ‘dementia friendly communities’. There are some people for whom you would not be able to tell they were living with dementia.
I understand the focus on memory problems in the general media, as this can be a dominant presentation in typical Alzheimer’s disease, the commonest form of dementia. But memory is only one of the cognitive functions we have.
What unites all people with dementia is that the law makes a verdict on whether they are able to make decisions. This is called legal capacity.
Decisions impact on many aspects of life, such as working out how to spend your money, or which treatment to go for in hospital.
And capacity is very topical. Not only is the House of Lords seeking to update the Mental Capacity Act (2005), but also neuroscientists currently want to know what members of the public think about their research on decisions.
This is therefore not about denying compassion or dignity for all persons with dementia. It’s about redressing a power balance, where I feel people who’ve just received a diagnosis of dementia might learn something constructive about dementia, decisions and science of how to influence decisions.
This is profoundly about having a discussion with persons with dementia.
I’ve been on the receiving end of ‘look at my website’ and I find it intensely nauseating. But I wish my website, which I intend to build with funds from a crowdfunding campaign and scientific grant bodies, to allow persons with dementia to think about their own decisions.
It’s well known in the science of decisions for example that some ‘bad’ decisions can be avoided by not following ‘hot impulses’ or following the ‘herd effect’.
So here is my explanatory video:
Whilst I have been urged to make this campaign so that ‘it touches every person with dementia’, I do also want a grown up conversation without dumbing down any of the concepts.
A lot of feedback has concentrated on the ‘social movement’ aspect of it, but I should like to say whilst I say I would like to build one, I really mean it’s important for me personally that this gathers some momentum.
And I think it will from initial feedback from persons with dementia, and even people involved in the NHS and social care.
All too easily dementia policy can have more regard to marketing and tokenism, which lends itself to commissioning ‘tick box’ culture. My campaign is not for them.
And I’ve got a bit of a shock for some people – I am determined to make a big success of it.