I received this morning my copy of “What the hell happened to my brain?” written by leading international advocate in dementia, Kate Swaffer. This book is due to be released by Jessica Kingsley Publishers on January 21st 2016. I received an advance copy as I wrote one of the Forewords. The other Forewords have been written by Dr Richard Taylor Ph.D. and Glenn Rees AM Chair of Alzheimer’s Disease International.
Kate is Chair of Dementia Alliance International, the international stakeholder group run by people living with dementia. I feel this book will be incredibly useful for a diverse audience, including doctors – especially those completing specialist training in medicine (general medicine, neurology, psychiatry, surgery especially) – as well as members of the public newly diagnosed with dementia.
I know Kate Swaffer held Dr Richard Taylor Ph.D. in very high esteem. I found the chapter dedicated to him, and his Foreword, very moving.
This book is all about living ‘beyond a diagnosis of dementia” – Kate’s phraseology TM. Kate was the first to articulate and explain the phenomenon of ‘prescribed disengagement’ how people at the point of diagnosis are often put into a process of managed decline when they could be given opportunities for an enriched life. This of course goes together with essential practical help, such as things you can do such as driving. It also explodes myths out of the water – and ignites a provocative debate on the ‘big money’ in dementia, disability discrimination, an urgent need to rework the medical label of ‘challenging behaviours’, early vs late diagnosis, stigma, loneliness, inclusion, and guilt.
It’s not hyperbolic, nor puffery, to claim that you won’t be able to put this book down. It’s an outstanding book, and I strongly commend it to you.
It’s well known that I survived a six week coma on the Royal Free ITU in 2007, after having had a cardiac arrest and respiratory arrest simultaneously.
I am only motivated doing my work promoting wellbeing for people beyond a diagnosis of dementia (TM – Kate Swaffer’s term), and motivated by my mum’s happiness.
The lyrics of David Bowie’s “Lazarus” have enormous personal significance for me.
Look up here, I’m in heaven
I’ve got scars that can’t be seen
I’ve got drama, can’t be stolen
Everybody knows me now
Look up here, man, I’m in danger
I’ve got nothing left to lose
I’m so high it makes my brain whirl
Dropped my cell phone down below
Ain’t that just like me
By the time I got to New York
I was living like a king
Then I used up all my money
I was looking for your ass
This way or no way
You know, I’ll be free
Just like that bluebird
Now ain’t that just like me
Oh I’ll be free
Just like that bluebird
Oh I’ll be free
Just before christmas, I made a quick tweet as follows.
Since then, I have watched this tweet progressively get retweeted to the point of ‘going viral’. At the time of writing, it has had 287 ‘retweets’ and 250 ‘favourites’.
Of course, no one can predict how, why, or when a tweet might go viral, though plenty of people have speculated on this phenomenon. Here is one example.
In case you missed it, the story begins as follows.
“Pianist Edward Hardy played in a jazz quartet for almost 40 years but had no one to play with after being moved into a care home following the onset of dementia.
Care home worker Sam Kinsella helped him post an online advert to bring in musicians to jam with the talented war veteran.”
The home in Somerset, was inundated with more than 80 requests from across the UK, including from three former band mates who he hadn’t seen for 35 years. Mr Hardy had set up his first band when he returned from serving in Japan in World War II, but had become depressed when he recently moved into the care home initially leaving his wife for 75 years, Betty, 91, at home, and was diagnosed with dementia.
Apparently, he has remembered the skill of playing music and “play it so well and it’s like everything comes back to him when he’s on the piano.”
I think one of the things which most surprises me about life in general is how binary or polar things can become. One person’s valid scoop is another person’s political manipulation. Decisions we make are simplistically ‘Marmite’.
I don’t believe you can wake up one morning ‘with dementia’, when you didn’t ‘have it’ on the previous day. I do think it’s possible for fit the criteria one day with you not having met them previously. This brings up the issue of how we define the various dementias.
And the diagnosis does matter. For example, if you get re-diagnosed as ‘minimal cognitive impairment’ instead of dementia this can make quite a big impact on your life, especially if you have lived for years as a person with dementia.
I don’t think NHS England appears to care enough about validating or confirming diagnoses of dementia. I have been surprised by how many people living with dementia are not sure where the diagnosis came from, nor even who made the diagnosis.
But I do worry when there are powerful external factors at force. I think we get onto dangerous territory if you incentivise doctors financially into making a diagnosis. This NHS England policy was not only unethical, but morally repugnant. I agree on the need to ‘close the diagnosis gap’, but I do not agree on giving people who don’t have a diagnosis of dementia a diagnosis.
Overall things, though, are going well. There’s much more meaningful involvement, as opposed to meaningless involvement, of people living with dementia and carers now in research and service provision. I really do wish England and Wales well if they develop a working group in the future. The Scottish lead has been very useful here.
Scotland often, I feel, leads England through the work of Alzheimer Scotland. For example, there is a much more coherent construct of integrated care through their “eight pillars”. In comparison, efforts through the Better Care Fund in England have been piecemeal, unpredictable and sometimes unimpressive.
Scotland now, I feel, can strengthen their lead on human rights. Their influence on Alzheimer Europe is not insubstantial, but Alzheimer Europe can become emboldened on taking a lead on human rights as Netherlands assumes the Presidency from Luxembourg.
I wish to applaud Prof Peter Mittler for his brilliant work. From my viewpoint as an academic, it will be hugely useful if we can look at quality of life and wellbeing in the WHO sustainable cities. I have high hopes from the Dementia Alliance International, and I am genuinely enthused by the lead taken by Glenn Rees recently appointed as Chair of Alzheimer’s Disease International.
With human rights, you get them all. You can’t choose, as such, which rights apply to you. Thanks to the UN, they all do under the UN Universal Declaration of Human Rights.
But things might not be all or nothing ultimately for personal budgets. The power of the National Health Service comes from a comprehensive service, free at the point of use, but this is undermined if there is creeping rationing of services (possibly at the individual level through personal budgets).
Things might not be all or nothing if a universal NHS is somehow bolted onto a means-tested social care framework. We’ve got to stop airbrushing ‘social care’ into ‘and care’, and we’ve got to think about pumping money into social care, into promoting wellbeing.
I dare say the binary articulation of the debate is what ‘campaigns department’ of Big Charity advises – a simple message which is easy to brand or sell.
I am very honoured that the main foreword will be by Prof Sube Banerjee, Chair of Dementia at Brighton and Sussex Medical School.
Sube is very influential in English dementia policy. His contributions have been outstanding. Indeed, he co-authored the original English dementia strategy ‘Living well with dementia’ in 2009 on behalf of the Department of Health.
I am very honoured that the other two forewords are to be by Lisa Rodrigues and Lucy Frost, who have substantial interest and knowledge in dementia.
The book will be a timely look at the evidence, with many of the topics being rehearsed elsewhere in policy, such as the NHS Five Year Forward View, or the NICE guidance on dementia (currently in development).
This book is likely to be published by Jessica Kingsley Publishers in the end part of 2016.
Chapter 1 : Overview
I will draw on the existent literature to consider what has emerged about a consensus about ‘care pathways’ for dementia, in particular the events which can lead up to “crises” or transfer to a residential settings. There has not been an adequate look at the work up in primary care for dementia, and I will consider how domestic policy might be harmonised with international guidance. In the presence of an evidence base for dementia advisors and dementia support workers, I will consider the potential of signposting to services. I will re-visit the evidence base for prevention of dementia, and the current evidence base for the use of cholinesterase inhibitors and other drugs, but will concern myself with the impact of human rights, disability and sustainable communities in current thinking. The largest part of this chapter will be considering quality of care, and novel approaches such as integrated personal commissioning and the personal medical care home. Throughout the book, there will be a detailed discussion of the need to promote the health and wellbeing of carers, both paid and unpaid, and to consider coping strategies which might help through clinical specialist nurses and social care practitioners, and other colleagues.
Chapter 2 – The caring environment and culture
This chapter will explore evidence for the components of the built environment and sensory stimulation and enhancing person and relationship centred care which enhance health and wellbeing across care settings. The main emphasis will be on considering what change might be needed, and under what leadership from all stakeholders, to ‘improve’ services, howeverso defined, and the rôles that risk and innovation might play in the future. If there are truly ‘no more throwaway people’, this chapter will also include how the social capital from people with dementia and carers might be consolidated to build more resilient communities co-designing research and services.
Chapter 3 : Physical health and aspects of pharmacy
Enhancing physical health is essential across all different care settings. This chapter will review the current evidence for management of falls, frailty, pressure sores, urinary tract infections, and hip fractures, as well as aspects of nutrition and metabolic medicine, from a multidisciplinary perspective, emphasising the role for allied health professionals. Aspects of prescribing will also be considered, including overuse, underuse and inappropriate use of medications, and what evidence base has thus far built up in the area of ‘therapeutic lying’ and its ethical implications.
Chapter 4 : Wellbeing and mental health
This chapter will consider aspects of mental wellbeing, including self and identity, and awareness and insight. Its will also consider various other issues to do with mental health, including agitation, apathy, depression, and sleep.
Chapter 5 : Cognitive stimulation and life story
A substantial evidence base has built up concerning non-pharmacological approaches to dementia. This chapter will consider diverse approaches including cognitive stimulation, reminiscence work and cognitive neurorehabilitation. This chapter will also consider the evidence base for ‘life story’ and how it has been approached across various care settings.
Chapter 6 : Oral health and swallowing difficulties
This chapter will consider a much neglected area of health and wellbeing, relevant to holistic health and wellbeing, that of oral health and disease. Current important issues in this field will be considered, including dysphagia and mastication, as well as possible areas of interest for the future.
Chapter 7 : Activities
This chapter will evaluate critically what exactly is meant by the term ‘meaningful activity’, and consider whether reframing of the narrative, such as promoting creativity’ might be more helpful. The chapter will discuss the importance of communication across this area, but consider specifically the arts, drama and theatre, dancing, gardening and outdoor spaces, humour, and music.
Chapter 8 : Spirituality and sexuality
Identity and relationships have emerged as key themes across various conceptualisations of personhood, including of course Tom Kitwood’s. This backdrop will be presented at first, before considering key issues in sexuality, spirituality and religiosity, not only in life after a diagnosis, but also for enhancing health and wellbeing across all health and care settings.
Chapter 9 : Research, regulation and staff
Research and regulation are examples of ‘work in progress’. This chapter will consider the key directions of research in the dementias, both qualitative and quantitative, across various care settings. This chapter will also consider specific areas of interest, including barriers to drug development including regulation. The overall area of regulation will be considered in terms of proportionality, and celebrate areas of good practice. The chapter will also consider areas which also are of utmost importance such as abuse and neglect, and adult safeguarding in general. The chapter will also include a discussion of how the health and wellbeing of staff might be promoted better to meet the needs of people with dementia and carers.
Chapter 10 : Care homes in integrated care
There have been various fashions and fads in thinking about ‘integrated care’, and part of the problem has been the plethora of different perspectives and models. This chapter will adopt a practical perspective of people living with dementia and carers having their health and wellbeing attended to in the right place, right way and the right time, and consider various aspects concerning this. Consequently, the discussion will emphasise advance care planning, attending hospital, admission and re-admission, avoiding hospitals, care transitions, case management, the “future hospitals” initiative from the Royal Colleges of Physicians, improving patient flow, intermediate care and discharge, liaison psychiatry and CMHTs, specialist clinical nurses including Admiral nurses, and “virtual wards”.
Chapter 11 : Independence
This chapter will consider some important diverse areas which intend to promote independence, their progress and impact in overall policy. These include electronic medical and care records, “individual service funds”, and reablement. This chapter will also consider potential opportunities and risks from personal genomics and personalised medicine.
Chapter 12 : Palliative care and end of life care
It is beyond dispute that palliative care and end of life care are essential components of promoting health and wellbeing in people living with dementia and carers. Person-centred care, maximising continuity of care, is fundamental. This chapter will consider the special features of this approach which are very important, and also consider why there has been a reluctance amongst some to consider dementia as a terminal illness. The chapter will also consider the significance of grief, and also consider a possible notion of ‘pre-grief’.
Chapter 13 : Living at home
The first twelve chapters are very relevant to the final chapter on living at home. Whilst much of the media attention is on care homes and nursing homes, or residential settings in general, there is remarkably little focus on living at home, including living at home alone, despite enormous interest in this amongst the general population. This chapter will consider how this approach may have evolved from the philosophy of ‘successful aging in place’, and consider how specific home environments might be enhanced including extra care environments. This chapter will include discussion of, specifically, community nursing including Buurtzorg Nederland, day and respite care, self management. telehealth and technology, and smart homes. The pivotal role of social care and social work will be emphasised throughout.
In her annual message today, the Queen said: “It is true that the world had to confront moments of darkness this year, but the Gospel of John contains a verse of great hope, often read at Christmas carol services, ‘The light shines in the darkness, and the darkness has not overcome it.’”
She continued: “It’s no surprise that such a human story still captures our imagination and continues to inspire all of us who are Christians, the world over.
“Despite being displaced and persecuted throughout his short life, Christ’s unchanging message was not one of revenge or violence but simply that we should love one another,” she said.
Thanks to the combined efforts of millions around the world, many people who have been given a diagnosis of dementia are not excluded by communities and societies.
I never cease to be amazed by the many initiatives in this country and around the world where people living with dementia find inclusive and accessible services. The language is also changing slowly, where words which were once commonly used, which are pejorative and offence, are not as frequent as before.
But there’s still more to be done. There are still ‘frequent offenders’ when it comes to language.
The light shines in the darkness, and the darkness has not overcome it.
At all times, understanding dementia is not about policies, processes or strategies. It is not about targets or the number of people recruited.
Dementia is fundamentally a human story.
It is a story of someone who may need help in noisy environments wishing to follow the thread of a conversation. Or it could be something totally different, like text being made a bit bigger on a blog.
No one size fits all.
There are about 47 million people in the world living with a diagnosis.
I have no doubt one day there will be successful treatments for some, but not all of the dementias. I anticipate the first to benefit from these new drugs will be some of the people living with young onset dementia.
This hope is important.
More important than fear.
We should not be terrified into action about helping people who are fellow citizens after all through manipulative message conveying a sense of shock.
We need to understand the needs of people with dementia, met and unmet, however diverse they are, and those needs of their significant others.
We need to make sure that everyone knows their obligations under the law, including obeying human rights and, in some cases of employers, employment law.
People living with dementia are entitled to the best possible healthcare, wherever they are.
Residential settings should not be viewed as fortresses, divorced from the rest of society, but where people can have a reasonable expectation of living in a homely place.
This is about care for today as well as for tomorrow; but we should not hold any negative feelings for those who can only see the world through a pharmacological and industrial lens.
This fundamental perspective, whatever your religious standpoint, is one which should resonate with us all.
I actually hate ’round robins’, so the idea of me “bigging up” my achievements is much of an anethema to me as it is to you. If I were a clinical regulator organisation, I’d want to be celebrating the very best, as well as identifying the very worst. I am unlikely to give myself a ‘very good’ rating, unless I am nominating myself for a HSJ award. In terms of my own development, I think I progressed substantially from my first book ‘Living well with dementia: the importance of the person and the environment’ to the second book ‘Living better with dementia: good practice and innovation’.
The reasons for this progression were two-fold, I think. Firstly, Chris Roberts most politely offered me feedback about the limitations of the phrase ‘Living well with dementia’. In a nutshell, the major problem is if somebody has a bad day the phrase unfairly blames him or her – in effect the phrase sets people up to fail. A better phrase ‘living better’ is aspirational, and relative. Secondly, I changed in style from one of technocracy, in meeting the demands of the NICE quality standard 30 ‘Supporting people to live well with dementia’ in England to a “more human”, as Steve Hilton might put it, discussion of some important issues in world policy.
My work no longer felt like work, and more like something enjoyable I would do learning from things which had happened in my life. A big thing which happened in my life was going to Australia. I always said to Chris, Jayne and Kate that this would end up ‘being a trip of a lifetime’, which was our justification to ourselves that we wouldn’t ‘slum it up’. Quite the opposite happened. I had a truly magical time. When I got over the daily anxieties of wondering where my passport, wallet, keys and phone were, I loved being in the company of some truly remarkable people. I almost daily read Kate Swaffer’s blog and Beth Britton’s blog. I read the DAI’s blog weekly if I can.
I should really avoid a list, for fear of missing people out, but these must include Kate Swaffer, Peter Watt, Boris the Cat, Veda Meneghetti, Lynda Henderson, Mick Carmody, Sue Carmody, Ian Gladstone, and Jacinta Lynch. But they also include people I came to know also through the Alzheimer’s Disease International conference, held this year in Perth, Western Australia, including Gayle Harris, Truthful Kindness, and Denise Craig. Definitely one of the most surreal ‘episodes’ in #ADI2015 was when the indefatigable Suzy Webster appeared by video link in one of sessions. It’s true – Chris had not seen Suzy on the plane either! My own talk there was on risk and genetic discrimination.
Later in the year, Kate Swaffer and I went down to see Charmaine Hardy and family down in Robertsbridge. I saw Charmaine where in London for the PPA Support Group, brilliantly run by UCL. As you’ll be aware, I think the world of Kate. We became fans of Tony and the Ostrich pub in Robertsbridge, as Charmaine had warned us!
I got to know as very close friends some people at events throughout the year, especially Agnes Houston, Donna Houston, Helga Rohra, Wendy Mitchell, Beth Britton, James Murray-White, Fenella Lemonsky, Jens Rohra, Prof Peter Mittler, Gary Mitchell, Joanne Agnelli, Ken Howard, Toby Williamson, Jennifer Bute, and Colin McDonnell. And also people who fleetingly appeared, but were a big part of my daily Twitter lives, cumulatively made a big impact, including Jeremy Hughes, Larry Gardiner, Alison Cameron, Jos Bell, Karen Dening, Rachel Thompson, Prof Alison Leary, Mehrdad Seyf, Steve Milton, Tommy Dunne, Ripajeet Kaur, Joyce Dunne, ‘Diverse Alz’, Ceri Sian Hodgkinson, Rachel Mortimer, Sarah West, Fran O’Hara, Katy Judd, Pam Luckock, Rebecca Myers, Carmen Medina, Lee Spokes, Hilda Hayo, Hilary Evans, Simone Willig, Hilary Doxford, Silke Kammer, Gráinne McGettrick, Rachel Niblock, Ruth Eley, Louise Langham, Anna Gaughan, Jean Tottie, Marc Wortman, Barbara Stephens, Reinhard Guss, Geoff Huggins, Prof. Olivier Piquet, Lorna Anna Hart, Al Power, Joy Watson, Tony Watson, Philly Hare, Andy Tyson, Zoe Harris, Rachel Menzies, Irene Oldfather, Sarah Reed, Helen Sanderson, Suzi Henson-Amphlett, Richard Humphries, David Oliver, Lucy Frost, Jim Pearson, George Mcnamara, Amy Dalrymple, Gavin Terry, Amy Pepper, Daniella Greenwood, Caroline Millichamp, Debbie Sorkin, Graham Browne, Gary Marsh, Sara Marsh, Andrea Sutcliffe, Nicky Taylor, Prof Dawn Brooker, Prof Murna Downs, Prof Alistair Burns, Prof Martin Prince, Des Kelly, Glenn Rees, Prof Bob Woods, George Rook, Olwen Williams, Caroline Sutcliffe, Joyce Cavaye, Nada Savich, Elo Novilunio, and, of course, Tommy Whitelaw. And Nicole Batsch on a DAI webinar!
Thanks to Jo Moriarty, whose modesty and sheer knowledge are unmatched.
@ermintrude2’s blog is a MUST read for me now, which cuts through all the bullshit in policy ( pardon ).
And I immensely value the thousands of people who know what dementia’s about from Twitter, and who know what life’s about, including Truffle the Cat (whom I have never met ever.) I try to keep up to date with blogs which interest me, like Pippa Kelly’s excellent blog. It was also nice to chat with Lyn Romeo, which I found generally most useful in realising the pivotal work done in the social care profession. I met for the second time ever Peter Ashley at a round table on human rights and dementia, being run by Toby Williamson at the Mental Health Foundation. Peter was a great man, and may he rest in peace. I have been massively moved by Kate Swaffer’s missing of Richard Taylor PhD who also passed away this year. Kate was visibly moved by the video sent by Richard for our private get-together of friends and colleagues on July 11th 2015 in the Arlington Centre, Camden.
Kate gave a talk on the 11th which was brilliant. I gave one too.
Chris’ introduction meant a lot to me personally. I find Chris a rock of support.
Also missed to me is Tim Lloyd-Yeates, whom I spoke to on the phone several times after his diagnosis. It was, however, great to celebrate Tim at the Dementia Congress in Telford.
I turned up to the ‘supporters day’ of Alzheimer Research UK in Euston Road round the corner of where I live, and thought the talks and workshops explaining the work the charity does were brilliant. Hilary clearly is hugely respected there, and so ‘gets’ it. I gave a talk on book 2 at the Alzheimer’s Show in London Olympia, which was another lovely get-together of lovely people too. I was on a panel at the King’s Fund, talking about the future directions of our English dementia strategy, which I loved (and I later attended the ‘enhancing health in care homes’ day there which I learnt a lot from). I attended the Alzheimer’s Society Annual Conference, which I loved, especially the talks by Dennis Gillings and Sir David Dalton.
I ‘made’ about a hundred ‘Dementia Friends’ this year through my talks at BPP Law School, which I’m proud about – a hundred more people who know a bit more about dementia. In fact, I went to an event for Dementia Friends Champions, at their HQ in Devon House, which I enjoyed enormously. DevoManc (with the work of ‘Dementia United’) turned out to be quite a big part of my year indirectly. As a complete aside, I did a few information leaflets on diverse issues for the Manchester academic unit. I loved Alzheimer Europe’s conference held this year in Ljubljana, where I gave a talk on the critical importance of clinical specialist nurses in dementia.
I will in the new year have a paper in Nursing Times on wider issues involved in Nursing Times with Karen Dening, who is Director of Admiral Nursing at Dementia UK. Education matters a lot to me.
I was honoured to accept an invitation to speak on the importance of social media and research at the Open University in Camden, even if it did have an unintended adverse effect of me disliking the research assessment exercise of professional academics. As the year progressed, research and advocacy became more enmeshed with one another for me. I became very interested in human rights and disability activism, and, completely as a result of Prof Peter Mittler, became interested in the United Nations Convention on the Rights of People with Disabilities. I think it’s fair to say that Peter keeps on the ‘right track’ as an academic mentor, for which I am hugely grateful.
In terms of education, I gave four one-hour evening lectures at BPP Law School on aspects of English dementia policy including dementia friendly communities, integrated care, care, cure and research, and choice and control.
This is the one Kate attended (as we were lucky enough to have Kate visiting England in the summer of 2015):
I hope to be organising an MSc online course in dementia for BPP in the new year. BPP is where of course I did some of my postgraduate degrees in law and business. It was, however, with unexpected pleasure I had a great time doing 20 slides with 20 seconds per slide ‘Peucha Kucha in Newnham College on risk and dementia, despite my mixed experience of Cambridge, my original alma mater.
Senses became very significant to me in three ways – firstly, Kate’s emphasis on them in her cuisine, Agnes’ work on raising impairment about sensory issues in dementia, and, finally, the talk I gave on the importance of music as part of Lucy Frost’s “Alive” season in a church in Brighton.
You see, I don’t ‘do’ dementia as a job, as a source of income, apart from very modest royalties from my books. I very rarely claim expenses. I overall attend events all at my own expense. But I enjoy what I do, and that counts for a lot. Chris Roberts did however emphasise that what I do for a living, writing and researching, is equal to a proper job, and advised that I should not belittle its value at all. I don’t have any conflicts of interest, which means I can speak my mind, as you can tell. It was, an honour, to have my work appreciated by peers in that I won best book in the category of ‘health and social care’ for the BMJ Book Awards.
I am now working on my third book, this one to be published by Jessica Kingsley Publishers, entitled ‘Enhancing health and wellbeing in people with dementia: care homes and care at home’, which is in effect on ‘integrated care’, but actually on promoting health and wellbeing persons with dementia in the right place, right time and right way. That of course is the ultimate goal of the NHS and social care, and ‘dementia friendly communities’. I intend to write most of it in one of the libraries of the Royal College of Physicians in London, where I became a member this year. I had intended book 3 to be my last, but I wish to do an important 4th one with Gary Mitchell in 2016 part 2 (a surprise.)
(Apologies to anyone I’ve missed out completely unintentionally.)
Thanks also to the membership of Dementia Alliance International, whose blog and ‘Meetings of the Minds’ sessions I’ve found interesting thus year.
Above all, please do remember that anything can happen to anyone at any time.
In my ‘yuletide blog’, I argue briefly that we’re in a good place as regards the English dementia policy.
What I don’t want to happen is ‘throw the baby out with the bathwater’. Patients have a pivotal rôle to play in service provision improvement and in research. They are not merely ‘data harvesters’.
Likewise, the good intention behind risk factors and prevention shouldn’t be drowned out by an aggressive push to private insurance systems. The National Health Service, paid for general taxation, involves us sharing risk in an equitable way.
This means that we’re not ultimately punished by being borne with higher risk for certain conditions, such as some of the dementias which run in the family. Likewise, identifying dementia at an earlier stage might help to identify more realistic and effective pharmacological treatments, with more research.
In a way, we are currently in the optimal position, so long as certain stakeholders don’t overplay their hand.
The progress in the English dementia policy jars inconveniently with the funding crisis and poor performance of some (not all) parts of the National Health Service.
The main issue is that the whole system is not working. For a start, it is not always possible to get people with dementia into hospital in a timely way as it is impossible to discharge ‘fit for discharge’ patients into the community due to the destruction of social care.
Earlier this year, we were also greeted by this cheerful headline:
And we know that social care has been on its knees for some time.
Richard Humphries, hugely respected at the King’s Fund, gave this unequivocal appraisal in December 2015 concerning the smoke and mirrors of the social care settlement, clouded by talk of the ‘precept':
“Instead of a fundamental root and branch review of how entitlements, as well as funding, are aligned across the NHS and social care, as proposed by the Barker commission, the government has chosen an opaque and messy hotchpotch of measures, which fails to address the short term pressures on social care; it does nothing to place funding on a more sustainable footing in the longer term.”
Dementia policy is currently running in two parallel universes. One universe is the poor state public health and social care find themselves in. The other is the multi-million pound ‘transformation fund’ for drugs for dementia, which may even be too expensive for the NHS to offer in a comprehensive way.
So what’s new in dementia that the Prime Minister can possibly get his teeth into?
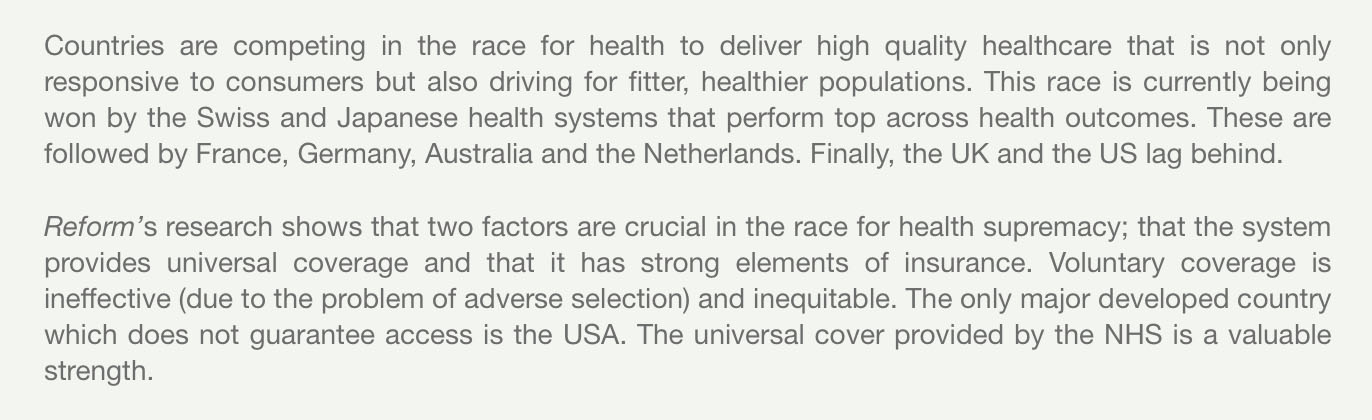
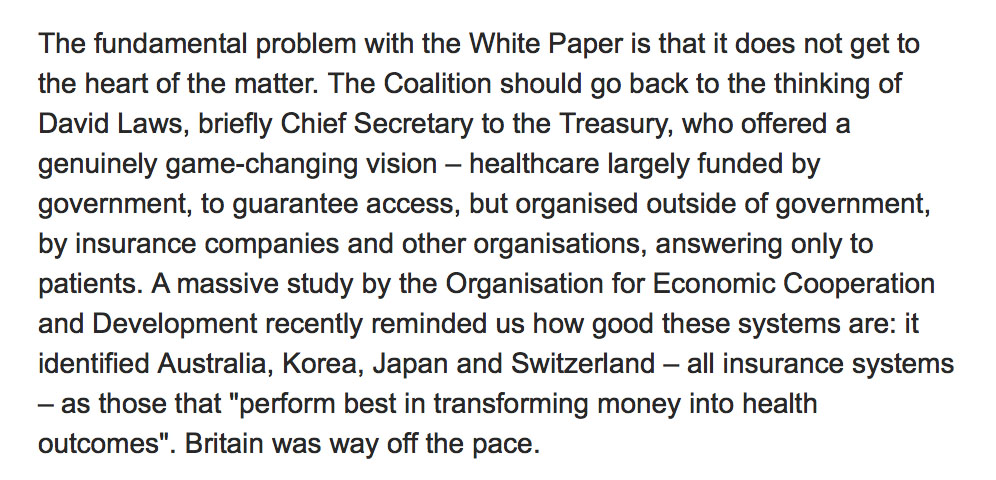
Nick Seddon used to be the Deputy Director of ‘Reform’.
He wrote in the Telegraph back in 2010, just as the intense political debate over the much criticised Health and Social Care Bill erupted, the following:
And the solution, unsurprisingly, is framed in terms of a hybrid insurance model.
Lord Warner was the only Labour Peer to vote in favour of the Health and Social Care Act (2012).
And, of course, there was the ideological legacy from the New Labour era, exacerbated a million times worse in the Health and Social Care Act (2012) due to the introduction of default competitive tendering under s.75, of competition as a tool to improve quality. There is very limited evidence to support this, whereas there is quite substantial evidence to show that competition in health markets worsens health equity, and is very costly.
In the Guardian in 2014, a description was given of his new Jerusalem on the NHS based on co-payments and an emphasis on prevention.
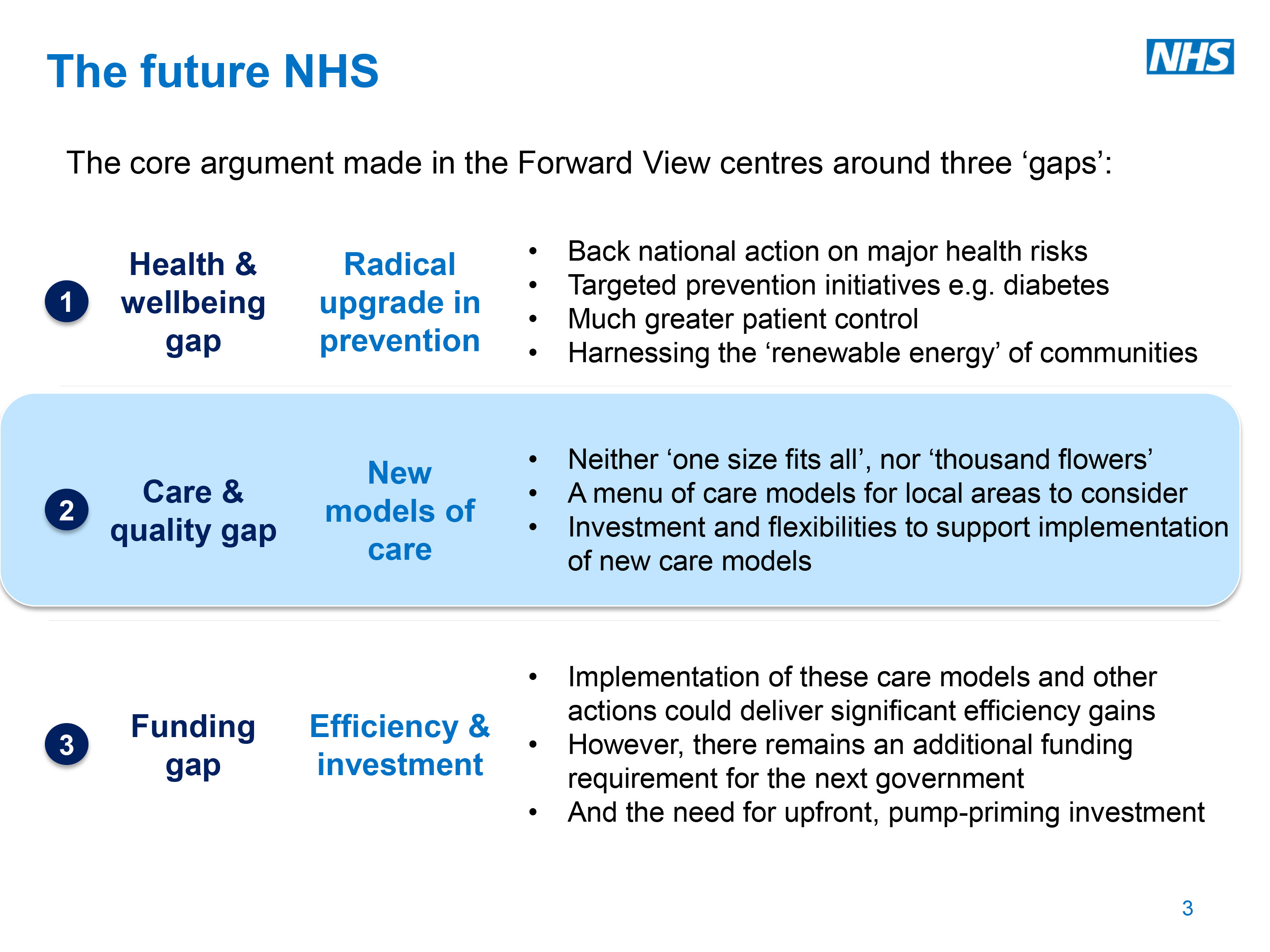
So fast forward to the current framework of the NHS underlying the ‘vanguards’ and the ‘new models of care’.
This all cosily fits in the structure of the ‘three gaps’ of the ‘Five Year Forward View’ from Simon Stevens, whose new Labour background is well known. In 1997 he was appointed policy adviser to two Secretaries of State for Health (Frank Dobson and Alan Milburn) and from 2001 to 2004 was health policy adviser to Tony Blair. He was closely associated with the development of the NHS Plan 2000.
Closing the ‘prevention gap’ is still “big business”. There has been an increasingly tendency to pedal the ‘we’re all patients now’ meme with the Big Charity creations of ‘pre-dementia’ and ‘pre-diabetes’, for example. Reasonable clinicians are of course running a mile from this. And – guess what – prevention of dementia means big money.
There is one huge reason why the mechanism of us pooling risk together through general taxation is the best way to look towards the future of dementia care. The alternative, through private insurance, would be an unmitigated catastrophe. But this is an ideological war against the National Health Service, and various devices such as the insidious introduction of the personalised budget through the Care Act (2014) have seen this subtle rationing of resources to the individual level, under the deceptive marketing of the word ‘choice’.
It is no accident that Simon Stevens is a huge fan of genomic medicine. With the possibility of your entire genome being scanned, for risk factors for dementia, you could be aware of your risk for dementia and be inclined then to take out private insurance. But the research into genetics in dementia is advancing quite rightly, as it is hoped that efficacious interventions for a suitable subset of genetic +ve persons might exist in the future.
But Alison Cameron has described very elegantly, recently in “Healthcare Manager” magazine, how the patient movement views itself as more than data points as a bit part for others’ agendas.
This creation of new private markets is the ultimate nirvana of those propose privatisation.
But it is a hugely slippery slope.
You could find out you’re at high risk of dementia and decide you’ve got nothing to lose, as the insurance company will pay out, and blow your lifestyle on all the unhealthy risk factors. Or if you’re at low risk you could decide that paying into the NHS is not for you, and opt out for a relatively cheaper private insurance system.
In 2008, in the US the Genetic Information Nondiscrimination Act (“GINA”) was passed into US law, prohibiting discrimination in the workplace and by health insurance issuers. One wonders whether a genetic phenotype should be considered one day for an amendment in the Equality Act for overseeing such claims under discrimination law.
GINA prohibits issuers of health insurance from discrimination on the basis of the genetic information of enrollees. Specifically, health insurance issuers may not use genetic information to make eligibility, coverage, underwriting or premium-setting decisions.
What has genetic discrimination in the US looked like?
“Jacob, a boy who carries a gene for a disorder called Long QT Syndrome (LQTS), was denied coverage under his father’s health insurance policy because of his pre-existing condition. LQTS is a rare and little-known genetic disorder that sometimes triggers sudden cardiac death. Those who carry the gene may be healthy until they suffer an attack without warning, but carriers can control their risk of cardiac arrest with preventive beta-blocker therapy. Jacob’s father wanted Jacob to be insured, but even after their state enacted a law prohibiting genetic discrimination, Jacob’s insurance company still refused to cover him.”
This year, there were about three reports which were published co-temporaneously on the theme of ‘women and dementia’. And yet there was surprisingly little focus on women, who are living ‘beyond a diagnosis of dementia’ (Kate Swaffer’s articulation), in leadership rôles.
In one way, I think this overall reflects the bias against people with dementia in leadership rôles. The obsession from medicine, nursing and allied health professionals has been predominantly in leadership in their professions.
There is also in parallel an area of patients who are assuming leadership rôles, although the term ‘patient leader’ can lead to unintended assumptions from some, like that that person is presenting himself or herself as a representative.
I think also the classification and taxonomy of subtypes of leaders has generally been unhelpful. I don’t think it’s possible to read too much into the identity type of leadership in a particular person. The range of options, for example heroic, charismatic, situational, transformative, solo, toxic, is a testament to that.
I also worry about people who nominate themselves as ‘leaders’, in the same way that the identity of ‘entrepreneur’ or ‘innovator’ is often bastardised.
I have little trust in the judgement of others in identifying ‘leaders’, howeverso defined. Whenever leadership and award ceremonies come together, it is not beyond reasonable doubt that the right winners are picked.
Are these winners supposed to be “rôle models”? Take for example the recent example of Katrina Percy who has seen both high points (such as in the HSJ and Guardian) and low points (such as countless newspaper articles and the recent Mazars report).
Bizarre
and even more bizarre
But you cannot extrapolate about women and leadership from one example, as countless counterfactuals exist. One person’s Margaret Thatcher is another person’s Barbara Castle. One person’s Shirley Williams is another person’s Clare Gerada.
The ‘second generation gender bias’, I felt, was particularly interesting.
“Many entrenched organizational structures and work practices were designed to fit men’s lives and situations at a time when women made up only a very small portion of the workforce. … A vicious cycle ensues: Men appear to be best suited to leadership roles, and this perception propels more of them to seek and attain such positions, thus reinforcing the notion that they are simply better leaders.”
And the current articulation of ‘the gender issue’ is perceived as inadequate, as per this article also from the Harvard Business Review website:
“The time has come to reframe the gender issue. In many companies and countries where I work, from Iran or Brazil to Russia, managers tell me that they recruit a majority of young women as they clearly outperform their male peers.”
I first encountered Susan Suchan, living with dementia, from the close group within the Dementia Alliance International. Her blogpost there is sensational.
Great – BUT what is the chance of Susan being given a paid rôle in a large charity as a leader?
One of the main theories about why women do not become leaders is that they do not find themselves onto the right training programmes or with the right informal networks.
But Susan is a leader.
Look at this video.
The Supreme Court were once asked to give an opinion on the definition of “pornography”. They failed to make a suitable definition but did comment ‘you recognise it when you see it’.
Kate Swaffer is clearly an international leader also living with dementia. Her seminal book ‘What the hell happened to my brain?” will be published next year. In addition to ‘power’ as Chair of Dementia Alliance International, she currently has enormous influence in world dementia policy too.
You recognise leadership when you see it. Helga Rohra has advocated away from the excessive medicalisation of dementia as a powerful advocate as Chair of the European Working Group of Persons with Dementia and latterly Vice Chair of Dementia Alliance International. Helga was pivotal in changing the narrative away from ‘the stages of dementia’ to the ‘faces of dementia’ – this was completely supported by the underlying medicine, as progression in dementia can be variable and unpredictable. Helga once asked what the offering of the current global dementia policy would be to the 47 million people living with dementia at one of the G7 events, and no good answer strikingly was forthcoming.
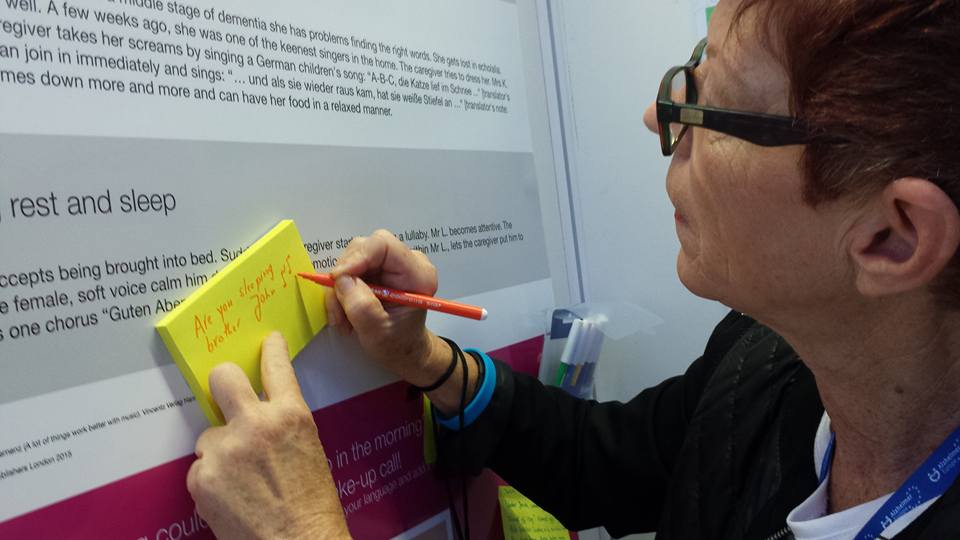
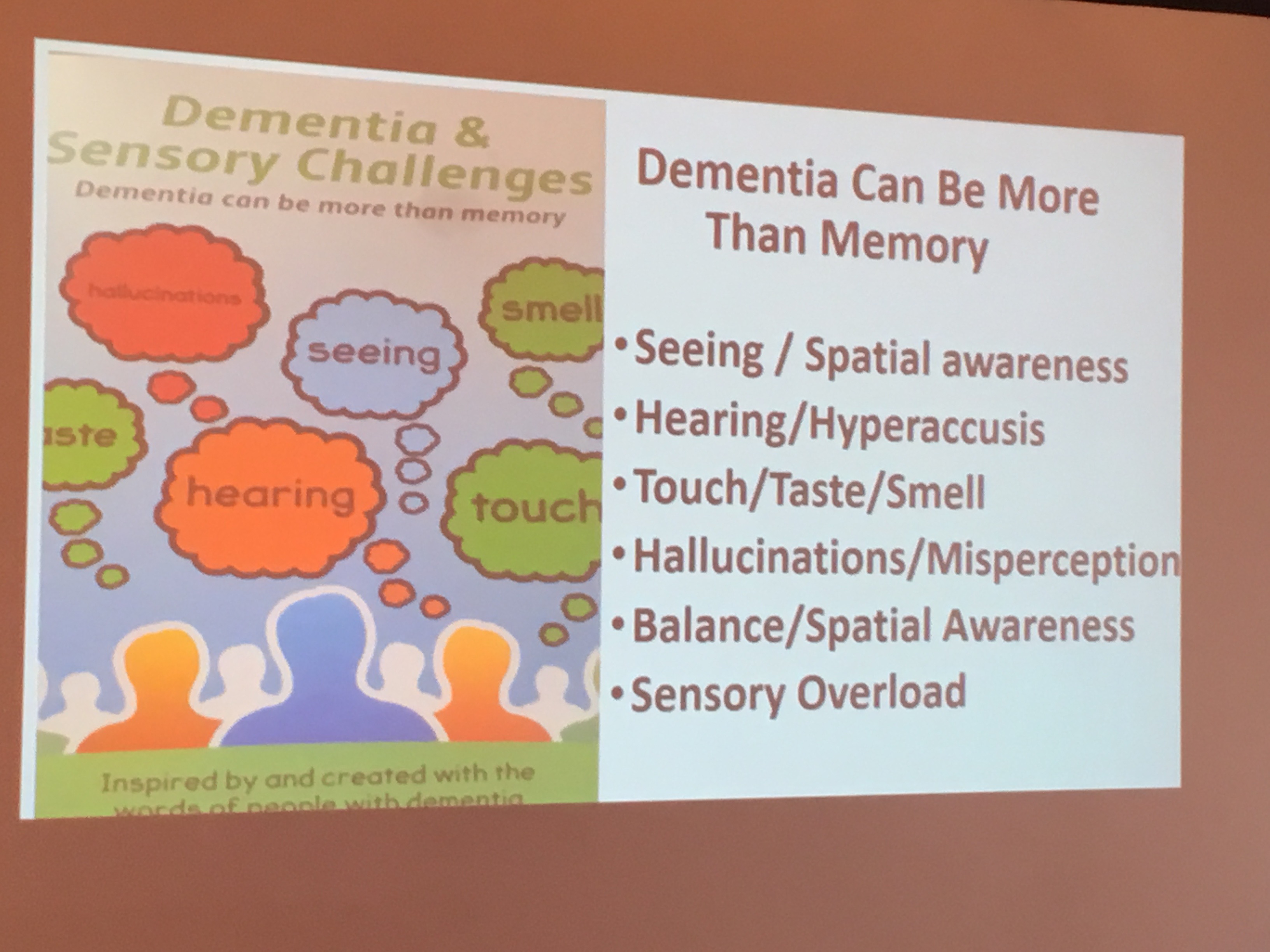
And Agnes is a leader too. She received her MBE today from Buckingham Palace. Agnes from her home base in Lanarkshire with her daughter Donna (whom Agnes calls a ‘rock of support’) has been campaigning very successfully on raising awareness of sensory features of living with dementia.
Agnes does this work for the benefit of other people living with dementia, but also others who desperately need the education. That’s “doing the right thing”, “not necessarily doing the easiest thing”. We don’t need tonnes of infograms and hashtags to realise the value Agnes’ work has brought thus far. Agnes is not ‘owned’ by any organisation, but Agnes is a huge team player as well as a leader.
So here’s a thought – what about a report this time not just on “women and dementia”, ‘engaging women’, but one on “women with dementia as leaders”? That sort of thing might actually change the narrative, from observational and identification, actually to producing a transformative change.
For example, Wendy Mitchell, living with dementia, at the Department of Health is exactly the type of change we need. See her excellent blogpost here.