I must admit that I always feel like throwing something at my computer screen when I see a steering group for people with dementia run by people without dementia but with big financial grants.
For some reason, I used to conceptualise the way some people had approached ‘dementia friendly communities’ like a zoo. Event organisers serially wheeled out a star ‘person with dementia’ like a spectacle, akin to the ‘push me pull you’ of Rex Harrison.
The boot is on the other foot now.
It’s like this.
The thing is communities which are ‘dementia friendly’ should in fact be suitable for all. This means inclusive to all. This means accessible to all.
A major problem with the term ‘dementia friendly’ is that it implies that you can identify immediately person with dementia by the way he or she is behaving in the community. No person with dementia has a sticky adhesive label on his or his forehead saying ‘I have dementia’.
Dementia is an invisible disability. It’s a disability where we can identify the exact problem, say problems with hearing in a noisy room, or problems with memory, or problems reading. Like all disabilities, it requires a sensible approach such as identifying if the problem causes an impairment and subsequent handicap.
I’ve seen this referred to as ‘cognitive ramps’ – but any level of analogy might be suitable such as ‘cognitive wheelchairs’. The basic point is that you’d expect employers to build wheelchair ramps (or simple) for young employees with a physical disability to allow them to get into the building to do their work in the first place; such an attitude is needed for people with young onset dementia too (this is dementia below the age of 65).
The other big way in which the term ‘dementia friendly communities’ is wrong is that it implies a very static process, which ironically is not how the UK accreditation scheme works at all. The UK standards (really specifications) necessitate sustainability, i.e. that the community will be friendly in the future, and is always ‘learning to be friendly’.
This gets to the heart of a tension which exists in policy. That you often hear from many diverse people with dementia that they’re living for the present, and yet there’s one dimension of policy that aspires for a better world for tomorrow – whether this is in the form of dementia friendly communities, or better treatments for the future (disease modifiers or symptomatic treatments).
The policy which crystallises the imperative for the world to build ‘dementia friendly communities’ for the future actually comes under the WHO sustainable development goals. They’re pictured here.
It’s clear that people living with dementia need access to the UN Convention on Rights of People with Disabilities (UNCRPD), as all the preamble and articles of that convention apply directly to people with dementia.
Both these instruments are very closely linked to the implementation of a rights-based approach for dementia. Human rights lie at the core of this phase of supporting people with dementia to live in the community after their diagnosis. Even if the UK takes the step of repealing its existing human rights legislation, implementing the European Convention on Human Rights, the global policy tools remain.
The question is of course how people with dementia can best advocate for them. The safest way to make this manageable is to make sure human rights remains in the international conversation, as demonstrated, for example, by Marc Wortmann in the PAHO Plan of Action summit in Washington.
But we do also need local leads which integrate dementia and disability policy drivers together. This, for example, might be facilitated by organisations such as Alzheimer’s Europe participating in the work of the European Disability Forum to make sure that the achievable ‘UN sustainable goals’ and UNCRPD are indeed implemented as ratified. Yesterday, the EPSCO Council adopting the Luxembourg EU Presidency conclusions most helpfully took Europe down the route of rights-based advocacy, as faithfully reported by Alzheimer Europe.
But I feel that we shouldn’t lose sight of the main issue: people with dementia are no longer in the audience. They’re the main actors.
It’s claimed that the British trade union movement, in response to yet another battering of the left-of-centre political parties at the general election in 2015, produced the clarion call, ‘Don’t mourn, but organise!’ The saying, originally associated with the last words of a singer and activist called Joe Hill it is reported, has become synonymous with a severe defeat.
The diagnosis of dementia, imparted to a person and his or her friends and family, can be perceived as a severe defeat. With a relative lack of pure biomedical offerings for symptomatic treatment or cure, currently, or indeed drugs to halt progression of the disease, persons on receiving a diagnosis can be expected to commence an endure a prolonged period of a type of ‘mourning’. The expectation of packing up your day job or dissolution of friends of family can be overwhelming, if an alternative of reablement through the social model of disability is not even ‘on offer’. It is estimated that there are currently about 47 million people in the world living with dementia.
I often give ‘Dementia Friends‘ sessions to the general public. Such information sessions can lead you to bring into sharp focus your own thinking indeed. I was asked about the ‘diagnosis gap’ recently by a salaried GP from West London: this is the gap between potential diagnoses of dementia in the community, and the actual number of diagnoses given. This shortfall has had a number of reasons associated with it across the years, and English policy has tried to reduce this gap.
Chris Roberts was told his diagnosis of mixed dementia, Alzheimer’s disease and vascular dementia, a few years ago. His dementia is what is called a ‘young onset dementia’, as it presented before the age of 65. However, Chris had a history of emphysema, a disease of the lung which can produce shortness of breath and marked decrease in oxygen saturations. Such low oxygen (hypoxia) can indeed cause memory problems. Chris underwent a series of systematic tests before finally arriving at a diagnosis. That is why you always hear Chris about preparing to wait for a proper and correct diagnosis in a ‘worth the wait’ manner.
Chris is passionate about educating others about dementia. He is in fact the Alzheimer’s Society regional ambassador for Wales, a contact for the Alzheimer’s Research UK, a ‘champion’ for Join Dementia Research, a delegate for Dementia Action Alliance, passionate about supporting Young Dementia UK, a Dementia Friends champion, amongst his main commitments. Such experience has been very recently recognised in his deserved appointment to the committee appointed by NICE (the National Institute for Clinical Excellence).
The basis for the doctor-patient relationship is based on trust and confidence. And yet the statistics surrounding how a diagnosis sometimes not being imparted are staggering. The whole ‘mix’ of reasons is complicated, including a reluctance by some not wanting to be given the diagnosis of dementia, but 37% of people with dementia in the UK do not receive a formal diagnosis, and the length of time you have to wait to receive a diagnosis varies hugely depending on where you live, from two weeks to over six months. For some time now, the Alzheimer’s Society has been doing its ‘Right to Know’ campaign.
In English policy, there have been correct concerns that accompanying the drive for diagnosis should be an equal sustained improvement in post-diagnostic care and support for a person with dementia. This might include a care coordinator, information sharing between care services, multi-disciplinary input as or when required (e.g. from a physiotherapist, speech or language therapist, occupational therapist, clinical psychologist, specialist nurse), enhanced healthcare across a diverse range of care settings (including at home, residential care homes, hospitals and hospices), better advanced care records and planning, better end of life care, and so on. Clinical nursing specialists have in particular a pivotal role in helping with coping strategies for carers, who very often find themselves under strain whilst doing valuable and rewarding work. And an optimal system must include dementia advisors and dementia support workers too.
Chris himself spoke briefly about this topic last year at the Alzheimer’s BRACE conference in Bristol.
Chris produced a brief ‘wish list’, which started with ‘joined up services’.
Here in a recent Care England/ITN debate, Beth Britton, well known campaigner and advocate in dementia care, says, “In my own experience, for my dad, integration simply did not exist.”
The cuts in social care funding over the last few years have been devastating. Such cuts have had an impact on the delivery of NHS care, for example in delayed discharges from hospital, but it is clear that the social care profession need proper resources and time to care in itself.
The Alzheimer’s Society is currently looking at standards in post diagnostic care and support for dementia, and this will be an extremely welcome contribution to the narrative here in England. A substantial contribution has been made previously by the Care Quality Commission in their ‘Cracks in the pathway’ document, which, while celebrating outstanding care, did concede simultaneously that bad care did exist and could not be accepted. Often care faltered at discontinuities in the care system, notably.
Life experiences matter enormously, as through building up a picture of how people have lived beyond their diagnoses of dementia in the community is critical for us all to understand dementia. Wendy Mitchell never fails to amaze me in the sheer commitment she puts into her campaigning, which includes describing her experience of early onset Alzheimer’s disease, including through her blog ‘Which me am I today?‘. Alzheimer’s disease is the most common type of dementia worldwide, typically presenting with significant problems in learning, memory, navigation and/or attention. Wendy is passionate about promoting dementia research particularly. Wendy will indeed be discussing with Gavin Terry in policy from the Alzheimer’s Society the need for an effective post-diagnostic network next week in ‘NHS Expo’.
There is no doubt that huge strides have been made in ‘engagement’ and ’empowerment’ of people with dementia. I do not wish to underestimate this. But I do find the word ‘engagement’ as a term a bit limp; for example, I do not as such ‘engage’ as postman when I receive my post from and chat with him daily. You can’t “half believe” in equality or inclusivity, I feel. It has to be more than perceiving people living with dementia as ‘living with an illness’ in the strict medical model, and getting away from the ‘does he take sugar?’ mentality which can inadvertently rear its ugly head. I feel the next obvious advancement is to advance empowerment to a further level, and to have those people who want to, living with dementia, also leading on policy. Chris’ appointment to NICE and Hilary’s appointment to the World Dementia Council, while conceding that a few representatives for the millions with dementia are inadequate, have been the necessary first step in this process, I feel.
There are ways of not mourning but organising, through for example the European Persons with Dementia (chaired by Helga Rohra), or internationally through the Dementia Alliance International (chaired by Kate Swaffer). Therefore, if one truly believes in genuine equality, we should be jumping at the chance of equipping those people with dementia who want to with the leadership skills to promote authentic advocacy. This will meet with some resistance from others, I am sure, but this is essential if we are to go beyond ‘friendliness’ and cut into the icebergs that are stigma and discrimination.
This could be the video from any corporate. The point is that the video contains very familiar concepts and memes which can be marketed very easily.
I have reviewed the development of the policy of ‘dementia friendly communities’ in the penultimate chapter of my book ‘Living well with dementia’.
The description of “dementia friendly communities” given by the Alzheimer’s Society is provided as follows:
“The dementia friendly communities programme focuses on improving the inclusion and quality of life of people with dementia… In these communities: people will be aware of and understand more about dementia; people with dementia and their carers will be encouraged to seek help and support; and people with dementia will feel included in their community, be more independent and have more choice and control over their lives.”
This definition doesn’t make sense to me as it ignores networks – networks (including social networks such as Facebook and Twitter) are particularly important to those whose physical or mental health might pose formidable barriers to being physically in any one place in a community.
But when you ask “what is a dementia friendly community?” inevitably the question becomes re-articulated “what constitutes a community, and what counts as it being ‘friendly’ to ‘dementia’?”
And immediately you see the problems. How large is a community? Or put another way what constitutes the boundaries of the community? In theory, a community could be members of a part of the Lake District, or the Square Mile. Being ‘friendly’ demands the question ‘how long is a piece of string’? Without some clarity, this construct is ‘motherhood and apple pie’ and a perfect tick-box vehicle for commissioners to demonstrate that they’ve done something about “dementia friendliness”.
And which dementia? There are about a hundred different causes of dementia, the most common one being globally Alzheimer’s disease, characterised typically in the early stages with real problems with learning and encoding new memories (and subsequent retrieval).
So it’s conceptually possible to talk about dementia-friendly communities where you put up signage everywhere so people with Alzheimer’s Disease, who have spatial navigation difficulties, can get a bit of help.
But not all memory problems are dementia, and not all dementias present with memory problems.
But what those people with frontal dementia who have perfect memory, but who present with a slow change in behaviour and personality according to their closest ones?
How should we make communities ‘friendly’ to them?
The policy construct immediately experiences an obstacle in that it talks about ‘dementia’ as one great mass, an error previously made for ‘the disabled’. But this criticism is of course by no means fatal – as conventional communities also contain a huge range of people of all different characteristics, anyway. But is then the concept too broad as to be meaningful, such as “male friendly communities”?
Something which Kate Swaffer, an Australian who has significant experience in campaigning for advocacy for people with dementia, and who herself lives with dementia, recently shared on Twitter was this eye-catching caption.
And you see the difficulty? How do we design a ‘community’ which is ‘friendly’ to ‘dementia’, if you believe like me that once you’ve met one person with dementia, you’ve met one person with dementia?
It’s clearly impossible to legislate for someone to be ‘friendly’ to another person in a society, however loosely defined, but it is worth at least acknowledging the existant law.
But you can easily argue that the policy fosters a spirit of solidarity far beyond rigid compliance with the law. Such solidarity of course seems somewhat at odds with the backlash against any form of state planning from this government and previous governments.
I’ve thought long and hard about the need to try not to dismiss worthy initiatives in dementia policy. For example, whilst I am concerned about the error rates of ‘false diagnosis’ of people with dementia, I would be equally concerned if NHS England did nothing to try to identify who the undiagnosed with dementia currently are.
Likewise, my natural instinct is to think about whether the charity sector is distorted with initiatives such as ‘Dementia Friends’. According to the Government’s website, by 2015, 1 million people will become Dementia Friends. The £2.4 million programme is funded by the Social Fund and the Department of Health. The scheme has been launched in England, and the Alzheimer’s Society is hoping to extend it to the rest of the UK soon. Linking the global policy of dementia friendliness to one charity, when other similar initiatives currently exist (such as the Purple Angels, Joseph Rowntree Foundation, University of Stirling, WHO, and RSA), means that many dementia charities may get unfairly ‘squeezed’.
I do, however, intuitively and desperately wish this policy to succeed. For example, at my stall yesterday at the SDCRN 4th Annual Conference (the Scottish Dementia Clinical Research Network), a person called Hugh actually bothered coming up to me to tell me how much being a ‘Dementia Friend’ meant to him. He talked about friends of his who were ‘Dementia Champions’. He spoke with tremendous affection about his late wife had lived with dementia for eight years, and the importance of community work to him.
And it is very difficult to deny that initiatives such are this are truly wonderful.
A real concern, though, is that by conceding one is building a ‘dementia friendly community’, even with all the best will in the world, the term itself doesn’t for me suggest or promote real inclusivity. It still sadly implies a ‘them against us’. I think I have this attitude because I’m physically disabled, and I would balk at the term ‘disabled friendly community’. It’s incredibly important that this policy is not London-driven friendly communities with more than a twang of tokenism.
I am therefore leaning towards a viewpoint expressed by Simon Denegri, Chair of INVOLVE, and NIHR National Director for Public Participation and Engagement in Research:
@SDenegri “i’m not sure I know what dementia friendly communities are. I’m not sure I even like the term” #SDCRN
And surely you’d want businesses and corporates to be ‘dementia friendly’? But which corporates, and why dementia? Surely you’d want them to be friendly with rare muscle wasting diseases, or cancer, for example? Shouldn’t carers get their own “carers friendly communities”?
This poses big problems for our perception of inclusive communities.
Alastair shared a lovely picture which sums up the problem for me.
You can easily see why certain corporates such as banks might wish to help out with this policy, because people with dementia can be at risk of financial abuse, but is this a genuine drive to help people with dementia or is it a pitch to secure competitive advantage like ‘ethical banking’.
Apart from isolated stories such as of dedicated no-hurry lanes in supermarkets, for example, surely one would have expected supermarkets to have pulled out all the stops with adequate signage everywhere? Many large supermarkets have about thirty lanes where it’s easy for the best of us to get lost. I don’t think I’ve ever been to a dementia-friendly supermarket where the signage would be of a good enough quality to prevent a person with mild Alzheimer’s Disease becoming spatially disoriented.
“Dementia friendly communities” lend themselves easily to ‘diversity marketing’, however. Diversity marketing is a marketing paradigm which sees marketing (and especially marketing communications) as essentially an effort in communication with diverse publics. As an acknowledgement of the importance of diversity marketing is that AT&T Inc. has a post for this discipline at vice president level. It is reported that, starting in the 1980s, Fortune 500 companies, government agencies, universities and non-profits organisations began to increase marketing efforts around diversity, according to Penn State University.
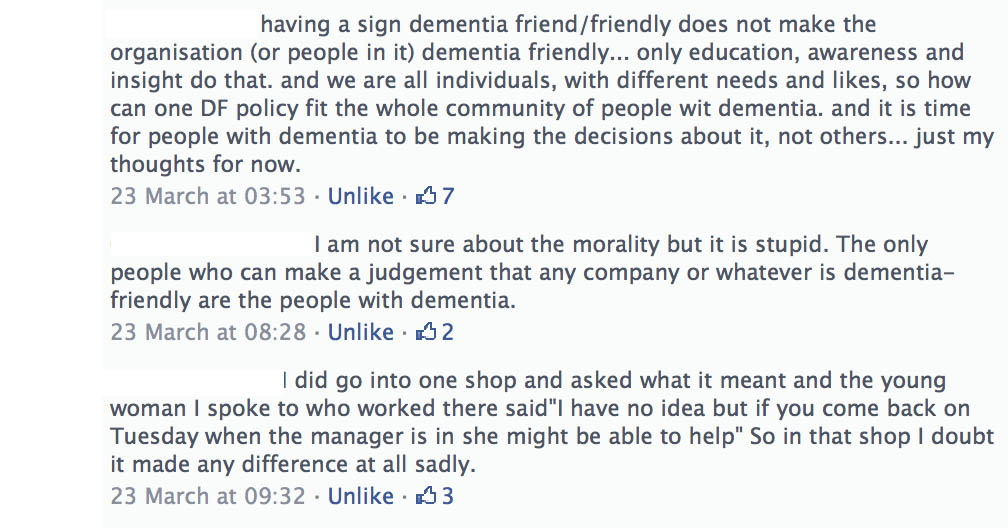
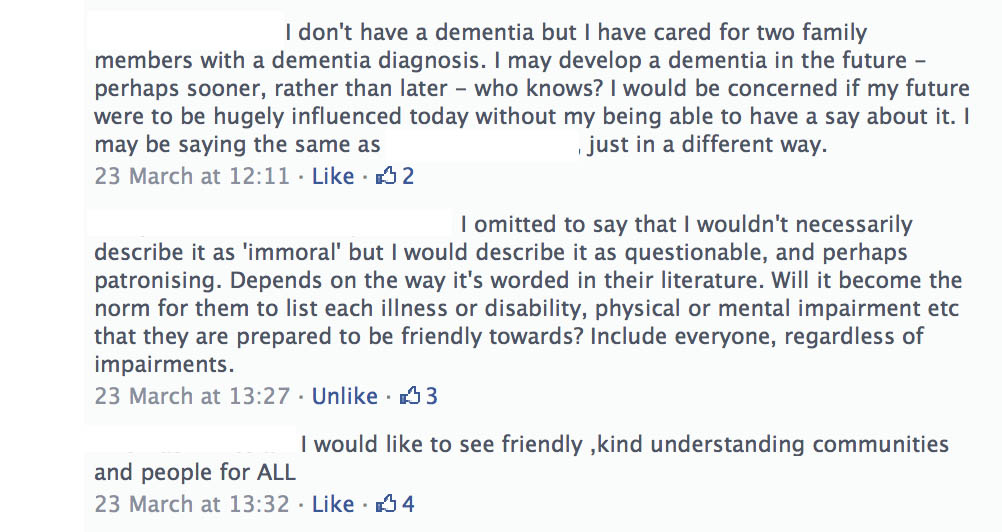
I asked my friends on Facebook whether there was anything particular ‘immoral’ about this diversity marketing in relation to dementia friendly communities, and their responses were as follows.
In other words, there is no ‘right answer’.
It’s clear to me that this policy, as it is currently being delivered, needs much greater scrutiny in terms of where the benefits have been, and for whom.
Strangely enough, with the focus of drugs, drugs, and yet more drugs, there’s been relatively scant attention for the environment in which a person living with dementia finds himself or herself in.
Improving wellbeing for a person is essentially about understanding the past and present of that person, and building on that person’s beliefs, concerns and expectations about the future. But the idea that you can ignore the environment is simply science-fiction.
The design of care homes maters. The design of hospital wards matter. The design of towns including pavings and signs matters.
Such an approach sounds ambitious and joined up, but not impossible. There’s been a long and proud history in England of understanding the social determinants of health, including housing.
The Attlee Government also extended the powers of local authorities to requisition houses and parts of houses, and made the acquisition of land less difficult than before. In 1949, local authorities were empowered to provide people suffering from poor health with public housing at subsidised rents. That very same year, unemployment, sickness and maternity benefits were exempted from tax.
Recent research suggests that wellbeing in later life is closely related to the physical environment, which is an important mediator of ageing experiences and opportunities. The physical character of the built environments or neighbourhood in particular seems to have a significant impact on the mobility, independence and quality of life of older people living in the local community.
According to a “Greenspace Scotland” report from 2008, “Trust for Nature” is a community-based conservation organisation that focuses on the protection of private land of high conservation value in the state of Victoria, Australia.
In recent research by Inclusive Design for Getting Outdoors (ID’GO), 15% of questionnaire respondents (a large sample, nearing 1000 in sample size) had stumbled or fallen outside within the last 12 months. The real figure is likely to be higher, since past-year falls are often under-reported. Many of the environmental risk factors associated with outdoor falls appear to be preventable through better design and maintenance; factors including pavement quality, dilapidation and kerb height.
Abstract experiential qualities such as perceptions of ‘safety’ and ‘attractiveness’ have been identified as important factors in stated preferences for parks and green spaces and there has been much written over many years on landscape aesthetics and how this might influence preference and use.
By contrast with research on environment and health, arguably this is a domain rich in theoretical concepts for the mechanisms behind engagement with the environment but poor in terms of tools to measure the detailed spatial and structural qualities of different landscapes in relation to how people actually use and experience them. For landscape designers, this is of crucial interest. There have been, historically, attempts to develop guidance based on general principles, but few tools actually to measure the dynamic spatial experience in practice.
A built environment for all ages is conceptualised as one that has been designed so that people can access and enjoy it over the course of their lifetime, regardless of ability or circumstance. Such environments are said to be designed “inclusively”. The I’DGO (Inclusive Design for Getting Outdoors) consortium was launched in 2004 to investigate how outdoor environments affect older people’s wellbeing and to identify what aspects of design help or hinder older people in using the outdoors. Their focus is on identifying the most effective ways of shaping outdoor environments inclusively. They support the needs and preferences of older people and disabled people, always seeking to improve their independence and overall quality of life.
I’DGO was set up to explore the ways in which being able to get out into one’s local neighbourhood impacts on older people’s wellbeing and what barriers there are to achieving this, day-to-day. The project asked the crucial question: why do we need a built environment for all ages? The first phase of research, which finished in 2006, involved over 770 people aged 65 or above. Participants were asked about their wellbeing and quality of life, how often and why they went outdoors and what features of their local neighbourhood helped or hindered their activity. Researchers also physically audited 200 residential neighbourhoods to look for barriers and benefits to getting around as a pedestrian.
The I’DGO research found quickly that older people went outdoors very frequently to socialise, exercise, get fresh air and experience nature. If they lived in a supportive environment – one that made it easy and enjoyable for them to get outdoors – they were more likely to be physically active, healthy and satisfied with life. Walking was by far the most common way that people spent their time outdoors, whether for recreation or transport (‘getting from A to B’). Participants in the I’DGO study who lived within 10 minutes’walk of an open space were twice as likely to achieve the recommended levels of healthy walking (2.5 hours/week) as those whose nearest open space was not local.
A major research goal has been to examine the specific attribute of neighbourhood streets – tactile paving at steps and crossings – and asks how this affects the biomechanics of walking and risk of falling in older people (the project run by the SURFACE Inclusive Design Research Centre and their colleagues in Health, Sport and Rehabilitation Sciences at the University of Salford). The benefits of tactile paving for blind and visually impaired people have been well established yet the system is not without its issues.
Tactile paving is not a policy area without its concerns, and a few in particular emerge from a report by the UK Health and Safety Executive. This report suggested that there is a need better to understand the extent and implications of incorrectly designed and laid tactile paving, and the toe clearance of an individual in negotiating paving ‘blisters’ and potential slip hazards. These factors appear to be crucial to older people, since many of the first phase ID’GO interviewees expressed concerns about falling or feeling unstable on tactile surfaces and fall-related injuries are associated with loss of independence, morbidity and death in older people.
If we are to understand what qualities of the environment are important to an ability of individuals to ‘live well’, we need perhaps to acknowledge the diversity that exists in people’s capabilities, experience, desires and needs. This overall is a huge challenge for designers; the response conventionally has been to look for factors in the environment that matter to most people, or to a defined group of people, and to address those factors as if they were equally important. Yet for any individual, different qualities and elements in the environment may be a matter of indifference (e.g. certain colours if you are visually impaired) or vitally important (e.g. proximity of an accessible toilet if you have a weak bladder).
Such an approach builds on the concept of “affordance” and the reciprocal relationship between perceiver and environment. The concept of affordance links environment and human behaviour, or opportunities for action, and is therefore of particular interest in understanding how the environment might encourage or support people to be more active—a primary goal of public health policy. This is an insight of key relevance to investigating human behaviour in the landscape. As Appleton has put it, more succinctly, for any individual considering their landscape context, it helps us understand “what’s in it for me?” (Appleton, 1975).
Key text
Appleton, J. (1975) The experience of landscape, New York, NY: John Wiley.