Many thanks to Fenella Lemonsky (@organiclemon) for this helpful review of my book in “Mental Health Today) [here is the link to the original article.]
I find reviews like this a useful steer on future work. Academics can be notorious in misjudging the ‘mood music’ of the main drivers behind the service: people who use the services, which in my case are people living with dementia, their friends and family and other carers. I am in a privileged position in having access to thousands of peer-reviewed papers, but also feel that I have learnt a lot about the dementias from people living after a diagnosis. My knowledge of dementia has vastly improved since I took myself away from the medical lens, and adopted a viewpoint of other professionals and practitioners and people living with disability.
Shibley Rahman, 2014, CRC Press, ISBN 978-1908911971, £29.99
There has been much written and spoken about dementia in the media recently as a result of the government’s Dementia Strategy, which aims to help those with dementia, their families, professionals and carers be more responsive to needs.
In this context, Living Better with Dementia, by Dr Shibley Rahman, a dementia expert who is qualified in medicine, neuroscience and law, is highly relevant.
Initially, Rahman talks about the stigma of dementia and how this has remained through the past century, despite dementia becoming better understood and having a more positive outlook in recent years. While dementia and the whole management perspective can appear a challenge as the older population survives longer, this book is encouraging and positive. Specific medication that delays the onset of dementia symptoms and other medication like antipsychotics are discussed at length, including their use in nursing and care homes and how specific practices that have no evidence base can be challenged.
Two chapters that for me stuck out as very important were on young onset dementia and on antipsychotics and innovation. Young onset dementia was first explained to me at the author’s book launch, where nurse lecturer Kate Swaffer from Australia, who has young onset dementia, gave a moving talk. The impact is huge for the individual, their family and peer network as well as professionals. It affects employment, career opportunities and has a huge stigma attached to it as it is still often misunderstood. This is all discussed in the book.
The use of antipsychotics and care homes is also discussed at length. This is an important chapter, especially for those who look after those going into residential care, and it can enable them be on alert to good practice and how to spot where medication is used inappropriately. Antipsychotics use in care homes is a complex issue. In many cases careful use can ease distress and agitation, but there seems to be concerning evidence that there is over-prescribing of antipsychotics where behavioural treatments are more appropriate. Using extensive research, Rahman explains why using antipsychotics needs careful thought.
Other chapters focus on deprivation of liberty, sporting memories, global view and leadership strategies.
This is a well-written, extensively researched, easy to read and important book for anyone interested or working with dementia.
Rating: Highly recommended.
Review by Fenella Lemonsky, mental health service user researcher
First of all, I should not actually ‘love dementia research’ if only because I’ve been doing it discontinuously since my finals in neuroscience at Cambridge in 1995-6. Familiary breeds contempt, and all that.
I think meeting three people in the last year really turbo-boosted my interest in research into dementia. And I think if you compare the contents and style of my two books in dementia, published last year and this year, I feel the second book, as Steve Hilton might put it, is ‘more human’.
The three people are Wendy Mitchell, Chris Roberts and Hilary Doxford – of all these three, I know Chris by far the best, but I find the eagerness of all three to promote dementia research awesome.
Chris Roberts, living with a mixed vascular and Alzheimer’s dementia (not uncommon a combo), managed to do two interviews on the BBC last week, “Victoria Live” and “BBC World”, managing to get a plug in for ‘Join Dementia Research’.
‘Join Dementia Research’ (@beatdementia) is an initiative anyone can join in to take part in dementia research. It’s sort of like a different sort of dating agency – one where you paired up to the research project most suitable to you. You don’t have to be living with dementia to participate.
When I tweeted this picture earlier today, I did not actually realise Chris Roberts and Jayne Goodrick were standing on the far right (where they are not politically.) Hilary’s on the far left (not politically either, to my knowledge) and Wendy’s in the eye-catching red jacket (not a political statement either, I think.)
Chris here explains his own experience of dementia, and explains the need for research in his BBC World interview. Any person with dementia becomes an expert in his or her own condition in time and place.
But having thought about it a lot recently, in light of national policy, I’ve concluded that I like research into dementia a lot. I enjoy reading about it all the successes and failures. I like doing my work, even though it does not consume any expensive resources. I’ve so far got a chance to present my findings, which have not cost anything at all, at two international conferences: Alzheimer’s Europe and Alzheimer’s Disease International.
I think I would strongly recommend anyone living with dementia or closest to such a person to think about even doing research for himself or herself, and publishing the research. Once you get involved with the research bug, it’s a great way to meet people, and talk effortlessly with people who share your interests. I’m invariably impressed by medics who’ve had the time, opportunity or resources to pursue research of some sort, not least because they’re furthering the knowledge and reputation of the profession. It also tells me that “they’re not one trick ponies”.
I don’t think of a primary goal of a researcher should be gainful paid employment. The people I’ve found who excel at research are the ones who are genuinely passionate about it. It’s a great privilege I feel to be able to study a topic in detail, and to take on contemporary challenges. As a person, I feel philosophically that nothing goes to waste, so for me even ‘negative findings’ have value.
Whilst I do not share in the hyperbole surrounding the drug trials research presented last week in Washington at the Alzheimer’s Association conference, I think any development which overall increases our understanding, however small or incremental, is to be welcomed. The advantage of well designed trials, even if they do not throw up the ‘clean results’ many would like to see, not least for a ‘return on investment’, is that they provide something people in the future can rely on. Money we spend on research is literally investing in hope. A love of knowledge I suspect would get a widespread democratic mandate, as would a greater understanding of human experience. All of this helps the NHS in our jurisdiction to offer a better care and support environment, with colleagues in social care, in theory and hopefully in practice.
I don’t feel it’s a just but lost cause, like any good Jacobite would, although I’ve been in love with lost causes since I became a supporter of Tottenham Hotspur, or a book called ‘Jude the Obscure’ (St Jude was apparently the Patron Saint of Lost Causes).
Possibly even there’s no such thing as satisfaction. In “The Dawn”, the 19th century philosopher Friedrich Nietzsche claimed that that which is erroneously called ‘pity’ is not selfless but actually self-motivated. Am I motivated by negative emotions such as ‘pride and satisfaction’ in doing research into dementia? Am I ‘taking control of biology’? Possibly.
I published my paper in 1999 with Prof John Hodges and various others for a reason. This was because they were patients turning up in cognitive neurology clinic, query the behavioural variant of frontemporal dementia, whose tests appeared at first blush entirely normal. And yet these tended to be people in their 50s or 60s with quite profound changes in personality which had been noticed by their closest. I provided an explanation for why this paradox exists in this paper which is now cited in the current Oxford Textbook of Medicine. I argued it’s because the part of the brain which is affected, a part of the brain near the front of the head towards the eye, is hard to investigate.
The vast majority of my colleagues in research have confirmed this finding, which brings me onto my final point. It is incredibly rewarding when someone you’ve never met before claims to agree with you and have taken your results further. And it’s wonderful when somebody you’ve never met before knows your research and likes it – this happened to me when I met Prof Brendan Boeve from the Mayo at the Alzheimers Association conference last year in Copenhagen.
We’ve had circular discussions on ‘suffering’ before, to the point we probably agree to disagree, but have learnt to respect other people’s well meant perspectives. But I think it’s fair to say that the happiness and camaraderie which accompanied #ADI2015 is a very real one. I took this photo at a chocolate factory in Adelaide Hills. Nutrition and dementia, as it happens, was a key satellite theme of the #ADI2015.
Here’s a film by Arc Seven Communications of Beth Britton explaining the need to consider what people with dementia can do.
As it happened precisely on the day of our return, as I was travelling from Kuala Lumpur to Amsterdam, Australia aired a brilliant programme ‘Insight’ on living with dementia.
It had been a huge pleasure to have returned from spending time with Kate Swaffer, Peter Watt and Colin McDonnell who all featured in this remarkable programme. In place of fear, I felt a substantial integrity was provided by having so many delegates living with dementia attend this year’s Alzheimer’s Disease International (ADI, @AlzDisInt) conference. We met up in Perth, Western Australia, in the middle of April, for three wonderful days.
@legalaware@DementiaAllianc absolutely and it was epic to have 10% PWD in attendance! Hope that trend continues. — Dementia Advocate (@jball49) May 1, 2015
My talk was on whether dementia care would easily lend itself to private markets. I received a lot of useful feedback from delegates. I basically pointed out the problems of trying to put dementia care under the philosophy of insurance contracts because of the potential asymmetry in information between insurer and person/patient. This information asymmetry, I argued, could come from, say, a complete genetic screen, if NHS England get their way in moving towards personalised medicine/Big Pharma. The problems arise if someone with a high genetic risk for dementia seeks insurance knowing he or she is at high or low risk; or whether a person obtains an insurance policy and then behaves in a high risk behaviour. I argued that it was likely that there would need to be legislation in the English jurisdiction to protect against genetic discrimination, as in the United States.
However, I think I had most fun in the ‘poster session’, for me on Friday afternoon. I had the unexpected pleasure of chatting with Karen Harrison Dening at my session, over the need for a network of national clinical nursing specialists. As it happens, Karen has just published a brilliant book on culture and dementia, which I strongly recommend.
Thanks hugely to Chris and Colin McDonnell (@ColinMcDonnell) in helping me enormously during the poster session, which I do find stressful every time (particularly when you have curled up posters so vehemently they have no chance of sticking onto the board!)
This was for me the most interesting poster of the whole conference – on challenging behaviours, by Kate.
This blogpost explains its rationale in part. Even putting aside the general consensus that the dementias are under diagnosed in many jurisdictions, there’s a feeling that the recent scrutiny in dementia policy has overall helped.
Every 4 seconds someone in the world develops dementia. It’s vital we provide support, both now and in the future pic.twitter.com/qOURmB6IZg — ADI (@AlzDisInt) April 30, 2015
I was particularly impressed by the research presented by Prof Martin Prince on behalf of his group at King’s College London. I think Prof Prince has a clear understanding of the critical assumptions of his work, as you would expect him to have. I had a long chat with him after his lecture. He struck me as a very sincere, thoughtful man, who was open to wider repercussions of his work. In particular, we shared a common interest in seeking accurate estimates for the global prevalence of younger onset dementia.
The beginning of the conference (@ADIConference), I felt, was very surreal but pretty magical. I don’t particularly like the word ‘indigineous’ as I feel Aborigines as it can further division and divide, and I feel that Aborigines have experienced a very bad deal culturally from others exerting racial and cultural imperialism.
Here, I feel some of us must show some solidarity.
I personally bought a didgeridoo which I gifted to my mother on return (although I am mindful of the physiological limitations of the use of didgeridoo as a musical instrument by females). I was surprised to hear that didgeridoos (sic) are not permitted in hand luggage, however.
The conference itself was incredibly well organised. You can still access the book of abstracts for the conference here and wider information about the programme. I helped to review abstracts for the conference; I was indeed on the international advisory board for the conference, so reviewed abstracts for dementia friendly communities and younger onset dementia.
I am at the end of policy involved with living better with dementia, which includes advocacy across jurisdictions. I found an intense sense of hope and confidence from the conference, as opposed to the shock doctrine of Pharma which can be striking elsewhere in global policy on dementia.
The “vanguards” of dementia advocacy, globally, one may argue, are Kate Swaffer from Australia and Helga Rohra from Germany.
So it came to pass that we were all hugely proud when Kate Swaffer, Co-Chair of the Dementia Alliance International, a group consisting of people living with dementia, came to give her plenary.
I understand that videos of talks given by members of the Dementia Alliance International will be uploaded onto their website in due course.
Here’s for example Helga Rohra, Chair of the European Persons with Dementia, giving her plenary. I was deeply honoured to be name-checked in her talk. Helga is a friend, and someone whom I deeply respect.
(video from the DAI You Tube channel)
One of the plenary speakers was Al Power (@alpower12), Allen Power. Basically, I thought Al is terrific. I have now read his book “Dementia beyond disease”, which I feel is a groundbreaking reframing of the narrative towards treating people living with dementia as individuals with dignity, and how they should not be the target of pejorative language or assault through inappropriate medication.
I have known of Mick Carmody for ages. Mick has been instrumental in ‘rallying the troops’. I anticipate that his enthusiasm and focus will lead to greater things in global advocacy.
But I fell in love with Mick and his wife Sue from the moment I met them. They’d come from Brisbane, Queensland, and were hugely thrilled about participating in an international conference on dementia. Mick lives with dementia in Australia, and, it’s fair to say, had not been given sufficient or appropriate encouragement, pursuant to diagnosis. What changed the game for him was finding the Dementia Alliance International.
I am a card carrying member of the club that individuals who’ve been given a diagnosis of dementia are all unique individuals with a huge amount of experiences, and it’s not what people cannot do, as with us all, but what people can do. Here are Helga Rohra and Chris Roberts, powerful Dementia Friends Champion ambassador for the United Kingdom, as described here in the popular Alzheimer’s Society magazine “Living with dementia”.
Helga is simply larger than life, and I found many things Helga shared with me profoundly interesting. Society has come a long way, but there’s still a long way to go. Helga, I suspect, speaks up for a vast army of people who’ve been given a diagnosis as part of a large social movement, expecting dignity, acknowledgement of human rights, expecting improved employment relations post diagnosis, and calling for holistic care.
The #ADI2015 was simply triumphant for the Dementia Alliance International. I think part of this confidence has come from the new strategic alliance with the Alzheimer’s Disease International organisation, which has supported DAI, but gone to great lengths to preserve the autonomy of DAI. This brand new arrangement is described in a recent ADI “Global perspective” newsletter. Credit must be given to Kate Swaffer (@KateSwaffer) and Marc Wortmann (@marcwort), CEO of ADI, who, I feel, have been instrumental in making this vaguely possible. Thanks especially to Marc Wortmann for his kind remark about my (minimal) contribution to the #ADI2015.
It’s dangerous to underestimate how Kate Swaffer has totally altered the terrain of attitudes towards dementia, in a positive way. Kate was diagnosed with the temporal variant of frontotemporal dementia, and the personal story is well described elsewhere.
I travelled around Australia after the conference too with Chris, and I hugely enjoyed meeting John Sandblom (@jball49), Treasurer of DAI. We all basically agree John is a top bloke!
Here’s a picture of Chris Roberts, Mick Carmody and Sue Carmody having a look at the posters presenting the latest research into the dementias at #ADI2015. That #ADI2015 was successful in disseminating research to people living with dementia, comprising 10% of the delegates of the conference, I feel is a huge achievement.
I found Daniella Greenwood entirely focused on what the needs of the people with dementia in the care sector are. In the Australian jurisdiction, persons are called “consumers”. Parking this difference in terminology, the plenary given by Daniella emphasised the critical importance of relationships, and I feel this is to be broadly welcomed, in her analysis of ‘consumer directed care‘.
Chris was often to be seen manning the DAI stall in between satellites and plenaries at the Conference. But the atmosphere there was “buzzing”.
We did enjoy each other’s company. I’ve known @TruthfulKindnes (@truthfulkindnes) for ages, living with a constellation of dementia symptomatology in the United States.
One of Tru’s list of achievements has been acting like a conduit for the creative expression of many people living with dementia. She specifically mentioned, for example, the experience of visual hallucinations. Visual hallucinations can be a predominant feature, for example, of the diffuse lewy Body type of dementia, an important cause of younger onset dementia, typically with a fluctuating way of symptoms appearing.
Having witnessed Tru’s desire to promote the work of people living with dementia, and her wish to use her gift in public speaking to inspire people, I know how important it was for Tru to make it from California to Australia to promote the experience of people living with dementia.
Tru has a true gift for speaking, with perfectly modulated speech and content.
Finding this hope to encourage others is deeply meaningful. Here, for example, is Simone Willig’s film (@SWHerborn) of Helga speaking about music therapy.
This year there were some truly outstanding satellite symposia. One that springs to my mind was the one on employment and dementia. I contributed there on the need for a greater understanding of disability law by employers in terms of unfair dismissal and discrimination, consistent with Kate Swaffer’s talk there, and I urged the need for cognitive diversity in the approach from employers, resources permitting.
Research was a key pervasive theme of the #ADI2015, which took as its title, ‘Cure, care and the lived experience’. There was a keen sense of learning from each other, across jurisdictions. Again, I thank Marc Wortmann for his lead in the workshop I attended where Chris Roberts gave a powerful overview of the lived experience.
Canada, I felt, offered an useful steer in this workshop on research.
It is a remarkable testament to the solidarity amongst people living with dementia and people close to them that there’s a huge interest in dementia research; but this is, as many us feel, not just about testing new drugs like guinea pigs but a genuine interest in research in care and living well with dementia. Otherwise, in policy terms, I feel that living better with dementia becomes the ‘squeezed middle’ between prevention and the optimistic search for the cure by 2025.
I was struck too by the inclusion of social media in this narrative.
When a diagnosis of dementia is disclosed to someone, quite sadly often in a substandard manner by professionals, there is a clear impact on friends and family. I found the contributions from Jayne Goodrick (@JayneGoodrick) and Kate Roberts, Chris’ daughter, sensational, in telling delegates actually what is happening in real life.
Tru devoted a substantial part of her talk in outlining the importance of the DAI, as well as her “swiss cheese” model of dementia.
Completely by accident, I happened to bump into Glenn Rees (@Glenn_Rees), now Chair of the ADI. Everyone who has been following world policy in dementia is aware of Glenn’s remarkable steer of Alzheimer’s Australia, where he has been instrumental in promoting consumer views; and this has had a profound impact internationally on a number of arms of policy, such as campaigning against physical restraint, and campaigning against the inappropriate use of antipsychotic medication.
Chris, I felt, was a true gentleman, and very engaging as a person. I loved travelling with him in Australia, and with Jayne and Kate. Many happy emotions are brought up in thinking of what we got up to; including Chris’ use of the phrase, “That’s the kind of guy I am!”
And it was incredible to meet for the first time ‘imaginary friends’, quite safe really, such as Jac (@JacintaLynch), here in Adelaide sitting with Chris.
I don’t drink alcohol. The reasons for this are well rehearsed.
But this did not stop me in any way loving the landscape of the environs of Adelaide Hills. Australia is of course well known for famous brand names in wine, and the Barossa Valley. It, ironically, took me a journey all the way to Australia to appreciate ‘black pudding’.
The proof of the pudding was indeed in the eating.
I learnt to trust the restaurant judgments of Kate Swaffer, a pretty mean chef herself (here’s her culinary blog).
I don’t think Kate has the time to write a cookbook on top of her massive list of other commitments – but.. her work can be felt in remote areas too.
And – seriously – I have never eaten such a perfect Thai curry ever (the lower dish): cooked by Kate.
On a completely different matter, I learnt very many things in Australia; not least that kangaroos have big scrotums (sic).
And that Chris can stand very close to emus, looking as if he’s in fact eyeing them up for dinner. One thing I certainly am thankful to Mick for is explaining how emus are bloody stupid creatures.
I didn’t know what to expect from Sydney after the conference. But it turned out to be amazing – I spent time with “guess who” (Kate) and new found close friends Lynda Henderson (@yodsupporter) and Veda Meneghetti (@Veda_Meneghetti).
I have many happy memories of my time in Sydney – here are Veda (left) and Lynda (right).
Veda is fast becoming a leading global ambassador for one of the lesser known of the temporal variants of frontotemporal dementia, the logopenic variant of progressive primary aphasia. She lives with it, and retains remarkable abilities from her life as a professional musician (aside: hence explaining the need for ‘life story’).
It’s yet again a case of what people can do.
Look at this – there’s no way I can sequence rhythms as well as this.
In fact, my supervisor from Cambridge, Prof John Hodges, who also shares a professorial position with Neuroscience Australia (@NeuraAustralia) happens to be one of the leading neurological authorities on this important condition.
I was really impressed with my visit to see Prof Olivier Piguet, a mutual friend and colleagues of colleagues of mine, Prof John Hodges and Prof Facundo Manes. NeuRA, an innovative research hub in Australia, is something truly advancing the frontiers of cognitive neurology.
Whilst I did not have time to go to the Sydney Opera House (I think Kate has seen the iconic ‘Carmen’ there)..
I did have a very long chat with Prof Olivier Piguet. Olivier and I have the same strong interests in social cognition, the somatic marker hypothesis and the functions of the ventromedial prefrontal cortex, anticipation of future events, episodic memory and eating behaviours; the common link being the behavioural variant of frontotemporal dementia. This is of course what I specialised in for my PhD at Cambridge.
It is nice to be involved with promoting research in dementia, if only at a global level and not in this jurisdiction (England).
I am not, however, convinced that a US baseball cap is the best way to do this for me?
I also discovered Olivier is much taller (and wittier!) than me!
Places like NeuRA do inspire me. They should inspire the rest of the global research community in cognitive neurology too.
And Veda, it turns out, was buzzing about the work of NeuRA.
Chris, it turned out, was amazing at throwing a spear as in Aboriginal culture. He did far better than the other visitors at Uluru, but of course it wasn’t a competition. When I delicately asked Chris how he came to be so proficient at throwing spears, he explained that he used to enjoy throwing javelin in school sports. So again it’s about what you can do – and I can’t throw a spear with my chronic double vision!
Chris, a leading advocate for living with mixed vascular and Alzheimer’s disease, was pretty good at boomerangs too.
The landscape around Yulara Drive (and Uluru) was simply gorgeous. This per se of course is nothing to do with #ADI2015, but conveyed the flavour of hope and happiness that was present at #ADI2015.
Chris, Jayne, Kate and I watched Ayers Rock change colour. Jayne in fact recorded a remarkable time lapse video of this.
Chris taught me how to take photos of people; consisting of 2 eyes and 1 ear.
Ayers Rock gave us plenty of time to think about the beauty of Australia.
But we had to ease our way back to the real world in a thud, albeit via a 4.5* hotel in Sydney near the international airport.
Currently, there is quite a lot of convergence in mutual research interests. Here for example is output from Alzheimer’s Australia taking as a spotlight prevention and social determinants of health (discussed in my new book).
This was my old book ‘Living well with dementia‘ (from 2014), which I didn’t “flog” at #ADI2015 (though many were well aware of it, which humbled me.) The large poppy on the front is courtesy of, and photographed by, Charmaine Hardy (@charbhardy).
I got Kate, Helga and Al to sign a copy of my book published last year – in a completely narcissistic way (I do apologise.)
I myself met ‘virtual friends’, such as @JoanneAgnelli whose work on language and dementia is widely respected.
My new book (“Living better with dementia”) is significantly more discursive than the last one, and should be published around 21 July 2015. Thanks very much to Jessica Kingsley for publishing it. It contains a chapter on whole person (integrated) care, which is due to reach a prominence, hopefully, after the UK’s general election on May 7th 2015.
The ‘stub’ will give you a flavour of the topics I will cover.
“What do national dementia strategies, constantly evolving policy and ongoing funding difficulties mean for people living well with dementia? Adopting a broad and inclusive approach, Shibley Rahman presents a thorough critical analysis of existing dementia policy, and tackles head-on current and controversial topics at the forefront of public and political debate, such as diagnosis in primary care, access to services for marginalised groups, stigma and discrimination, integrated care, personal health budgets, personalised medicine and the use of GPS tracking. Drawing on a wealth of diverse research, and including voices from all reaches of the globe, he identifies current policy challenges for living well with dementia, and highlights pockets of innovation and good practice to inform practical solutions for living better with dementia in the future. A unique and cohesive account of where dementia care practice and policy needs to head, and why, and how this can be achieved, this is crucial reading for dementia care professionals, service commissioners, public health officials and policy makers, as well as academics and students in these fields”
And I think #ADI2015 has paved the way for this book (and my final one which will be on living at home and residential care settings in more progressed living with dementias.)
We’re nearly there. Between 15th and 18th April 2015, Perth Australia will be the host for the 30th International Conference of Alzheimer’s Disease International.
If you ever an opportunity to listen to Tommy Whitelaw for an hour, do it. It’s really easy for people interested in English and global policy like to me to become obsessed with the usual macro policy details, but many people aren’t interested in macro. They want to know how the organisation of health and care systems will affect them individually.
We need to face facts. That is, there are about a million unpaid caregivers often members of a family, like a child or a spouse, in some form of care or support rôle. They do not see themselves as being labelled ‘carers’, but are fully aware of the rewarding and demanding aspects. Invariably they describe how they’ve never been given any formal preparation, just chucked in ‘at the deep end’.
It’s still pretty amazing that there are people who, despite being incredibly busy, find time to go on courses such as my friend Charmaine.
And here’s another crucial ‘issue’. I know nothing about what it is like to live with dementia, nor to care for someone with dementia. I am not a fan of the term ‘co-production’. There is, however, nothing more important than research and service provision being designed around the needs of the people who want the system to help.
I of course like the idea of ‘primary care support workers’, but I do like the idea of GPs being able to diagnose dementias more confidently (particularly differentiating the younger onset dementias, such as frontal dementia, from psychiatric syndromes such as anxiety or depression).
I like the idea of trained specialist nurses being able to get to know a person living with dementia more. I would like greater clarity of how professionals, people in a care or support rôle, and people living with dementia can work together, share knowledge and views, come to a plan while managing beliefs, concerns, expectations and conflicts. I would like this without the bubblewrap of selling “person centred care” and policy wonks, managers and politicians getting fixated with their measurement and gaming.
There will be a few highlights for me in the Alzheimer’s Disease International conference coming up. Not least is Al Power who I’ve got to know reasonably well in the last few weeks – and who seems to be one of the guys who ‘gets it’.
The programme is amazing, with lots for everyone to get their teeth into.
There are fewer things more humbling than to listen to Kate Swaffer or Helga Rohra. Of course, it is a tall ask to be able to be representative of any of the 47 million people living with dementia, but you get immediately a flavour of what these two view as important from them speaking. They want things better for other people living with dementia, and they are living in the here and now. They don’t deny making the world a better place for the future, but they want people with dementia to emerge from being hidden from view to being active people in society wherever possible.
Of course, the diagnosis of dementia itself is a big deal, and I personally feel, like Chris Roberts, living with mixed vascular and Alzheimer’s dementia in Rhuddlan Wales, and prominent Dementia Friends Champion, that more care has to be paid to preparing the ground for the diagnosis, the diagnosis itself, and what happens after the diagnosis.
And pay attention to Kate Swaffer, Co-Chair of the Dementia Alliance International, who politely queries how her investigations were done without clear explanation. I find this approach from the medics ‘underhand’, but Kate would be far too polite to say so, I reckon.
People with dementia have human rights, and it’s become accepted, sadly, for people including professionals to abuse those rights, e.g. physical restraint in residential homes.
Helga, Chair of the European Working Group for People With Dementia (with Alzheimer Europe), doesn’t refer to ‘stages’ of dementia, and I agree with Helga; ‘stages’ is a very medical term, and I have never known such clear linearity (people varying at symptoms in different presentations and rates). But whatever ‘faces’ of dementia, people with dementia and those closest to them have an inalienable right to dignity.
I’ve been honoured to have advance notice of what will be in Truthful Kindness’ presentation. That too will also be a smorsborg of creative astonishment on how one person from California has successfully inspired others around the world to live with symptoms of a dementia.
I do not deny the incredible work being done in dementia friendly communities and young onset dementia around the world. I know, because I reviewed a lot of the abstracts for the conference in these categories, being on the advisory committee for the conference.
But, above all, it’s a chance to meet up with people I like, and whose work I respect, like Simone Willig. There is a real sense of global solidarity I feel currently, including of course the traditional work being done in translationary neuroscience.
I will be looking forward to bumping into Marc Wortmann while dunking my biscuits, as usual; and I look forward immensely to meeting Glenn Rees, the incoming elected Chair elect of Alzheimer’s Disease International.
I reckon I’m all set – I’ve only got this far in organisation for this ‘trip of a lifetime’, thanks to Jayne Goodrick.
It’s our day at the King’s Fund, “Leading change in dementia diagnosis and support”.
The programme is here. If you feel that something is reported which is complete garbage, make sure you get a chance to give feedback using the hashtag #kfdementia.
I had dinner last night with Chris Roberts, Jayne Goodrick and Tommy Whitelaw in a pub in Euston. It’s well known I don’t drink alcohol any more, but I had a fantastic time!
Chris gave the ‘warm up’ talk – which was a talk I hadn’t heard before. As ever, I was intensely proud of Chris, and what he contributes to the community.
I have pledged to go through the thousands of letters with Tommy and bring them the key themes in a book. When people wrote their letters, they had no one to turn to. They would have been ‘processed’ by Government in the usual way.
This would not done justice to them. They’re not ‘complaint’ letters, but they contain information and experiences which are gold-dust. It’s likely that these wider messages will extrapolate to the care system across a number of jurisdictions. It’s likely an overall theme will emerge that people are not actually alone in their experiences, and just one small thing might have made a difference.
I told Tommy at the end of the evening that I had intended to make a polite comment at the end of his talk. But actually I actually wanted to comment on how outstanding it was. We all had joked about how it had ended up being mission impossible for me getting there taking a bus ride (I haven’t taken a bus for ten years), and climbing two flights of stairs. But, like L’Oreal, Tommy was “worth it”.
Like the NHS Change Day in England, it was absolutely great to see staff and other people involved in the NHS become truly feeling pride in what they want to see the NHS doing – which is of course great for me to see the NHS in a refreshing light.
Thanks especially to Dr Hilary Marmot, who is a person of significant sincerity, depth in knowledge and gravitas, in real life, with impeccable manners and kindness; Hilary had expressed to me in private how she had made a number of timetable “reconfigurations” to be there.
The talk has “mellowed me” out today. Instead of going to the King’s Fund in full wonk mode, expecting to spit policy bullets at people, I’ve decided to go there unscripted after all, listen and learn, and reflect on it all for my panel discussion this evening. I am looking forward to meeting many further friends and colleagues today, too many to name, but I will be especially looking out for Beth Britton, Tony Jameson Allen and Gary Rycroft.
And why not Chris and Jayne? Am seeing them in Oxford St before we begin!
A special thank you to Matthew Hopkins (@M_J_Hopkins) and his team for looking after us so well as his Trust yesterday. The pride in what you do really showed.
The biggest dementia conference to be taken place in Scotland (“Conference”, attended by 800 professionals, people with dementia and carers) was held in Glasgow last week (20-23 October 2014).
The focus of the conference was Dignity and autonomy in Dementia and the four day event explored in quite some detail how recognising the human rights of people with dementia, their carers, partners and families is key to ensuring dignity and respect, as well as overcoming stigma.
It was the 24th Annual Conference of Alzheimer Europe (@AlzheimerEurope, an umbrella organisation of 36 Alzheimer associations from 31 countries across Europe), supported this year by Alzheimer Scotland, .
The timetable was exacting.
The people there were very special; for example Tommy Whitelaw (@TommyNTour) mentioned in Alex Neil MSP’s speech at the conference. Tommy and Irene Oldfather (@IreneOldfather) happened to be passing through during one of my poster sessions.
Well done to the conference organisers for putting it together, especially Gladwys Guillory.
The main conference hall of the venue, the Crowne Plaza in Glasgow, the Argyll Suite, was majestic.
I particularly liked the ‘live Twitter feed’ at the front of the hall, where curiously Kate Swaffer (@KateSwaffer) appeared many times all the way from Australia. Here I am appearing with my ‘selfie’, with somebody well known in the foreground of the photograph.
The relative failure of the medical model in addressing the needs of people with dementia and caregivers was a pervasive theme throughout the whole conference.
I had a nice chat with Marc Wortmann (@marcwort) over one of the lunches. Marc is in charge of all aspects of ADI’s work (ADI = Alzheimer Disease (and associated conditions) International; @AlzDisInt). Collaborating with the Board, Marc implements finance and campaign strategies.
Cabinet Secretary for Health, Alex Neil, delivered a clear keynote speech to the conference at the Tuesday morning plenary session, in which he paid tribute to the immense contribution of Tommy Whitelaw.
Key to the event was the signing of the Glasgow Declaration: a commitment to promoting the rights, dignity and autonomy of people living with dementia across Europe, as guaranteed in the European Convention of Human Rights and the Universal Declaration of Human Rights.
The satellite symposium sessions were well put together, and attracted substantial audiences.
There was an amazing moment when Agnes Houston (@Agnes_Houston), Chair Scottish Dementia Working Group, said to Helga Rohra (@ContactHelga), the Chair of the satellite session and Chair of European Persons With Dementia, “All we people with dementia need is a bit of help — AND A BIT OF TIME!”
A quotation from Agnes – from a previous conference – says it all for me.
The audience burst out laughing.
The reason for this is that Agnes had been originally timetabled to have more time for her slot, apparently.
As the conference was themed around the law, including human rights, invariably discrimination against people with dementia came up in various forms.
I asked about the topic several times.
One talk of the entire programme which I thought was truly outstanding was PL1.3. Gráinne McGettrick (Alzheimer’s Society of Ireland): The UN Disability Convention as an instrument for people with dementia and their carers.
In the English jurisdiction, dementia can count as a disability; therefore there are statutory requirements for ensuring dementia-friendly communities from employers. Also, unfair dismissal of a person on account of being newly diagnosed with dementia will clearly be unlawful.
A member of the audience politely pointed out to me afterwards that a person normally gets sacked first, and then gets his or her diagnosis of dementia confirmed much later, so at the point of dismissal the dismissal does not obviously appear unfair legally.
I found this observation incredibly insightful, as there have been thus far no ‘test cases’ of unfair dismissal on grounds of a diagnosis of dementia in the English jurisdiction.
I asked several times why there is no representative of persons living with dementia or caregivers on the World Dementia Council (@WorldDementia). The background to this fiasco is explained here.
It was by chance we gave a lift to Dr Ruth Bartlett (@RuthLBartlett) to the conference venue. Ruth was staying, as it turns out, in the same competitively-priced hôtel.
Ruth is of course well known for her well respected contributions about the citizenship of of people living with dementia, and how this has influenced the ‘involvement’ of people with dementia in policy.
This was us just before the opening ceremony – when we were full of energy.
I really enjoyed speaking with Geoff Huggins (@GeoffHuggins), who gave an excellent speech in the opening ceremony.
I presented my talk on how dementia healthcare would not be best served by a private insurance system, because of the potential problems of ‘moral hazard’ and genetic discrimination.
This talk was, overall, well received.
I was particularly pleased with the wide-ranging, excellent discussion we had after my talk. Thanks especially to Amy Dalyrymple (@Amy_Dalyrymple), Head of Policy for Alzheimer Scotland, whose contributions in all areas of policy were particularly interesting. The work currently being implemented in Scotland represents a culmination of very high quality inclusive work through a number of different stakeholders.
I was also honoured to present two further research posters, which I had co-authored on the perception and identity of the G8 conference.
Chris Roberts (@mason4233) helped me with the poster session. It was in fact Chris who identified that the phrase “living well with dementia” was not used even once in the top 75 web articles on #G8dementia on Google, in about 44000 words odd.
All around the conference were people whose work is directly relevant to my book: for example Silke Kammer – on the arts and music – and Emma Killick (@RealEmmaKillick) who at the excellent MacIntyre leads on children and adults with learning disabilities and/or autism, but is clearly passionate about people with learning disabilities who later have further unaddressed needs on receiving a diagnosis of dementia.
It was terrific to bump into followers everywhere I went. It was great to meet Julie Christie (@juliechristie1) for the first time, whose work on resilience I am much interested in. It was also lovely to see Anna Tatton (@annatatton1) doing so well.
I happened to meet in the foyer of the Crowne Plaza on Monday night Ann Pascoe, @A_Carers_Voice, somebody who I have not only liked a lot on Twitter, but whose work on rural ‘dementia-friendly communities’ I have massively respected for some time.
Likewise, it was really nice to catch up with Caroline Bartle (@3SpiritUKNZ), who very kindly once did an infographic of my book ‘Living well with dementia’.
I met in the poster session Prof Mary Marshall to whom the Stirling School in design in dementia owes a huge amount. I owe a huge amount to Prof Marshall too, as the Notting Hill masterclass which I once attended got me first interested in this subject a few years ago (I had a long chat with Prof Marshall there.)
There were not idle tokenistic sops to people living with dementia, and their closest ones, in the whole conference. They were at all times integral to the fabric of the conference.
For example, the seating arrangements in the main Argyll conference suite reflected the special respect given to people with dementia and those closest to them.
The substance of the conference for the most part was of an exceptionally high standard in policy; there was next to no shilling of commercial projects.
The work from Alzheimer Scotland (@alzscot), including, predictably, the work focused on autonomy and dignity, and human rights, was showcased in an impressive way. Their work hangs together as a coherent, forceful narrative of meaningful significance for the Scottish jurisdiction.
It also has clear implications for how England conducts itself south of the border, notably, for example, in a right to timely diagnosis, and a right to timely care and support (including proper coordination of care and support).
In common with Scotland, England is trying to tackle hard the inappropriate use of antipsychotics. Dr Karim Saad (@KarimS3D) gave an excellent talk on this subject, drawing on recent findings from the ALCOVE2 study.
Scotland, in fairness, seems to be having less trouble with its policy than England is.
There was a very good sprinkling of cutting-edge research relevant to all practitioners in the field.
For me, the conference had the feeling of a happy wedding without any of the arguments.
Here are Agnes and Donna.
Whilst originally ‘unkeen’, I ended up having a wonderful time at the “Gala Dinner”. The entertainment – traditional Scottish music and dance – was amazing.
I was able to chat with Agnes and Nancy for some time. What a joy.
Elaine Hunter (@ElaineAHPmh) gave an excellent presentation on the transformative changes which had happened around the workforce in Scotland, including leadership from allied health professionals.
Without doubt, a skilled workforce for the provision of dementia services is essential, not gimmicks.
I consider Helga to be a true friend too. Meeting Helga was akin to being wowed by Lady Gaga.
I had last felt like this when I met Norman McNamara (@norrms) at the Queen Elizabeth II centre in London, Westminster.
I learnt a lot from the all-day workshop on building dementia friendly communities.
Over lunchtime, Joy Watson gave a brilliant ‘Dementia Friends’ (@DementiaFriends) session. I, in fact, was total awe as I am also a ‘Dementia Friends Champion’, and discovered many tips how to run my sessions in future!
This is a brilliant film exhibiting the passion which Joy puts into her Dementia Friends sessions.
Chris Roberts made time to hand out flyers for membership of the ‘Dementia Alliance International‘, an unique campaigning group run wholly by people living with dementia.
This Conference mapped topics clearly onto people living with dementia and caregivers, for which the organisers of this event must be heavily congratulated.
Next year’s Conference will be in Slovenia. I’ll be there! Bring it on!
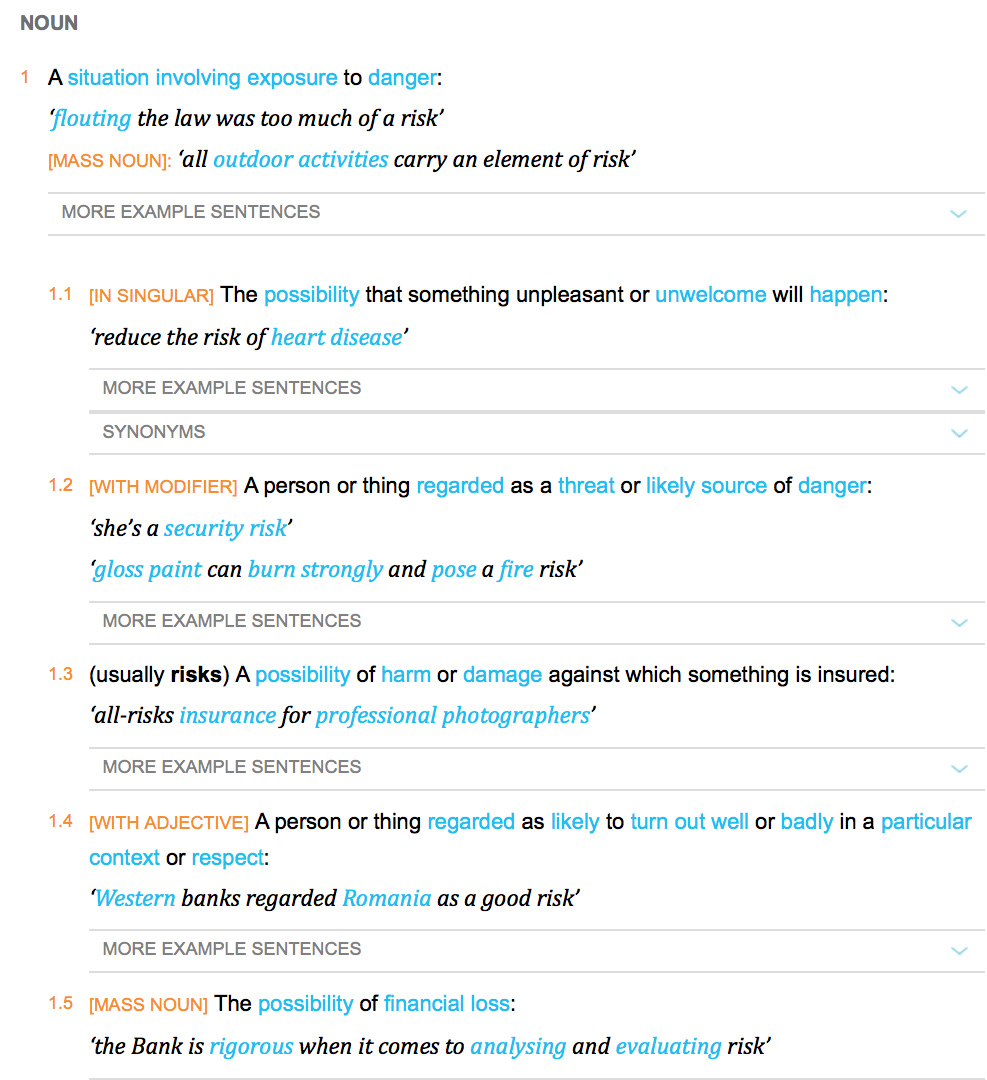
“Risk” is one of those entities which bridges the financial world with law and regulation, psychology or neuroscience. The simplicity of the definition of it in the Oxford English Dictionary rather belies its complexity?
‘You need to break eggs to make an omelette’ is one formulation of the notion that you have to be able to make mistakes to achieve an overall goal. That particular sentence is, for example, used to convey the way in which you might have to put up with ninety nine turkeys before striking gold with one truly innovative idea. ‘Nothing ventured nothing gained’ is another slant of a similar idea. Interestingly, this phrase is often attributed to Benjamin Franklin. Franklin has an established reputation of his own as a ‘conceptual innovator‘.
It’s also a very interesting policy document on risk in dementia from the UK Department of Health, from 10 November 2010, a really useful contribution. This guidance was commissioned on behalf of the Department of Health by Claire Goodchild, National Programme Manager (Implementation), National Dementia Strategy. The guidance was researched and compiled by Professor Jill Manthorpe and Jo Moriarty, of the Social Care Workforce Research Unit, King’s College London.
Prof Alistair Burns, England’s clinical lead for dementia, has written a very focused and relevant Foreword to this piece of work. Here Alistair is, pictured with me earlier this week at the Dementia Action Alliance Annual Conference hosted in Westminster, London (“DAA Conference”). The event was a positive celebration of the #DAACC2A, “Dementia Action Alliance Carers’ Call to Action”, which embodies a movement where, “carers are acknowledged and respected as essential partners in care, and are supported with easy access to the information and the advice they need to assist them in carrying out their role.”
Risk enablement, or as it is sometimes known, positive risk management, in dementia involves making decisions based on different types of knowledge. However, people living with dementia and caregivers, quite often an eldest child or spouse, can handle risk in different ways. I feel that understanding living well with dementia is only possible through understanding the background to a person living with dementia, and his or her interaction with the environment. I’ve indeed written a comprehensive book on it, and I am in the process of writing a second book on it, which brings under the spotlight many of the key stakeholders, I believe, who contribute to “dementia friendly communities”.
Risk enablement is based on the idea that the process of measuring risk involves balancing the positive benefits from taking risks against the negative effects of attempting to avoid risk altogether. For example, the report cites the example of the risk of getting lost if a person with dementia goes out unaccompanied needs to be set against the possible risks of boredom and frustration from remaining inside. There are clearly various components of risk which might affect a person living with dementia. Risk engagement therefore becomes a constructive process of risk mitigation, an idea highly familiar to the law and regulation through the pivotal thrust of ‘doctrine of proportionality‘, that legislation must be both necessary and proportionate.
Risk enablement, it is argued, goes far beyond the physical components of risk, such as the risk of falling over or of getting lost, to consider the psychosocial aspects of risk, such as the effects on wellbeing or self-identity if a person is unable to do something that is important to them, for example, making a cup of tea. Therefore, the report proposes that “risk enablement plans” could be drawn up which summarise the risks and benefits that have been identified, the likelihood that they will occur and their seriousness, or severity, and the actions to be taken by practitioners to promote risk enablement and to deal with adverse events should they occur. These plans need to be shared with the person with dementia and, where appropriate, with his or her carer or caregiver. Thus advancing the policy construct of ‘personalisation’ offering choice and control, risk assessment tools are envisaged by the authors to help support decision making, and should include information about a person with dementia’s strengths and of his or her views and understanding about risk. Risk could apply to making a cup of tea, or going for a walk. We know that people living with dementia handle risks in different ways. For some people, a person living with dementia excessively walking beyond a local jurisdiction might be a known problem. For all the different causes of dementia medically, and for all the different ways in which individuals react to a dementia at different stages of the condition, a person can live with dementia in a sharply distinctive way.
Risk therefore in a hugely meaningful and substantial way has moved away from the “safety first” circles? And it fundamentally will depend on how an unique person living with his or her dementia embraces the environment in reality.
The idea that you need risk to live well with dementia is brought into sharp focus here by Chris Roberts, a friend of mine, speaking at the DAA Conference. I have recently begun to take risks in a highly enjoyable game for my #ipad3, which Chris indeed introduced me to, called, “Real Racing 3″. Here, Chris also talks about the crass way in which he was originally told his diagnosis, and lack of information about his condition given at the time of diagnosis. Therefore, Chris, I feel, brings into sharp focus a number of problem areas, which hopefully Baroness Sally Greengross and colleagues will address in a new five year strategy for England for 2015-20.
There’s been a persistent concern amongst many academics and amongst many persons with dementia themselves that persons with dementia are not at the heart of decision-making in dementia-friendly communities.
Such directors are obviously fluent in how to present such a strategy as elegant marketing, to secure competitive advantage, to make money, so it makes absolute sense for them.
It also makes sense for the Department of Health and the Alzheimer’s Society, who are seeing through the policy of ‘Dementia Friends’ through a sustainable financial arrangement, to see this policy plank politically flourish. With every single newspaper article on dementia now mentioning ‘Dementia Friends’, it is hard to see how this campaign cannot succeed.
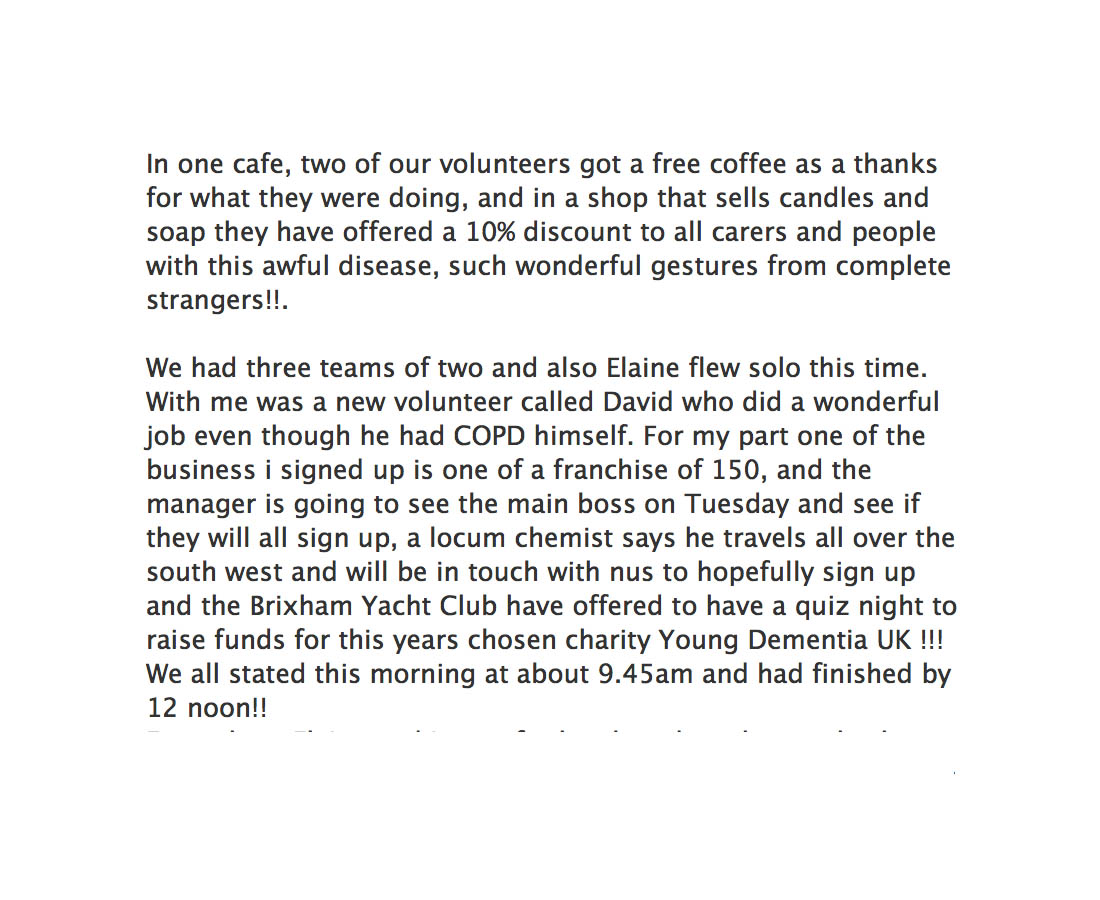
Norman McNamara, an individual campaigning successfully and living with dementia of Lewy Body type, reported yesterday on Facebook local success around the Brixham community area.
“Since being diagnosed, i’ve noticed that there isn’t a lot for people in the mild to moderate stage. There are dementia cafes of course, but these seem to suit carers more than the people with dementia, we just sit there smiling when looked at while our carers and spouses chat away to each other, sharing there experiences and so on.”
“There are 100s of thousands of us in the same positition with nowhere to go or nowhere to be left! We could popin for an hour or for the day. We could practically run the place our selves, some where we could chat and share, watch tv, play cards, draw , we would arrange our own activities not led by someone who thinks they know what we want!”
“Yes we can live with dementia, yes we could even live well ! Yes we could live even better !”
The National Dementia Strategy makes reference to such activities being ‘purposeful‘:
And this gets away from the concept of persons with dementia sitting around calmly doing knitting when they might have been, for example, proficient motorcycle bikers:
When one criticises that persons with dementia are often not at the heart of decision-making, these days I get a standard reply saying, ‘we always take serious note of the opinions of people with dementia; in fact there are two representatives on our board.’
Yet personal feedback which I receive is that persons with dementia resent this “tokenism”.
Having persons with dementia at the heart of decision-making I feel is important in the campaign to overcome stigma and discrimination against persons living with dementia. Persons with dementia running businesses of their own dispels the notion that persons with dementia are incapable of doing anything at all.
As a Fellow of the RSA, I intend to apply for a RSA Catalyst grant, as well as to the Wellcome Trust (who funded my own Ph.D. in decision-making in dementia fewer than 15 years ago now), to investigate collective decision by people in earlier stages of living with dementia to see how they in fact shape their community.
I am hoping that this will be in the context of their ongoing research work with the RSA Social Brain project, and I am hoping to hear from other Fellows about their work there, shortly. I will be putting my grant in with various people who are genuinely interested in this project.