The transfer of an individual living with dementia into a residential setting, at worst, can be associated with an sensorily-unstimulating environment, as well as reduced sensorimotor and cognitive stimulation, social interactions, and physical activity.
Starting from the 1960s, various non-pharmacological treatments for patients with dementia have been proposed, in order to improve cognitive skills and quality of life, to reduce behavioural disturbances and maximise function in the context of existing deficits.
There is a long tradition of psychological therapies for people with dementia, but they had seldomly been rigorously evaluated, making it difficult for commissioners and providers to plan services from a solid evidence base, and also making it difficult to draw comparisons with pharmacological interventions. However, Cochrane reviews on non-pharmacological interventions have previously highlighted the insufficiency of the available evidence.
A recent Cochrane review on cognitive stimulation (Woods et al., 2009) combined the data from nine randomised controlled trials. It found that, oer and above any medication effects, and some studies suggest that the benefits may be maintained for over a year. Recently, Apóstolo and colleagues (2014) reported that cognitive stimulation therapy had significantly improved cognition, explaining the 15.7% variability, but there was no statistical evidence of its effectiveness on depressive symptoms. This improvement was not affected by the baseline level of dependence-independence in activities of daily living.
Conceptualising dementia within the framework of a disability model highlights the distinction between the underlying impairment, resulting from pathological changes, and the resulting limitations on engaging in activity (disability) and restrictions on social participation (handicap).
Cognitive impairment is a defining feature of dementia caused by neurodegenerative conditions including the dementias. Family caregivers are also affected because of the practical impact of cognitive problems on everyday life and the strain and frustration that often result. It has been suggested that rehabilitation provides a useful overarching conceptual framework for the care and support of people with dementia and for the design of interventions to meet their needs. Recreational activities (e.g., crafts, pets) and art therapies (e.g., music, dance, art) have been often proposed as non-pharmacological treatments in dementia, and are widely utilised in residential settings.
Cognition-focused interventions as a group fall under the broader umbrella of non-pharmacological interventions. Cognition-focused interventions can be broadly defined as interventions that directly or indirectly target cognitive functioning as opposed to interventions that focus primarily on all aspects of whole person care – i.e. behavioural, emotional or physical function.
An increasing number of dementia studies describe their intervention as ‘cognitive stimulation’. Clare and Woods (2008) provided a definition which stated that cognitive stimulation:
- targets cognitive and/or social function;
- has a social element — usually in a group or with a family care-giver;
- includes cognitive activities which do not primarily consist of practice on specific cognitive modalities;
- may be described as reality orientation sessions or classes.
Several types of cognition-based interventions have been described. The potential benefits of non-specific stimulation of cognitive functioning for people with dementia have long been recognised. These interventions typically involve engaging the person with dementia in a range of general activities and discussions, are commonly conducted in groups and are aimed at general enhancement of cognitive and social functioning.
Cognitive stimulation typically involves a set of tasks designed to reflect cognitive functions such as attention, memory, language, and problem solving, combined with a reality orientation session. This training takes place in individual or group sessions with a range of difficulty levels. The fundamental assumption is that practice with specific cognitive function tasks may improve, or at least maintain, functioning in a given domain and that any effects of practice will generalise and induce a general improvement of cognitive and social functioning. There is some additional evidence that these interventions can decrease behavioural problems and improve mood. Other authors have also reported positive results for training of basic activities of daily living.
However, some treatment guidelines have been highly critical of cognitive stimulation or training interventions in dementia in view of the risk that cognitive gains may be achieved at the expense of reduced wellbeing and adverse effects.
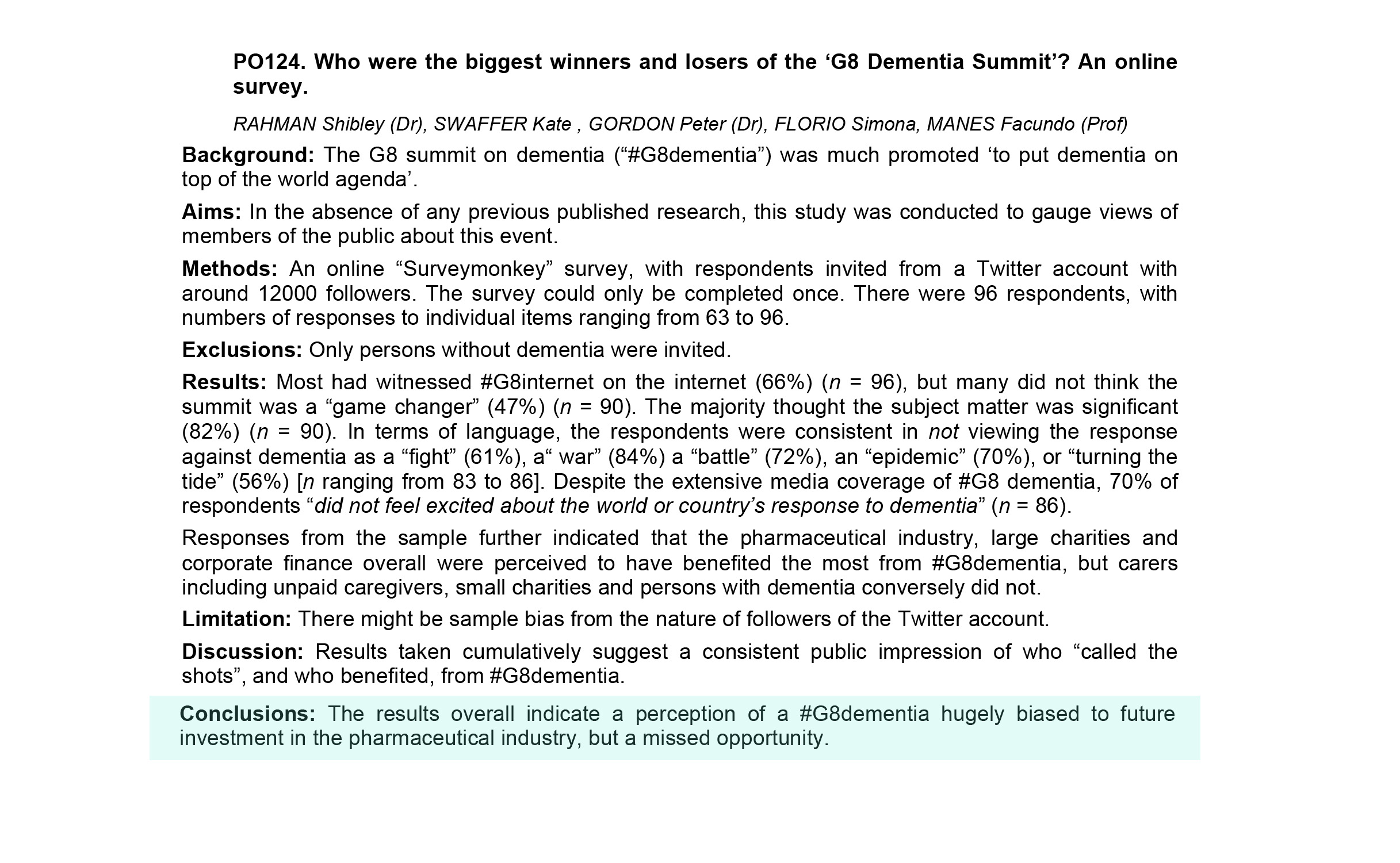
So, the burning question is: if the drugs don’t always work, why don’t we consider more seriously cognitive stimulation therapy? The answer is possibly in large part cultural and social. That is, medical professionals, large charities and the media, in cahoots in Big Pharma, don’t want to give up their traditional power base in treatment. Look for example at Julianne Moore on the red carpet of the Oscars last night talking about how ‘there is no treatment for dementia’. But almost certainly we don’t have that the correct organisational structures in place. There is regulatory capture, which means that drugs can rarely become recommended despite modest effects, but there is virtually no head to head comparison of the cost efficacy or resource allocation consequences of medication vs psychosocial approaches. There is no clear infrastructure subserving ‘social prescribing’, where GPs can easily prescribe such treatments, yet, in England, despite the fact that this could potentially save the NHS a lot of money, and see an improvement in wellbeing in many of its patients.
There are powerful forces at work. You have been warned.
References
Apóstolo JL, Cardoso DF, Rosa AI, Paúl C. The effect of cognitive stimulation on nursing home elders: a randomized controlled trial. J Nurs Scholarsh. 2014 May;46(3):157-66. doi: 10.1111/jnu.12072. Epub 2014 Mar 5.
Clare L, Woods RT. 2004. Cognitive training and cognitive rehabilitation for people with early stage Alzheimer’s disease: a review. Neuropsychol Rehabil 14: 385–401.
Woods B, Spector A, Orrell M, Aguirre E. 2009. Cognitive stimulation for people with dementia (review) The Cochrane Database of Systematic Reviews Chichester: Wiley